A report by The Rt Hon the Baroness Hallett DBE
Chair of the UK Covid-19 Inquiry
Volume I: Introduction and key events from January 2020 to May 2022
Presented to Parliament pursuant to section 26 of the Inquiries Act 2005
Ordered by the House of Commons to be printed 20 November 2025
HC 1436-I
CORRECTION SLIP
Title:
UK Covid-19 Inquiry
Modules 2, 2A, 2B, 2C: Core decision-making and political governance
Volume I: Introduction and key events from January 2020 to May 2022
A report by The Rt Hon the Baroness Hallett DBE
Chair of the UK Covid-19 Inquiry
Session: 2025
HC 1436-I
ISBN: 978-1-5286-5449-4
Ordered by the House of Commons to be printed 20 November 2025
Corrections:
Text currently reads (Chapter 2, para 41):
In Scotland, on 24 January 2020, Ms Sturgeon received a briefing from Health Protection Scotland incorrectly stating: “We now know that people carrying the virus are only infectious to other people when experiencing symptoms.”104 Ms Sturgeon challenged the view that asymptomatic transmission was not possible.105 The following day she received further advice from Health Protection Scotland, which explained that “it is likely that person to person transmission, when it does occur, mostly involves transmission of virus from people with symptoms” and that:
Text should read:
In Scotland, on 24 January 2020, Ms Sturgeon received a briefing from the Scottish Government’s Health Protection Policy Team incorrectly stating: “We now know that people carrying the virus are only infectious to other people when experiencing symptoms.”104 Ms Sturgeon challenged the view that asymptomatic transmission was not possible.105 The following day she received advice from Health Protection Scotland, which explained that “it is likely that person to person transmission, when it does occur, mostly involves transmission of virus from people with symptoms” and that:
Date of correction: 16 January 2026
Text currently reads (Chapter 3, para 16):
Richard Pengelly, Permanent Secretary to the Department of Health (Northern Ireland) from July 2014 to April 2022, had written to the Chief Executives of health and social care trusts on 1 March 2020, warning them that:
Text should read:
Richard Pengelly, Permanent Secretary to the Department of Health (Northern Ireland) from July 2014 to April 2022, had written to the Chief Executives of health and social care trusts on 26 March 2020, warning them that:
Date of correction: 16 January 2026
| Figure | Description |
|---|---|
| Figure 1 | Message from Mr Hancock to Mr Cummings, 25 January 2020 |
| Figure 2 | Reported cases in selected European countries in February 2020 |
| Figure 3 | Daily confirmed cases from 1 to 12 March 2020 across the UK |
| Figure 4 | Exchange of messages between Mr Cummings and Mr Gove on 4 March 2020 |
| Figure 5 | Exchange of messages between Mr Cummings and Mr Gove on 11 March 2020 |
| Figure 6 | Daily confirmed cases from 2 March to 23 March 2020 across the UK |
| Figure 7 | Notes on a whiteboard during the meeting at 10 Downing Street on 13 March 2020 |
| Figure 8 | Notes on a whiteboard during the meeting at 10 Downing Street on 14 March 2020 |
| Figure 9 | Message from Mr Cummings to Mr Johnson on 14 March 2020 |
| Figure 10 | Message from Mr Cummings to Mr Johnson on 15 March 2020 |
| Figure 11 | Notes on a whiteboard during a ministerial meeting on 15 March 2020 |
| Figure 12 | Daily confirmed cases from 2 to 23 March 2020 across the UK |
| Figure 13 | Daily confirmed cases from 1 March to 30 April 2020 across the UK |
| Figure 14 | Daily deaths per 100,000 population by date of death from 23 March to 13 July 2020 across the UK |
| Figure 15 | Five tests for adjusting the lockdown, 16 April 2020 |
| Figure 16 | UK government steps of adjustment to current social distancing measures |
| Figure 17 | Daily deaths per 100,000 population by date of death from 6 July to 28 December 2020 across the UK |
| Figure 18 | Increase in infections in Northern Ireland from 1 September to 1 October 2020 |
| Figure 19 | Alert levels in Wales, December 2020 |
| Figure 20a | Tiers in England from 20 December 2020 |
| Figure 20b | Tiers in England from 26 December 2020 |
| Figure 20c | Tiers in England from 31 December 2020 |
| Figure 21 | Revised rules for Christmas 2020 |
| Figure 22 | UK Covid-19 statistics at 31 December 2020 |
| Figure 23 | Estimated percentage of the population testing positive |
| Figure 24 | UK Covid-19 statistics at 15 February 2021 |
| Figure 25 | Steps in the COVID-19 Response – Spring 2021 roadmap, February 2021 |
| Figure 26 | Extract from Moving Forward: The Executive’s Pathway out of Restrictions |
| Figure 27 | Vaccine doses across the UK, as at 21 February 2021 |
| Figure 28 | Step 3, COVID-19 Response – Spring 2021 roadmap |
| Figure 29 | Estimated percentage of the population testing positive for Covid-19 from 1 May to 31 July 2021 across the UK |
| Figure 30 | Step 4, COVID-19 Response – Spring 2021 roadmap |
| Figure 31 | Alert levels in Wales in the summer of 2021 |
| Figure 32 | Estimated percentage of the population testing positive for Covid-19 from 1 August to 31 October 2021 across the UK |
| Figure 33 | Estimated percentage of the population testing positive for Covid-19 from 31 October to 31 December 2021 across the UK |
| Figure 34 | Daily deaths per 100,000 population by date of death from 31 October to 31 December 2021 across the UK |
| Figure 35 | Plan B measures announced on 8 December 2021 |
| Figure 36 | Estimated percentage of the population testing positive for Covid-19 from 1 December 2021 to 1 June 2022 across the UK |
| Figure 37 | Daily deaths per 100,000 population by date of death from 1 December 2021 to 1 June 2022 across the UK |
| Figure 38 | Cumulative daily deaths per 100,000 by date of death from May 2021 to May 2022 across the UK |
| Table | Description |
|---|---|
| Table 1 | Summary of potential response strategies |
| Table 2 | Interventions considered by SAGE (presented by the Cabinet Secretariat to COBR on 12 March 2020) |
| Table 3 | The rule of six by nation, September 2020 |
| Table 4 | Combined estimate of R and the growth rate in the UK, four nations and English NHS regions, 23 September 2020 |
Introduction by The Rt Hon the Baroness Hallett DBE
The Covid-19 virus spread around the world rapidly and caused untold misery and suffering. The number of deaths across the UK for which the virus was responsible – calculated by whether Covid-19 is mentioned on the death certificate – is now over 230,000. This appalling loss of life resulted from the virus spreading across the UK in three successive waves. The devastating socio-economic consequences resulted both from the virus and from the decisions taken to respond to it.
This, the second report of the UK Covid-19 Inquiry, focuses on those decisions.
As democratically elected leaders, politicians were entitled to draw their own conclusions as to how to balance the ethical, public health, social and economic challenges posed by Covid-19. In this Report, I have considered whether their decisions were reasonable and justifiable in light of the information that was then known, or which ought to have been known, to determine if things could have been done better and to learn lessons for the future.
In doing so, I bear very much in mind that, in trying to stem the spread of the virus, politicians in the UK government and devolved administrations were faced with unenviable choices. There were few, if any, easy decisions for them to make. The decisions to impose stringent social restrictions, including most obviously the lockdown decisions, gave rise to agonising dilemmas and were highly controversial. They were also taken under conditions of extreme pressure and often without access to data or a full understanding of the epidemiological position. Such an understanding is vital to any response to a pandemic.
Most importantly, politicians across the UK found themselves having to take decisions in the context of the UK lacking resilience and being ill prepared.
In its first report, relating to Module 1 on the resilience and preparedness of the UK, the Inquiry examined the state of the UK’s central structures and procedures for pandemic emergency preparedness, resilience and response. It concluded that the UK was ill prepared for dealing with a catastrophic emergency, let alone the coronavirus pandemic that actually struck. In particular, it found that there were fatal strategic flaws underpinning the assessment of the risks faced by the UK. The UK government’s sole pandemic strategy, from 2011, was outdated and lacked adaptability.
As a result, there was a damaging absence of focus on the measures, interventions and infrastructure required in the event of a pandemic – in particular, a system that could be scaled up to test, trace and isolate. The Inquiry recommended fundamental reform of the way in which the UK government and devolved administrations prepare for whole-system civil emergencies.
Such reform is vital. Had the UK been better prepared, fewer lives would have been lost, the socio-economic costs would have been substantially reduced and some of the decisions politicians had to take would have been far more straightforward.
The decisions that politicians were forced to take were further complicated by the UK devolution settlements. This was primarily a health emergency and health is a devolved matter, but three of the nations of the UK form a single epidemiological unit (Great Britain). The other, Northern Ireland, forms an epidemiological unit with the Republic of Ireland. Whatever steps each government took, they were bound to be affected by the decisions taken elsewhere in the UK and by constant cross-border travel. In addition, the devolved administrations were generally reliant on the UK government for funding to support their emergency response.
Initially, the UK government and devolved administrations followed the same path in responding to the pandemic but, in the summer of 2020, they began to diverge. This might not have been surprising, given the devolution settlement and the different characteristics of the four nations, but it did lead to difficulties for the people of the UK as they sought to comply with restrictions that varied around the UK – and it caused political controversy. This Report will examine those differences in approach and, where appropriate, compare them.
Some past public inquiries have provided definitive accounts of every aspect of the particular disaster, tragedy, other momentous event or government policy into which they were charged to inquire. However, as I observed in the Introduction to the Inquiry’s first report, the Covid-19 pandemic – and the response to it from the UK government and devolved administrations – was the most complex and multi-layered emergency to have struck the UK in peacetime. No inquiry, however large or however long, could possibly or sensibly inquire into every part of it. This Report does not seek to address every relevant decision or provide a historical record of everything that happened. It is focused on the key issues and decisions taken during the almost two and a half years of the pandemic, in order to identify the critical lessons to be learned for future pandemics or other civil emergencies.
Other modules of this Inquiry and their reports will consider specific aspects of the governments’ response in more detail. At the time of publication of this Report, there have been public hearings in Module 3 (Impact of the Covid-19 pandemic on healthcare systems in the four nations of the UK), Module 4 (Vaccines and therapeutics), Module 5 (Procurement), Module 6 (Care sector), Module 7 (Test, trace and isolate) and Module 8 (Children and young people). Hearings will take place shortly in relation to Module 9 (Economic response) and Module 10 (Impact on society, which has a particular focus on key workers, the most vulnerable, the bereaved, mental health and wellbeing).
The speed and thoroughness with which the momentous events and decisions have been examined, from the emergence of Covid-19 in January 2020 until the final restrictions were lifted in May 2022, reflect a mammoth undertaking for the Module 2 (UK government), 2A (Scottish Government), 2B (Welsh Government) and 2C (Northern Ireland Executive) teams.
During the investigation phase, there was an extensive and complex process of obtaining more than 2 million potentially relevant documents from a wide range of sources. This material was then examined by the Inquiry team and in excess of 180,000 documents were deemed to be relevant. These were disclosed to the 53 Core Participants to assist them in their preparation for the public hearings, which took place over 69 days and during which 166 witnesses were examined.
This reflects the enormously hard work of a large number of people, and I wish to express my gratitude to all those who have given so much of their time and resources to assisting the Inquiry. In particular, I am very grateful to the Core Participants and their legal teams, especially the groups representing bereaved people, for their helpful contributions to the Inquiry process. I would also like to thank the teams (both secretariat and legal) in Modules 2, 2A, 2B and 2C, without whose hard work, diligence and dedication the hearings and this Report would not have been possible.
Finally, I should like to thank those who have given evidence and those who have contributed to the Inquiry’s listening exercise, Every Story Matters, and to the moving films played at each hearing about the impact of the Covid-19 pandemic on them and their loved ones. They have shown great courage. Their accounts not only help me and inform the Inquiry’s work, but also serve as a constant reminder of why the work of this Inquiry is so important.

The Rt Hon the Baroness Hallett DBE
20 November 2025
Voices
Five days after Daddy went into hospital we had to get the police to break into my mum’s house because she was unconscious in bed. She was rushed to the same hospital and she would test positive when she got there. My dad died on the 10th of May. The day we buried Daddy, we were waiting for a phone call because that was the day they thought Mummy was going to die. But she died the next day. So we buried them three days apart.”¹
I feel that my mother was getting more and more nervous going into the second lockdown. I feel the Government were on TV every day talking about all these different things and there was no equality for her as an elderly lady. The elderly were not considered. It was a case of ‘keep away from the elderly and vulnerable to protect them’ meanwhile other people were in and out of each other’s bubbles and houses. There was no consideration for the elderly. I feel they were just numbers. My mum caught covid and died in the hospital.”²
[My mother] said ‘No I’m too afraid to go to the hospital, you know, if i haven’t got it and it’s just a really, really bad flu, then I’m going to end up with it, I don’t want to be on my own’ she said. So she was too afraid to go to the hospital.”³
I think I immediately found it very difficult to grieve. Not in the traditional sense, in terms of the funeral, obviously that was not available to us but I found it very hard emotionally to feel the – to go through the natural emotional process of grieving, because I think what was blocking me was that I felt very strongly that his death was not an inevitability.”⁴
Executive summary
This Report concerns the core political and administrative decision-making across the UK in response to the Covid-19 pandemic, drawing on the work of four of the Inquiry’s modules: Module 2 (UK), Module 2A (Scotland), Module 2B (Wales) and Module 2C (Northern Ireland). This has provided the Inquiry with the opportunity to compare and contrast the different choices made by the four governments in responding to the same emergency and to identify the most important lessons for responding to future UK-wide emergencies.
The Inquiry finds that the response of the four governments repeatedly amounted to a case of ‘too little, too late’. The failure to appreciate the scale of the threat, or the urgency of response it demanded, meant that – by the time the possibility of a mandatory lockdown was first considered – it was already too late and a lockdown had become unavoidable. That these same mistakes were repeated later in 2020 is inexcusable. While the nationwide lockdowns of 2020 and 2021 undoubtedly saved lives, they also left lasting scars on society and the economy, brought ordinary childhood to a halt, delayed the diagnosis and treatment of other health issues and exacerbated societal inequalities. The Covid-19 lockdowns only became inevitable because of the acts and omissions of the four governments. They must now learn the lessons of the Covid-19 pandemic if they are to avoid lockdowns in future pandemics.
Key events from January 2020 to May 2022
The emergence of Covid-19 (Chapter 2)
The initial response to the pandemic was marked by a lack of information and a lack of urgency. When the first cases of Covid-19 had been confirmed outside China, the significant degree of scientific uncertainty – in particular, whether there was sustained person-to-person transmission and whether the virus could be transmitted by individuals without symptoms (asymptomatic transmission) – meant that the level of risk that the virus posed was not fully appreciated.
Once the scientific community and the scientific advisers for each nation became aware that the virus had spread from China, and that it was causing substantially more cases of moderate or severe respiratory illness in China than were being officially reported, the tempo of the response should have been increased and threat levels raised.
By the end of January 2020, when thousands of cases had been identified outside China and the first few cases of Covid-19 had been confirmed in the UK, it should have been clear that the virus posed a serious and immediate threat. However, the limited testing capacity in the UK and a lack of adequate surveillance mechanisms, combined with a failure to assume that there was asymptomatic transmission, meant that decision-makers did not appreciate the extent to which the virus was spreading undetected.
The political system across the four nations lacked urgency and treated the emerging threat as predominantly a health issue. The obviously escalating nature of the crisis made it surprising that COBR, the UK government’s crisis coordination committee, was not chaired by the Prime Minister, Boris Johnson MP, until 2 March 2020 and that neither COBR nor the UK Cabinet met during the half-term holidays in mid-February 2020. Mr Johnson should have appreciated sooner that this was an emergency that required prime ministerial leadership to inject urgency into the response. Mr Johnson’s own failure to appreciate the urgency of the situation was due to his optimism that it would amount to nothing, his scepticism arising from earlier UK experiences of infectious diseases, and, inevitably, his attention being on other government priorities. This was compounded by the misleading assurances he received from the Cabinet Office and the Department of Health and Social Care that pandemic planning was robust, as well as the widely held view that the UK was well prepared for a pandemic. As the pandemic unfolded, the Secretary of State for Health and Social Care, Matt Hancock MP, gained a reputation among senior officials and advisers at 10 Downing Street for overpromising and underdelivering.
The devolved administrations similarly failed to engage with the threat posed to their nations and were overly reliant on the UK government to lead the response. Covid-19 received no attention in Welsh Cabinet meetings before 25 February 2020. After the first case was identified in Wales on 28 February, the First Minister of Wales, Mark Drakeford MS, chose to attend St David’s Day celebrations in Brussels rather than the Welsh Cabinet meeting on 4 March 2020. In Northern Ireland and in Scotland, Covid-19 was only discussed under ‘any other business’ in meetings as late as 24 and 25 February respectively. It should have been equally apparent to the First Ministers and deputy First Ministers of the devolved administrations that, by this point, Covid-19 was the most pressing issue facing their governments.
Ministers and officials in the UK government had been given clear advice that, in the reasonable worst-case scenario, up to 80% of the population would be infected – with a very significant loss of life – but did not appreciate the increasing likelihood of this scenario materialising. At the same time, it was clear that the test and trace system was inadequate for a pandemic. The lack of urgency on the part of all four governments, and the failure to take more immediate emergency steps, are inexcusable.
The spread of the virus globally and, in particular, the escalating crisis in Italy were clear warning signs, which should have prompted urgent planning across the four nations. Instead, the governments did not take the pandemic seriously enough until it was too late. February 2020 was a lost month.
The first UK-wide lockdown (Chapters 3 and 4)
The Coronavirus: Action Plan, published on 3 March 2020, outlined the initial plan to respond to Covid-19, first by ‘containing’ its spread through testing, contact tracing and isolation of infected individuals, and then by ‘delaying’ its spread through introducing restrictions such as social distancing. Based on the strategy for pandemic influenza, the plan made a similar assumption that it would only be possible to slow, rather than prevent, the spread of the virus.
This approach was expected to lead to a degree of population immunity (otherwise known as ‘herd immunity’), where the spread of the virus through the population reduced its vulnerability to further infections. Despite a lack of clarity in media appearances, the UK government’s strategy was not to encourage the spread of the virus with the aim of achieving population immunity sooner – rather, population immunity was seen as the eventual outcome of an inevitable and widespread wave of infections.
At this stage, the Scientific Advisory Group for Emergencies (SAGE) was advising the UK government that restrictions should not be introduced until the spread of the virus was nearer its peak. This was driven partly by concerns about the negative social and economic consequences of introducing restrictions and wanting to minimise the amount of time such restrictions were in place, but also by concerns expressed by Professor (later Sir) Christopher Whitty (Chief Medical Officer for England) and Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser, that the public would not maintain compliance with restrictions over a long period. This concept of ‘behavioural fatigue’ had no grounding in behavioural science and proved damaging, given the imperative to act more decisively and sooner.
It is clear that the Coronavirus: Action Plan was already out of date by the time it was published. Containment had failed, as belatedly recognised by the UK government. Although there were only 39 official cases of Covid-19 in the UK by this point, the known lack of capacity for testing meant that this was clearly a significant underestimate. As the country moved to the ‘delay’ stage, from 13 March 2020, anyone with coronavirus symptoms was advised to self-isolate at home for at least seven days. However, this first restriction was too little, too late.
The lack of testing capacity had, by this point, resulted in the stopping of community testing. This meant that the UK government and devolved administrations had no real understanding of the spread of the virus in the community. Some scientists – and some civil servants and advisers within the UK government – were increasingly alarmed by the lack of urgency and the failure to act more robustly. It became clear that any opportunity to get on top of Covid-19 had been lost.
Friday 13 March 2020 was a watershed moment in the UK’s response. SAGE had concluded that the number of cases was several times higher than its previous estimates and that there were potentially thousands of cases occurring each day. The pandemic was moving faster than previously anticipated, and modelling indicated that the capacity of the NHS would be overwhelmed by the scale of infection, even if self-isolation and social distancing measures were introduced. If NHS capacity were to become overwhelmed, then far higher numbers of people would die from being unable to access medical treatment, both for Covid-19 and for other medical conditions. The plan to wait to implement restrictions until nearer the peak of the virus was no longer sustainable.
Over the next few days, decision-makers concluded that stringent measures were needed to reverse the growth of the virus. The focus remained on a package of advisory measures including self-isolation, household quarantine and social distancing. The advisory measures came into effect from 16 March 2020 and became increasingly stringent in the subsequent days, with the closure of schools and hospitality businesses from 20 March.
By 23 March 2020, SAGE estimated that the number of cases was doubling every three to four days and intensive care units in London were on track to reach capacity within ten days. Almost 300 people had died, with more than 100 of those deaths occurring in the previous two days. The situation was rapidly escalating and it was not clear that the advisory measures in place would be sufficient to prevent the NHS from being overwhelmed. A mandatory lockdown had become unavoidable.
The measures announced on Monday 16 March 2020, and strengthened through the week with the closure of schools and hospitality, should have been implemented much sooner. Had more stringent restrictions, short of a ‘stay at home’ lockdown, been introduced earlier than 16 March – when the number of Covid-19 cases was lower – the mandatory lockdown that was imposed might have been shorter or conceivably might not have been necessary at all. At the very least, there would have been time to establish what effect the restrictions had on levels of incidence and whether there was a sustained reduction in social contact. However, with measures not introduced sooner, a mandatory lockdown was the only viable option left.
The Inquiry recognises that the lockdown decision was as difficult a decision as any UK government or devolved administration has ever had to make. However, the Inquiry accepts the consensus of the evidence before it that the mandatory lockdown should have been imposed one week earlier. Had a mandatory lockdown been imposed on or immediately after 16 March 2020, modelling has established that the number of deaths in England in the first wave up until 1 July 2020 would have been reduced by 48% – equating to approximately 23,000 fewer deaths.
However, the Inquiry rejects the criticism that the four governments were wrong, in principle, to impose a lockdown. In any event, the UK government and devolved administrations had received clear and compelling advice by this time that the exponential growth in transmission would, in the absence of a mandatory lockdown, likely lead to loss of life on a scale that was unconscionable and unacceptable. No government, acting in accordance with its overarching duty to preserve life, could ignore such advice or tolerate the number of deaths envisaged. The governments acted rationally in taking the ultimate step, a mandatory lockdown, in the genuine and reasonable belief that it was required. Nevertheless, it was only through their own acts and omissions that the four governments had made such a lockdown inevitable.
Exiting the first lockdown (Chapter 5)
Upon entering the first lockdown, neither the UK government nor the devolved administrations had a strategy for when or how they would exit the lockdown. These considerations should have been at the forefront of decision-makers’ minds from the moment imposing a lockdown was contemplated. Up until this stage, the four governments had acted in unison, with the same measures applying across the whole of the UK, but they each devised their own approaches to ending the lockdown.
The easing of the majority of restrictions in England took place on 4 July 2020, despite Mr Johnson being informed by scientific advisers that this was an inherently high-risk approach as it would create an environment where infections could grow more quickly and overwhelm the ability of test and trace systems to control further outbreaks. A more cautious approach should have been taken by the UK government. Mr Johnson acknowledged that a second lockdown would be a disaster, but the approach to releasing restrictions increased the risk of this being necessary.
In contrast, the governments of Wales, Scotland and Northern Ireland adopted a more gradual approach to the relaxation of restrictions throughout the summer of 2020. This more cautious approach was taken in the context of different epidemiological circumstances, but created a greater prospect of further lockdowns not being necessary or, if they were, of them not being necessary for so long. However, as there was nothing to prevent people resident in England from travelling across the internal borders of the UK, the approach adopted by the UK government risked undermining the effectiveness of the more cautious responses of the devolved administrations.
Nonetheless, in each of the four governments, insufficient attention was given to the prospect of a second wave of the virus, with only limited contingency planning in place for reintroducing restrictions if a second wave emerged.
The second wave (Chapters 6 and 7)
In the autumn of 2020, infection rates varied significantly across the UK, leading to more significant divergence in approach as all four governments tried to manage the increasing case rates at a local level. The UK government, Welsh Government and Northern Ireland Executive had all failed to learn from the experiences of the first lockdown. Local restrictions were introduced too late, were not in place for long enough or were too weak to control the spread of the virus.
Ministers are required to weigh up all competing factors in their decision-making and do not always need to follow scientific advice. However, the reasons for rejecting scientific advice – and the implications of doing so – must be clearly understood.
Throughout September and October 2020, Mr Johnson repeatedly changed his mind on whether to introduce tougher restrictions and failed to make timely decisions. For those restrictions that were introduced, such as the ‘rule of six’, SAGE had warned that they were unlikely to be effective, but Mr Johnson continued to reject SAGE’s advice to implement a ‘circuit breaker’ lockdown. The weakness of the restrictions used and Mr Johnson’s oscillation enabled the virus to continue spreading at pace, and ultimately resulted in a four-week lockdown from 5 November 2020.
Mr Johnson should have ordered the imposition of a circuit breaker lockdown in late September or early October 2020. Had a circuit breaker been utilised at that time, the second lockdown in England could have been reduced in length and severity – and might conceivably have been avoided altogether. In the event – with the opportunity to regain control having been lost – the second lockdown should have been imposed more quickly. Unlike the circuit breaker or ‘firebreak’ restrictions in Wales and the circuit breaker restrictions in Northern Ireland, the second England-wide lockdown was not timed to coincide with the school half-term holidays. Schools did, however, remain open.
The Welsh Government’s approach of targeted local restrictions was ultimately unsuccessful and led to the imposition of the firebreak. Despite receiving clear advice on 5 October 2020 that the reproduction number (the average number of people that one person with a disease infects) was above 1 and that further restrictions were needed to avoid hospital capacity being exceeded, modelling of the proposed firebreak was not sought until 11 October and the firebreak was not implemented until 23 October. From August to December 2020, Wales had the highest age-standardised mortality rate of the four nations. It is likely that this was the result of a combination of failed local restrictions, imposing the firebreak too late and the decision to relax measures more quickly than scientists advised.
Notwithstanding the imposition of circuit breaker restrictions, the decision-making in Northern Ireland was chaotic. Despite having been advised that a six-week intervention was required, the Northern Ireland Executive Committee opted for a four-week circuit breaker, which commenced on 16 October 2020. This ultimately proved inadequate. In the weeks that followed, Executive Committee meetings were deeply divided along political lines and beset by leaks, leading to an incoherent approach in which the circuit breaker restrictions were extended for one week, then lapsed for one week, before being reintroduced for two further weeks – with the one-week lapse in restrictions correlating with a 25% increase in cases.
The number of cases in Scotland in the autumn of 2020 did not reach the peaks experienced in the rest of the UK. By swiftly using stringent, locally targeted measures to deal with outbreaks, case numbers grew much more gradually and the need for a nationwide lockdown in the autumn was avoided.
Although it was not formally identified until December 2020, the more transmissible Alpha variant emerged in Kent during the autumn and drove a rapid rise in cases. The emergence of a more transmissible variant was entirely foreseeable, but all four governments failed to take decisive action in response. Rather than recognising the threat early on and introducing measures to control the virus, the governments continued to press on with plans for relaxing measures over Christmas while cases grew rapidly, only to change course on 19 December when levels of infection became critical. The mistakes of February and March 2020 were repeated – the failure to take sufficiently decisive and robust action in response had created a situation in which a return to lockdown restrictions had once again become unavoidable.
The vaccination rollout and Delta and Omicron variants (Chapters 7 and 8)
In December 2020, the UK was the first country in the world to approve a vaccine and commence a vaccination programme for Covid-19. On 2 December, temporary authorisation was granted by the Medicines and Healthcare products Regulatory Agency for the Pfizer/ BioNTech vaccine and the vaccine rollout commenced on 8 December. Authorisation for the Oxford/AstraZeneca vaccine swiftly followed on 30 December and the Moderna vaccine on 8 January 2021. This was a remarkable achievement and a decisive turning point in the pandemic.
This development enabled the four governments to take a different approach in their plans to exit their respective lockdowns, balancing the scale of infection against the additional protection from serious illness now being offered by vaccines. Plans were led by data rather than fixed dates and when the Delta variant emerged in March 2021, all four governments sensibly heeded the scientific advice to delay the planned relaxation of restrictions to allow time for the vaccine rollout to progress further. In this respect, the four governments had learned from the experience of earlier lockdowns.
Although the Omicron variant that emerged in the winter of 2021 was a less severe variant, it was much more transmissible and an estimated 5 million people in the UK were infected at the peak of the Omicron wave. Despite the enhanced protection offered by the vaccine rollout, the sheer volume of cases still led to more than 30,000 people dying with Covid-19 in the UK between November 2021 and June 2022. By the time the Omicron variant was identified, all adults had been offered two doses of the vaccine and the programme of booster doses was sensibly accelerated to offer further protection against serious illness and hospitalisation.
The approach of all four governments in the second half of 2021 carried with it an element of risk. The potential for a variant that escaped the immunity conferred by prior infection or by vaccination had been repeatedly identified as the biggest strategic risk. The sheer number of infections demonstrates that, if the vaccines had been less effective or the Omicron variant as severe as previous variants in terms of morbidity and mortality, the consequences would have been disastrous.
Key themes
Scientific and technical advice (Chapter 9)
SAGE provided high-quality scientific advice at extreme pace throughout the pandemic, but some aspects of its operation were strained by the breadth and duration of the response. There was no systematic process in place to ensure that it provided sufficient breadth of scientific expertise: participants were recruited through existing networks and professional connections, relying on people who were able to free up time from their normal jobs. Initially, there was also no clear process for the devolved administrations to gain access to SAGE discussions and advice. As the pandemic progressed, the devolved administrations used their own existing advisory scientific committees or set them up. These fed information into SAGE while applying their advice to their own local circumstances.
The effectiveness of SAGE’s advice was also constrained by the limited information provided by the UK government on its overall objectives when advice was commissioned, which made it harder for SAGE to place its advice in the right context. This lack of clearly stated objectives contributed to the conservatism of SAGE’s advice in early 2020, with participants not believing that lockdowns would be a palatable policy response and, therefore, not modelling its implications until mid-March 2020.
More significant concerns were raised about the quality of economic modelling during the pandemic. Although structures for providing economic advice were set up in Wales and Scotland, there was little evidence in each of the four nations of substantive economic modelling and analysis being provided to decision-makers. This inevitably hampered the ability of decision-makers to assess and balance relative harms.
The process for providing advice on the economic and social implications of decisions was also much more opaque than that for scientific advice. The lack of transparency of this economic and social advice, together with the repeated use of ‘following the science’ and similar phrases in communications to the public, gave a misleading impression that decisions were being taken solely on the basis of advice from SAGE. This impression may have contributed to the wholly unacceptable hostility, threats and abuse to which some experts were subject. The Inquiry strongly condemns such behaviour.
Vulnerabilities and inequalities (Chapter 10)
Although the pandemic affected everyone in the UK, the impact was not shared equally. Older people, disabled people and some ethnic minority groups faced a higher risk of dying from Covid-19. For example, when taking into account age, people from a Black African and Black Caribbean background had the highest rates of mortality during the first wave of the pandemic. From the second wave onwards, the highest mortality rates were among people of an Asian or Asian British background. The increased risk of harm was also strongly influenced by socio-economic factors, with people living in overcrowded housing or working in low-paid employment at higher risk. This often overlapped with other factors such as ethnicity.
Vulnerable groups were also affected by the restrictions introduced to control the virus. The vast majority of children were not at risk of serious direct harm from Covid-19, but suffered greatly from the closure of schools and requirement to stay at home, and the consequent loss of interaction with friends and family and limited access to play. Children were not always prioritised. No government in the UK was adequately prepared for the sudden and enormous task of educating most children in their homes and failed sufficiently to consider the consequences of school closures for children’s education and physical and mental health. Module 8 is examining these issues in more detail.
Despite this harm being foreseeable, the impact on vulnerable groups had not been adequately considered in pandemic planning, and the existing mechanisms for assessing the impact of decisions were largely applied retrospectively. Decision-makers consequently had little understanding of the impact of restrictions on vulnerable groups.
Government decision-making (Chapter 11)
COBR is designed to deal with acute emergencies and proved inadequate for responding to a prolonged pandemic. While the COBR mechanism is appropriate for assessing the initial UK-wide response to an emergency, a clearer plan for how each government will make key decisions in a prolonged emergency is needed.
The UK Cabinet was largely sidelined in decision-making, albeit that as the pandemic progressed the coordination of advice and decision-making improved and became more formalised through the Covid-19 Strategy Committee (Covid-S) and Covid-19 Operations Committee (Covid-O) and the supporting Covid-19 Taskforce. Mr Johnson’s hospitalisation in April 2020 also exposed the lack of formal arrangements for covering the absence of a Prime Minister.
Decision-making authority in the Scottish Government rested with a small group of ministers throughout the pandemic. Although the First Minister of Scotland, Nicola Sturgeon MSP, was a serious and diligent leader who took responsibility for decisions, that also meant that ministers and advisers were often excluded from decision-making. The use of the informal Gold Command meeting structure diminished the role of the Scottish Cabinet, which frequently became a decision-ratifying body and not the ultimate decision-making body.
By contrast, the Welsh Cabinet was fully engaged throughout the pandemic, with decisions mostly being made through consensus. Mr Drakeford was recognised by his ministers as a careful and considered leader. He maintained positive relationships throughout the response.
The power-sharing arrangements in Northern Ireland are designed to ensure that each department has a significant degree of operational independence and individual ministers are afforded significant autonomy. This weakened the ability of the Northern Ireland Executive to coordinate the pandemic response and there was no one sufficiently empowered to hold departments to account. The Department of Health (Northern Ireland), which was the lead government department with responsibility for the response at the outset of the pandemic, largely operated in a silo – especially in the early stages of the response. The Northern Ireland Executive had only recently re-formed in January 2020, following a three-year period during which power-sharing was suspended, and it is unclear how decisions usually subject to ministerial approval would have been made in Northern Ireland had power-sharing still been suspended when lockdown decisions were taken.
The distinct power-sharing arrangements in Northern Ireland offered the opportunity to demonstrate that decisions were being made by all parties collectively for the greater good. Instead, however, on multiple occasions decision-making was marred by political disputes between Democratic Unionist Party and Sinn Féin ministers. The attendance of the deputy First Minister of Northern Ireland, Michelle O’Neill MLA, at the funeral of Bobby Storey in June 2020, and her initial refusal to apologise for this, contributed to tensions in the Northern Ireland Executive Committee. The four-day Executive Committee meeting from 9 to 12 November 2020 represented a low point in Northern Ireland politics during the pandemic. The confidentiality of discussions was undermined by leaks and there was inappropriate instigation of cross-community votes to make political points by the First Minister of Northern Ireland, Arlene Foster MLA (later Baroness Foster of Aghadrumsee).
The pandemic response also exposed wider cultural issues. The very least the public should be entitled to expect is that those making the rules will abide by them. Instances where ministers and advisers appeared to break Covid-19 rules caused huge distress to the public. This was especially the case for people who had endured huge personal costs to stick to the rules, with many bereaved people unable to be with their loved ones when they died. Instances where rule-breaking was not swiftly addressed also undermined public confidence and increased the risk of people not complying with the rules designed to protect them.
Decision-making was particularly affected by cultural problems in the UK government and Northern Ireland Executive. There was a toxic and chaotic culture at the centre of the UK government during the pandemic, with the Inquiry hearing evidence about the destabilising behaviour of a number of individuals – including Dominic Cummings, an adviser to the Prime Minister. By failing to tackle this chaotic culture – and, at times, actively encouraging it – Mr Johnson reinforced a culture in which the loudest voices prevailed and the views of other colleagues, particularly women, often went ignored, to the detriment of good decision-making.
Public health communications (Chapter 12)
Communication with the public is a critical aspect of a pandemic response, since controlling the virus is dependent on members of the public understanding the risk they face and acting accordingly. The ‘Stay Home’ communications campaign was effective at maximising compliance with the first lockdown, at a time when this was the understandable priority. However, the simplicity of the message meant that the intended nuances in the regulations were poorly understood, with the focus on ‘protecting the NHS’ potentially discouraging people from seeking medical treatment for non-Covid-19 conditions or from seeking help when they needed it. The balance between simplicity and detail became increasingly difficult to strike as the regulations and guidance became more complex. The introduction of localised restrictions made it difficult for members of the public to understand what rules applied to them in different places and situations, and their confusion was compounded by variations in rules across the four nations.
In focusing on how to get messages across to the whole population, the needs of vulnerable groups were sometimes lost. In particular, the UK government and Northern Ireland Executive initially failed to provide British Sign Language interpretation for press conferences or to provide key guidance in alternative formats. These are not secondary considerations. Everyone should be able to understand the action their government is asking them to take, and improvements made later in the pandemic serve to highlight the difference that proper and timely consideration of accessibility issues can make.
Legislation and enforcement (Chapter 13)
The legal response to the pandemic laid bare the limits of the UK’s legislative framework and the practical consequences of devolution. Faced with a public health crisis, the UK government relied on older public health legislation and bespoke emergency laws, rather than the Civil Contingencies Act 2004. While this enabled rapid action, it came at the cost of fragmented decision-making, reduced parliamentary scrutiny and caused public confusion.
Ministers relied on secondary legislation to implement many of the most far-reaching restrictions in modern UK history, with little or no parliamentary oversight. Across all four nations, ministers routinely used a procedure allowing laws to come into effect before they had been approved by the legislatures. While this approach was understandable in the earliest days of the pandemic, the approach continued throughout the pandemic, even when there was ample time for parliamentary scrutiny. This weakened democratic safeguards – the use of emergency regulations must be subject to greater scrutiny in future emergencies.
Frequent, complex changes to the law fuelled confusion, misunderstanding and – at times – incorrect enforcement. Police were asked to enforce unclear, shifting regulations, often issued at the last minute with little guidance. Fixed penalty notices were issued inconsistently across the UK. In England and Wales, some individuals faced £10,000 fines; in Scotland, most fines were just £60. Disproportionate impacts on certain groups were evident, especially in England, Scotland and Wales. In some cases, enforcement was practically impossible or legally uncertain – as seen in Northern Ireland during the controversy over the size of crowds at the funeral of Bobby Storey.
Time and again, public messaging failed to reflect the actual laws in place. Ministers made statements suggesting legal obligations where none existed, or vice versa. The public – and even the police – struggled to distinguish between government advice and binding legal restrictions, and there was no single, easily accessible source that clearly laid out the rules applying in each area. The resulting confusion undermined trust and compliance, particularly as legal rules diverged across the UK.
Intergovernmental working (Chapter 14)
A lack of trust between the Prime Minister and First Ministers of the devolved nations coloured the approach to involving the devolved administrations in UK government decision-making throughout the pandemic. Although the devolved administrations were invited to COBR meetings, they perceived that the decisions had already been effectively made beforehand by the UK government. COBR meetings were largely discontinued after May 2020 and intergovernmental discussions were thereafter led by the Chancellor of the Duchy of Lancaster and Minister for the Cabinet Office – Michael Gove MP (later Lord Gove). The devolved administrations had a positive view of Mr Gove and felt that he was genuine in his efforts to understand their perspectives, but ultimately these meetings were limited in what they could practically achieve without Mr Johnson in attendance. Clearer structures for intergovernmental relations during an emergency, led collectively by the Prime Minister, First Ministers and deputy First Ministers, are necessary to facilitate better informed decision-making across the four nations.
Devolution has been a feature of the UK’s constitutional arrangements for over 25 years and the public is used to the devolved administrations taking different decisions from the UK government. An effective, four-nations response to a pandemic should be capable of accommodating differences in response between the nations, and it is incumbent on politicians to work collectively in the public interest in any future emergency.
Key lessons for future emergencies
In Chapter 15, in Volume II, the Inquiry presents the key lessons that should inform the response in a future pandemic. Ten lessons have been identified across five themes and these should be considered in the development of future pandemic preparedness strategies (see the Inquiry’s Module 1 Report, Recommendation 4).
Multiple scenario planning
Firstly, planning both before and during an emergency must anticipate multiple scenarios and consider the short term and long term in parallel. While no plan will ever be 100% comprehensive, the more potential scenarios that are considered in advance, the better placed decision-makers will be to react quickly and decisively.
Better strategy
Secondly, there must be an unambiguous strategy with clear objectives and a framework to guide how decisions are considered and support faster decision-making. The potential impact of those decisions should be understood in advance of them being implemented.
Acting quickly and decisively
Thirdly, when faced with a virus with the potential for exponential growth, interventions must be imposed earlier and ‘harder’ than might be considered ideal. Even where the available evidence is sub-optimal, decisions still need to be made – putting off decisions until later is in itself a decision not to intervene.
Constructive working
Fourthly, leaders must work constructively within their own governments and across the four nations. Political differences should not be a consideration at a time of national emergency. Leaders should accept responsibility for their decisions and explain clearly to the public if and when they change their mind.
The importance of data
Finally, as part of pandemic preparedness, governments must understand what data they are likely to need during a pandemic and identify how these will be collected. The limitations of data should be understood and clearly explained to decision-makers, and consideration should be given to how front-line experiences can sit alongside quantitative data.
Specific recommendations
Across this Report, the Inquiry also makes a series of recommendations aimed at improving the end-to-end decision-making process during emergencies across the four nations of the UK. Although each recommendation is important in its own right, all the recommendations must be implemented in concert – both with each other and with the recommendations from the Inquiry’s Module 1 Report – to produce the changes that the Inquiry judges to be necessary. In summary, the Inquiry recommends:
- Broadening participation in SAGE: Open recruitment of potential experts and representation of the devolved administrations would ensure that advice to decision-makers draws on a wide range of expertise. The Inquiry also recommends extending the principles of transparency of scientific advice to other forms of technical advice provided to governments, so that the public can understand the range of factors beyond scientific advice that influence decision-making during an emergency.
- Improving the routine consideration of the impact that decisions might have on those most at risk in an emergency: This includes extending to England and Northern Ireland the implementation of the socio-economic duty within the Equality Act 2010 and the use of child rights impact assessments. These changes should aim to identify, during the planning phase, any risks to which vulnerable groups are likely to be exposed during a future pandemic and to ensure that those assumptions are revisited at the outset of an emergency, that the assumptions remain valid and that adequate mitigations are in place.
- Reforming and clarifying the structures for decision-making during emergencies within each nation: Clear arrangements for synthesising advice from across governments and presenting it to decision-makers should be in place from the outset of any future pandemic. Specific recommendations are made in relation to the arrangements in Northern Ireland to avoid a potential vacuum of decision-making powers, should an emergency occur during a period where power-sharing arrangements are suspended.
- Ensuring that decisions and their implications are clearly communicated to the public: The laws and guidance in place should be easily understood, including by having clear plans for making key messages available in accessible formats such as British Sign Language.
- Enabling greater parliamentary scrutiny of the use of emergency powers through safeguards such as ‘sunset clauses’ and regular reporting on the use of powers: The role of the Civil Contingencies Act 2004 should also be re-examined to identify if, when and how it could be used in future emergencies – particularly during the initial phase. Communication of the regulations to the public should also be improved through the creation of a central repository of regulations and guidance.
- Establishing structures to improve the communication between the four nations during an emergency: These structures should aim to minimise the risk of confusion caused by similar, but different, rules being implemented in each nation, seeking alignment of approaches where desirable and providing a clear rationale for differences in approach where they are necessary.
A full list of the Inquiry’s recommendations for Modules 2, 2A, 2B and 2C is included in Appendix 3, in Volume II, to this Report.
Chapter 1: The context for pandemic decision-making – key structures and concepts
Introduction
| 1.1. | This chapter provides the context for the decisions that were taken during the coronavirus (Covid-19) pandemic – namely, the complex devolutional structures and the key scientific concepts. |
Key structures
Devolution in the UK
| 1.2. | The UK has a complex structure of government. The Prime Minister is the leader of the UK government and is ultimately responsible for all policy it implements and decisions it takes. The Prime Minister is supported by the UK Cabinet, which is made up of the senior members of government. Government departments and their agencies are responsible for putting government policy into practice. While some departments (such as the Foreign, Commonwealth and Development Office and the Ministry of Defence) cover the whole of the UK, others do not. This is because some aspects of government are devolved to the Scottish Government, the Welsh Government and the Northern Ireland Executive (also referred to in this Report as the Executive Committee). The UK Parliament typically does not legislate on devolved matters without the consent of the relevant devolved legislatures: the Scottish Parliament, the Welsh Parliament and the Northern Ireland Assembly.1 |
| 1.3. | The devolved administrations are responsible for many domestic policy issues and their legislatures have law-making powers for those areas. For example, the Scottish Government, the Welsh Government and the Northern Ireland Executive are responsible for education, culture, the environment and transport in their respective nations. Critically for this Inquiry, they are also responsible for policy and laws in relation to health.2 |
| 1.4. | In the UK, powers that are not specifically reserved to the UK Parliament and UK government are devolved as follows:
Professor Ailsa Henderson, expert witness on devolution and the UK’s response to Covid-19, told the Inquiry that the differing degrees of autonomy among the devolved legislatures stemmed from their distinct origins, varying public appetite for devolution and the ad hoc, reactive changes to the devolution settlements over time.3 |
| 1.5. | The arrangements for the governance of Northern Ireland are distinct because they bring together politicians of different parties who are in opposition to each other (in terms of their designation as nationalist or unionist), along with politicians who are not aligned in this way. Together, they form an Executive Committee. This is a form of coalition government – but it is a multi-party, ‘coerced’ coalition.4 Because of the way power is shared among the political parties, there is no unified government of the day. Each Executive Department operates with significant autonomy, and individual ministers have authority to determine policy and operations within their departments without needing to maintain a collective Cabinet position. These power-sharing arrangements are not merely a framework for devolved governance but are fundamental to sustaining peace in Northern Ireland. They hold the highest constitutional significance, stemming from the Belfast Agreement of 1998 (also known as the Good Friday Agreement) and endorsed through referendums. This Inquiry does not seek to question or critique these arrangements, their structure or their rationale. |
Local services
| 1.6. | Local services are the responsibility of local councils and local authorities, as well as a number of directly elected regional mayors in England who chair combined authorities (ie groups of local councils) with specified functions and budgets. As set out in the Inquiry’s Module 1 Report, this includes regional and local activities related to civil emergencies such as pandemics.5 |
Understanding the implications for a public health emergency
| 1.7. | In a public health emergency, relevant powers span both reserved and devolved areas. For example, emergency powers, air transport and immigration are reserved to the UK government, while policing and justice are reserved in Wales but devolved in Northern Ireland and Scotland.6Key public services in Scotland, Wales and Northern Ireland affected by the pandemic – in particular, public health services and education – are the responsibility of the devolved administrations. |
| 1.8. | However, some devolved policy areas relevant to public health emergencies (such as health) may overlap with reserved policy areas (such as UK border control). Professor Daniel Wincott (expert witness on Welsh Government core political and administrative decision-making) referred to this overlap as the “jagged edges of devolution”,7 while Professor Paul Cairney (expert witness on Scottish Government core decision-making and political governance) noted that the boundaries between reserved and devolved responsibilities are “blurry” and “overlaps are inevitable when problems transcend individual policy sectors”.8 |
| 1.9. | In addition to this overlap, the legal powers to deal with the spread of infection are set out in different pieces of legislation for the four nations of the UK. The decision to use pre-existing public health legislation and the bespoke Coronavirus Act 2020, which was passed with the consent of the devolved legislatures – rather than the UK-wide Civil Contingencies Act 2004 – meant the response to Covid-19 followed devolved responsibilities rather than being managed more centrally.9As considered in more detail in Chapter 13: Legislation and enforcement, in Volume II, this had advantages and disadvantages. However, the pandemic necessitated shared responsibility between the UK government and the devolved administrations. |
| 1.10. | The UK government relied on a range of decision-making structures and bodies to address the crisis, including:
|
| 1.11. | In parallel, each devolved administration established its own mechanisms to manage health and emergency responses, reflecting the devolved nature of public health responsibilities. This was done as follows:
|
| 1.12. | Each of the devolved administrations has a Chief Medical Officer. The Scottish and Welsh governments also each have a Chief Scientific Adviser. During the Covid-19 pandemic, the Northern Ireland Executive did not have a cross-government adviser but had two departmental Chief Scientific Advisers. They worked with Professor (later Sir) Christopher Whitty (Chief Medical Officer for England from October 2019) and Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, to provide coordinated advice to government departments in all four nations. |
| 1.13. | There are a number of expert scientific advisory groups at UK level to advise the Chief Medical Officers for the four nations, health authorities and the devolved administrations directly. During the Covid-19 pandemic, these included the following:
|
| 1.14. | Although effective coordination between the UK government and devolved administrations was essential, established mechanisms for intergovernmental relations, such as the Joint Ministerial Committee – a set of committees that comprises ministers from the UK government and devolved administrations – were not used. Instead, at the outset of the Covid-19 pandemic, intergovernmental coordination was intended to function through COBR meetings and regular ministerial discussions. Ad hoc mechanisms were also introduced, including regular meetings chaired by Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021 and Minister for the Cabinet Office from February 2020 to September 2021, with the First Ministers of Scotland and Wales, as well as both the First Minister and deputy First Minister of Northern Ireland. |
| 1.15. | The pandemic therefore revealed both the strengths and challenges of the UK’s devolved system. While devolution enabled tailored responses to local circumstances, it also exposed the limitations of ad hoc coordination and the lack of institutionalised mechanisms for intergovernmental cooperation during a national crisis. Divergent approaches, overlapping responsibilities and inconsistencies in communication highlighted the need for clearer frameworks to balance flexibility with unity. Future public health emergencies will require strengthened intergovernmental structures to ensure both effective collaboration and the ability to address regional needs. |
Key scientific concepts
| 1.16. | Initial information about new viruses is always limited. Covid-19 was initially identified as pneumonia, but within a few days the World Health Organization announced that the cause of an outbreak in Wuhan in the Hubei province of China had been identified as a novel or new coronavirus.10 As summarised in the Inquiry’s Module 1 Report, coronaviruses are a large family of respiratory viruses.11 They cause a diverse range of illnesses, from the common cold to life-threatening conditions such as severe acute respiratory syndrome (SARS) and the highly deadly Middle East respiratory syndrome (MERS). Some coronaviruses transmit easily from person to person, while others do not.12 |
| 1.17. | In order to assess the threat posed by any new and rapidly growing epidemic, it is vital to understand as quickly as possible some key aspects of how the virus is transmitted between people and how severe the illness it causes can be.13 |
Understanding transmissibility
| 1.18. | In order to assess the risk posed by an emerging virus, it is essential to know how contagious it is (ie whether and how easily it is transmitted between people). |
| 1.19. | Evidence of person-to-person transmission is “the critical tell-tale sign of a potential pandemic.14 Some viruses are only capable of transmitting between a small number of people who are in close contact with each other – such as in a family, care or work setting – before dying out. This is referred to as ‘limited’ person-to-person transmission. Other viruses may be able to continue spreading with ease from one person to the next within the wider community. This is known as ‘established’ or ‘self-sustaining’ person-to-person transmission. At SAGE’s first meeting to discuss the outbreak on 22 January 2020, it was not known whether sustained transmission was occurring.15 |
The speed of transmission
| 1.20. | Transmissibility is affected by:
|
| 1.21. | The transmissibility of a virus is measured by the reproduction number (ie the average number of people that one person with a particular disease infects). The reproduction number is also known variously as the ‘R number’, the ‘R value’, ‘R0’ (R zero), ‘Rt’ or just ‘R’. |
| 1.22. | References to the reproduction number in the evidence considered by the Inquiry – and references to it in this Report – are generally references to Rt. This is the average number of people that a single infected person passes the virus on to at a particular time point, taking into account current levels of immunity and the extent of social mixing.18 Whenever Rt is above 1, an epidemic is still growing. Whenever it is below 1, the epidemic is shrinking.19 It is Rt that interventions such as social distancing were intended to reduce. |
| 1.23. | Less commonly, there are references to ‘R0’, which represents the average number of people that one infected person would pass the virus to in a population with normal mixing behaviour and no prior immunity.20 R0 can be used to estimate the proportion of a population that will eventually become infected. On 28 January 2020, R0 for Covid-19 was estimated by SAGE to be between 2 and 3 during the first outbreak in Wuhan.21 If replicated in the UK, this would have translated to about 80% of the population becoming infected.22 |
| 1.24. | Rt and R0 can be used together to inform estimates of the ‘doubling time’ (ie how long it will take for the total number of cases to double). A doubling time of one week means that the number of cases will be twice the current size after one week, four times that size after two weeks and eight times that size after three weeks. Estimates of the doubling time of Covid-19 in the UK remained highly uncertain, given the lack of testing and concerns about the extent to which cases were not being identified. |
| 1.25. | The transmissibility of a virus is also informed by identifying when people become infectious and the period for which they remain infectious:
Taken together, the incubation period and duration of infectivity are important for informing the design of the response – particularly the length of self-isolation for infected individuals and their contacts.27 The upper estimates of an incubation period for Covid-19 of about 11 days, and a duration of infectivity of 14 days, informed the initial recommendation of a 14-day isolation period for contacts of people testing positive.28 |
| 1.26. | Increased testing of suspected cases is vital to understanding the true extent of transmissibility, and this was echoed in a message from the World Health Organization on 16 March 2020 imploring all countries to “test, test, test”.29 The data used to estimate growth also need to cover a sufficiently long period – ideally at least two weeks – to account for factors such as the typical delay in obtaining test results at weekends.30 |
Routes of transmission
| 1.27. | Alongside understanding how quickly a disease is spreading, it is important to understand how the disease spreads from person to person. The five main routes of transmission capable of sustaining a pandemic or major epidemic are: respiratory (eg influenza); sexual and blood-borne (eg human immunodeficiency virus); oral – from water or food (eg cholera); vector transmission from insects or arachnids (eg malaria); and touch (eg Ebola virus disease).31 Respiratory viruses can also transmit via objects or surfaces (known as fomites) that are contaminated by droplets or aerosols exhaled by someone infected, then transferred to people whose hands touch the contaminated surface and then their eyes, nose or mouth.32 |
| 1.28. | Covid-19 was understood from an early stage to transmit predominantly via respiratory routes.33 However, there was considerable uncertainty about the extent of transmission at closer range (typically one to two metres) via larger respiratory droplets and through very small airborne aerosols that can remain in the air for long periods of time and infect at greater distances. In the early stages of the pandemic, scientists thought most transmission was likely to be via droplets, with some fomite transmission and less aerosol spread.34 Initial advice from the World Health Organization in December 2019 suggested that the virus spread “mainly” through droplets or shorter-range aerosols, but by July 2020 there was a growing body of evidence supporting the importance of airborne transmission.35 Over the course of the pandemic, there was only a small amount of epidemiological evidence showing that a significant amount of Covid-19 was transmitted by fomites, and advice given by scientists shifted from a strong focus on cleaning surfaces and washing hands to a greater emphasis on ventilation.36 |
| 1.29. | It is also important to understand the extent to which an individual who does not display symptoms (someone with an ‘asymptomatic infection’) can infect others. This is known as ‘asymptomatic transmission’.37 In the absence of mass diagnostic testing, it is not possible to calculate the spread of a virus if symptoms are not detectable. If infected people do not show symptoms, it means that they will not know to self-isolate before they infect others. As explained by Professor Sir Michael McBride (Chief Medical Officer for Northern Ireland from September 2006):
“[T]here is a very different response required for planning for and responding to a pandemic which has asymptomatic transmission.”38 |
| 1.30. | With a reliable test, it is possible to measure the proportion of asymptomatic infections by testing a sample of the population. In February 2020, modellers from Imperial College London used data from repatriation flights from China to estimate that one-third of infections of Covid-19 were asymptomatic.39 |
| 1.31. | However, measuring the proportion of onward asymptomatic transmission is more complex, as people without symptoms will not generally be tested and the chain of transmission is unlikely to be identified unless they are tested by chance.40 At its meeting on 28 January 2020, SAGE noted that there was “limited evidence of asymptomatic transmission” but that early indications implied “some is occurring”.41 A Public Health England study carried out in six care homes across London during April 2020 identified that almost 40% of residents had tested positive for Covid-19, of whom nearly 45% were asymptomatic.42 It concluded that “symptom-based screening alone is not sufficient for outbreak control”.43 Mr Hancock told the Inquiry that this study formed the basis for adopting an assumption that asymptomatic transmission was occurring.44 |
| 1.32. | Understanding the extent of asymptomatic transmission is critical to the design of the response to a virus.45 The significant proportion of asymptomatic transmission during the Covid-19 pandemic, for example, increased the importance of contact tracing to monitor the spread of the virus and meant that personal protective equipment (PPE) needed to be used in a much wider range of settings. |
Understanding severity
| 1.33. | It is also critical to understand the severity of a new disease in the early stages of any pandemic to understand how many people might die as a result of infection.46 Estimates of fatality ratios are “fundamental to determining policy strategy”.47 Severity can be measured by the case fatality ratio and the infection fatality ratio. |
| 1.34. | The case fatality ratio is the proportion of those with a recognised case of infection who die from it. At its simplest, the case fatality ratio can be calculated as the total number of recognised deaths divided by the total number of recognised cases. However, this does not take into account unrecognised cases – particularly those where individuals have mild or no symptoms. If the recognition of cases improves (eg through more testing) then the case fatality ratio will often be corrected downwards, which would also reduce the overall expected death toll of the pandemic. At a meeting on 11 February 2020, SAGE reported an uncertain case fatality ratio of 2% to 3%.48 |
| 1.35. | The infection fatality ratio is the true proportion of all infected individuals, including those without symptoms, who die because of the infection. Estimates of the infection fatality ratio attempt to correct for biases in testing and errors in attribution of the cause of death. The true underlying number can decrease significantly over time due to natural immunity, vaccines and therapeutics, but can increase significantly if pressure on healthcare systems means infected people are not receiving timely or effective treatment. In a February 2020 report, Imperial College London estimated an infection fatality ratio for Covid-19 of approximately 1%.49 As Professor Neil Ferguson (Mathematical Epidemiologist at Imperial College London) explained:
“80% of the population being infected translates into approximately 500 thousand deaths in the UK.”50 However, the infection fatality ratio for Covid-19 varied significantly by age. On 4 March 2020, SAGE endorsed assumptions of a rate for people aged 19 and under of 0.01%, and for those aged 80 and over of 8.76%.51 |
Understanding potential responses to a pandemic
| 1.36. | In the early stages of the pandemic, one of the main priorities was to establish the likely impact of Covid-19 if it arrived in the UK in order to design a response. |
| 1.37. | In advance of sufficient data, a reasonable worst-case scenario was used as a tool for planning purposes to illustrate the worst manifestations of the risk that could reasonably be expected.52 It was not a prediction of what would happen, but the worst that could reasonably happen if no countermeasures were put in place. |
| 1.38. | It was agreed in January 2020 that the reasonable worst-case scenario for pandemic influenza should be used for government planning for Covid-19 until sufficient data emerged.53 As a result, plans proceeded on the basis of:
“the reasonable worst-case scenario … similar to a medium flu pandemic (with the added challenge of no vaccine)”54 Although it was not a prediction of what would happen, it was calculated that as many as 820,000 people in the UK might die.55This would, of course, shape the response. |
Strategies
| 1.39. | There are three key strategies that can be adopted in response to a pandemic (see Table 1), although the distinctions between these approaches continued to evolve during the course of the Covid-19 pandemic. |
| 1.40. | Under a ‘mitigation’ strategy, the spread of the virus is seen as inevitable. Any interventions in response are aimed at reducing or slowing the spread of the virus to reduce its peak – rather than reversing its growth – and are therefore relatively minor, such as advising people to minimise contact with others. Rt would be reduced but would remain above 1 and the epidemic would continue to grow. The pandemic would peak at a lower level over a longer period, rather than there being a higher peak of infections over a comparatively shorter period.56 A mitigation strategy reduces the number of people infected with the virus at any one time and therefore also reduces pressure on the healthcare system, while providing some time to research effective treatments or develop vaccines. However, although peak cases would be lower, a similar number of people overall would still eventually be infected. There might be efforts to protect groups likely to be more clinically vulnerable to the virus, rather than applying to the population as a whole – for example, the provision of PPE in hospitals or restrictions on visitors to care homes. The UK Influenza Pandemic Preparedness Strategy 2011 is an example of a mitigation strategy, which had the following as its premise:
“It will not be possible to stop the spread of, or to eradicate, the pandemic influenza virus, either in the country of origin or in the UK, as it will spread too rapidly and too widely.”57 |
| 1.41. | A ‘suppression’ strategy aims to deploy more stringent or widespread interventions that bring Rt below 1 to reverse the growth of the epidemic. Strict interventions such as physical distancing and legally backed ‘stay at home’ orders can be used to substantially reduce the transmission of cases and bring Rt below 1. The benefit of a suppression strategy is that, since the number of infections in circulation should decline, fewer people will be infected with the virus while the measures are in place. However, a suppression strategy does not bring the epidemic to an end; it will return to growth once interventions are released. As a result, interventions might need to be reintroduced periodically, unless an effective system is in place to test, trace and isolate any new infections or until medical countermeasures become available that can halt transmission of the virus or significantly reduce its severity. |
| 1.42. | An ‘elimination’ strategy aims to deploy strict interventions until there is no transmission of cases in the community. Under this approach, strict interventions are introduced and not released until the virus has stopped circulating in the community. Although an elimination strategy aims to reduce cases to effectively zero, the risk of new cases of the virus being reintroduced – particularly through international travel – means that at least some action may be required until such time as effective medical countermeasures are available. Countries that pursued an elimination strategy – often referred to as a ‘zero Covid’ strategy – during the pandemic were generally geographically isolated islands, such as New Zealand, that were able to apply strict restrictions at international borders to reduce the risk of importing new cases. |
| Strategy | Aims | Potential public health interventions |
|---|---|---|
| Mitigation | • Slow the rate of virus transmission, but with Rt remaining above 1 • Protect clinically vulnerable people from infection |
• Advisory interventions to minimise contacts • Measures focused on the protection of clinically vulnerable people, such as restrictions in care homes |
| Suppression | • Reduce the rate of virus transmission until Rt is below 1 • Prevent healthcare systems from being overwhelmed |
• Measures to reverse growth of cases, potentially including lockdowns • Testing, contact tracing and self-isolation • Shielding for vulnerable groups |
| Elimination | • Eliminate community transmission • Identify and stop chains of transmission |
• Stringent measures, including maintaining lockdowns until community transmission is halted • Tight border restrictions and quarantine of arrivals • Testing at scale, with strict isolation of cases and contacts |
Interventions (also known as non-pharmaceutical interventions)
| 1.43. | Interventions or measures adopted in response to a pandemic (excluding vaccines, drugs or other medical interventions) may seek to:
|
| 1.44. | It can be difficult to measure the effectiveness of individual interventions. Many common research methods such as randomised controlled trials (eg shielding only part of the clinically vulnerable population) would not be feasible or ethical to conduct during an emergency. The way an intervention is implemented (eg how it is communicated) can also impact its effectiveness. Behavioural responses can also obscure the effect of an intervention, such as people choosing to avoid settings that they perceive to be high risk even when they are not subject to restrictions.59 |
| 1.45. | It is also critical to note that interventions can have significant downsides, such as the economic harm caused by forcing businesses to remain closed, the social harm caused by closing schools, or the health harm caused by missed screening and treatment of other health conditions.60 Decision-makers therefore need to balance the potential for an intervention to reduce the direct harm of the virus against the potential for it to increase harms elsewhere. |
Anticipating and reacting to variants
| 1.46. | Variants of a virus will appear regularly, but not all will change the behaviour of the virus or become significant problems.61 Early detection and notification of variants is of the utmost importance in any pandemic response. As a new variant is identified, key factors such as its transmissibility, the severity of illness it causes and its potential for ‘escaping’ the immunity conferred by prior infection or vaccines have to be reassessed. |
| 1.47. | During the Covid-19 pandemic, three ‘variants of concern’ became dominant at different stages – Alpha, Delta and Omicron. Each of these was more transmissible than previous strains. Omicron in particular exhibited significantly different characteristics from the original strain of the virus. For example, its generation time of between 1.5 and 3.2 days was far shorter than the 6 to 7 days of previous variants,which made Omicron more difficult to contain with test, trace and isolate procedures.62 |
Immunity
| 1.48. | Understanding the nature of immunity following infection or indeed vaccination is critical to understanding how an epidemic might come to an end. |
| 1.49. | Where a population achieves protection from an infectious disease, either through immunity developed from having previously been infected or through vaccination, this is known as ‘population immunity’ (or ‘herd immunity’). It results in fewer people to infect and the spread of the virus gradually slows to a halt. Population immunity provides protection for the whole of a population, including people who have not themselves caught the disease or received a vaccine. The percentage of the population that needs to be infected or vaccinated to achieve population immunity depends on the transmissibility of the disease, with a higher rate of transmission requiring a higher threshold for population immunity.63 For example, the basic reproduction number for measles is estimated to be between 10 and 20 (ie a single child with measles will infect between 10 and 20 others), and therefore the World Health Organization has a target of 95% vaccine coverage to achieve and maintain measles elimination.64 |
| 1.50. | However, population immunity is not an inevitable endpoint for an epidemic. Many diseases never reach this threshold, or only do so temporarily. Immunity might weaken over time to the point that it no longer prevents people from being reinfected, or variants of the virus may emerge that escape prior immunity.65 Understanding the level of protection offered by vaccination or previous infection is therefore critical to understanding whether population immunity can be achieved.66 Vaccination or prior infection may also reduce the severity of any subsequent infection.67 That knowledge will be inherently uncertain in the early stages of an epidemic, when case numbers are small – and especially uncertain for a novel virus. |
Complications or resulting conditions
| 1.51. | Viral infections can cause long-term illnesses – known as ‘long-term sequelae’ – after the initial acute infection. While these may appear rare for most viruses, large numbers of cases can occur at the same time when the virus is at the scale of a pandemic.68Not all viruses will cause significant long-term illnesses, and this was not a “major common problem” for viruses such as severe acute respiratory syndrome coronavirus 1 (SARS-CoV-1), which causes SARS and is closely related to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, which causes Covid-19) and Middle East respiratory syndrome coronavirus (MERS-CoV), which causes MERS.69 As Professor Whitty told the Inquiry:
“Some very severe diseases rarely have post infection syndromes whilst other relatively trivial infections can have quite common and prolonged ones.”70 |
| 1.52. | While the potential for long-term illnesses to occur is predictable, the scale and characteristics of those illnesses vary from virus to virus and cannot be predicted.71 The long-term illnesses arising from Covid-19 are commonly described as Long Covid. Over 200 symptoms of Long Covid have been reported, though it often involves fatigue, breathlessness and ‘brain fog’, impacting on both mental and physical function and leading to disability and impaired health.72 Much remains unknown about the mechanisms causing Long Covid.73 The percentage of those who go on to develop it following infection with Covid-19 also remains unknown – the World Health Organization has estimated that between 10% and 20% of infected people will develop Long Covid.74 |
- The Sewel Convention is a constitutional principle stating that the UK Parliament will not normally legislate on matters within devolved competence without the consent of the relevant devolved legislature.
- INQ000083096
- INQ000269372_0010 para 26
- INQ000472398_0006
- Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 2(https://covid19.public-inquiry.uk/documents/module-1-full-report)
- For full lists of reserved matters, see Schedule 5 of the Scotland Act 1998 (https://www.legislation.gov.uk/ukpga/1998/46/contents); Schedules 2 and 3 of the Northern Ireland Act 1998 (https://www.legislation.gov.uk/ukpga/1998/47/contents); and Schedule 7A of the Government of Wales Act 2006 (https://www.legislation.gov.uk/ukpga/2006/32/contents).
- INQ000411927_0020 para 44
- INQ000274154_0005 para 1
- Coronavirus Act 2020 (https://www.legislation.gov.uk/ukpga/2020/7/contents); Civil Contingencies Act 2004 (https://www.legislation.gov.uk/ukpga/2004/36/contents)
- INQ000236523_0001
- Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 1 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000236523_0001
- This was recognised in the UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000232194_0024 para 95
- INQ000061509_0003 para 7
- INQ000270553_0008 para 4.3
- INQ000270553_0009 para 4.6
- INQ000252450_0013 para 2.15
- INQ000251645_0057 para 5.41
- INQ000252450_0013 para 2.14
- INQ000061510_0003 para 11
- INQ000119430_0001 para 5
- INQ000174700_0002 para 8; INQ000074987_0001
- INQ000251645_0055 para 5.31
- INQ000251645_0055 para 5.33
- INQ000074896_0001; INQ000051925_0002 para 17
- INQ000251645_0056 para 5.39
- INQ000251645_0055 para 5.32
- INQ000512530
- INQ000249526_0083-0084 para 258
- INQ000248853_0088 para 6.2
- INQ000236261_0056 para 10.27
- INQ000248853_0099 para 6.51
- INQ000238826_0112 para 339
- INQ000236522_0004; see also INQ000203978_0001; INQ000236261_0049-0050 para 10.9
- INQ000236261_0057 paras 10.33-10.34
- There is also ‘presymptomatic transmission’, where the infection is passed on by someone who was not displaying symptoms at the time but who goes on to develop symptoms of illness later.
- Michael McBride 10 May 2024 68/19-21
- Neil Ferguson 17 October 2023 134/7-20; see also the SAGE meeting on 10 September 2020, which noted that a review of 22 studies put the figure at 28%, albeit with very wide confidence intervals (INQ000061564_0005 para 31)
- INQ000251645_0053-0054 para 5.25
- INQ000061510_0003 para 16
- INQ000089681_0003
- INQ000089681_0004
- INQ000232194_0083 para 346
- INQ000252450_0015 para 2.25
- The case fatality ratio and infection fatality ratio only measure the direct severity of the virus itself and do not account for deaths indirectly related to the spread of the virus, such as those that might arise from healthcare systems being unable to treat other health conditions.
- INQ000249526_0040 para 126; INQ000310090_0003 para 19
- INQ000061514_0003 para 9
- Report 4: Severity of 2019-Novel Coronavirus (nCoV), Imperial College London, 10 February 2020, p1 (https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-severity-10-02-2020.pdf; INQ000236277)
- INQ000249526_0040 para 126
- INQ000074987_0002
- See also Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 3 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000061510_0004 para 27
- INQ000233747_0002
- INQ000232194_0038 para 159; INQ000320718_0002
- INQ000249526_0048 para 150(b)
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, p15 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, pp234-235
(https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642) - Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, pp239-240 (https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642)
- Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, p235
(https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642) - INQ000251645_0155-0156 para 8.93
- INQ000213239_0003-0004 para 9
- INQ000248853_0091 para 6.15
- See Risk Assessment for Measles Resurgence in the UK, UK Health Security Agency, July 2023 (www.gov.uk/government/publications/measles-risk-assessment-for-resurgence-in-the-uk; INQ000548395)
- INQ000252450_0017 para 2.35
- INQ000252450_0017 para 2.36
- INQ000252450_0017 para 2.34
- INQ000251645_0207; INQ000273807_0169 para 12.1
- Peter Horby 18 October 2023 222/20-223/2
- INQ000251645_0207 para 12.2
- INQ000273807_0169 para 12.1
- INQ000280198_0011-0012 para 1.14-1.16
- INQ000280198_0016 para 3.4
- INQ000280198_0019 para 4.1-4.2; see also INQ000271436_0075, 0077-0079 paras 231-232, 238-247
Chapter 2: The emergence of Covid-19 (January and February 2020)
Introduction
| 2.1. | As Covid-19 emerged in early 2020, the UK government and the devolved administrations were facing a number of pressing matters. These included: the setting up of a new administration under Boris Johnson MP (Prime Minister from July 2019 to September 2022) following the December 2019 General Election; the resumption of power-sharing in Northern Ireland on 11 January 2020 after a prolonged period of suspension; the departure of the UK from the European Union (EU) on 31 January 2020; widespread flooding in Wales in February 2020; and preparations for the UK government budget in March 2020. |
| 2.2. | This chapter examines how, against this backdrop, the systems and personnel within the UK government and devolved administrations responded to the developing crisis in the first two months of 2020. The decisions that were made during this early and fast-moving phase of the Covid-19 pandemic had a significant impact on the effectiveness of the UK’s response. The chapter considers whether the scientific, administrative and political arms of government properly understood the threat and reacted appropriately and with sufficient speed on learning of the emergence of the virus. |
January 2020: Emerging understanding
| 2.3. | When Covid-19 first emerged, there was a great deal that was unknown, including some of the key characteristics of the virus, as set out in Chapter 1: The context for pandemic decision-making, in this volume. In particular, the nature and extent of its transmission were not understood, including the degree to which it could be transmitted through contact or respiratory routes.1 |
Initial awareness
| 2.4. | On 2 January 2020, Professor (later Sir) Jonathan Van-Tam, Deputy Chief Medical Officer for England from October 2017 to March 2022, received an email notification from a publicly available system reporting infectious disease outbreaks. It referred to a “mystery viral pneumonia outbreak” in the city of Wuhan, China, which had led to the hospitalisation of 27 people – the majority of whom were stallholders at a live animal ‘wet market’.2 Professor Van-Tam forwarded the email to colleagues in the Department of Health and Social Care, including Professor (later Sir) Christopher Whitty, Chief Medical Officer for England from October 2019. He commented that the outbreak was “one we should watch (no more than that)”.3 Over the next few days, he sought to obtain further information from multiple sources, including Professor (later Sir) Peter Horby (Professor of Emerging Infectious Diseases and Global Health at the University of Oxford), the World Health Organization and the US Centers for Disease Control and Prevention.4 On 3 January 2020, Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, activated the internal Scientific Advisory Group for Emergencies (SAGE) team to monitor the outbreak.5 |
| 2.5. | On 5 January 2020, Professor Whitty identified three “triggers” which, if met, would “mean we should start taking a close interest and considering risk to the UK”.6 These triggers were:
Professor Whitty said that “much of the next 2 weeks were spent trying to ascertain if the triggers were met”.8 |
| 2.6. | Professors Whitty and Vallance met on 7 January 2020 and discussed the outbreak in Wuhan. At this stage, their view aligned with that of Professor Van-Tam and:
“would have been that this was something to keep a close eye on rather than something which was definitely going to turn into a pandemic”9 |
| 2.7. | On 8 January 2020, Professor Van-Tam advised the Department of Health and Social Care that there remained “no known [person-to-person] transmission” in relation to the new emerging virus.10 |
| 2.8. | Public health agencies across the UK shared information. On 7 January 2020, Public Health England provided a briefing note on the known cases in Wuhan, along with clinical advice and advice on implications and recommendations for onward distribution to the NHS, private health providers and the devolved administrations.11 Each devolved administration subsequently produced its own briefing.12 Public Health England also began work on adapting its First Few Hundred Protocol, which functioned as both a scientific study (to gather and publish data on all early UK cases of a new outbreak) and a relatively small-scale test and contact tracing system for initial cases.13 |
| 2.9. | On 9 January 2020, Public Health England assessed that the current threat level to the UK population was “Very Low”.14 However, the purpose of this and other risk assessments was:
“not to assess the risk at some theoretical future point but rather the risk at that point in time [ie on that day]”.15 Professor Whitty told the Inquiry that, with China having “reported 41 cases and the first case outside of China had just been reported”, in the circumstances as they then stood, the ‘very low’ threat was “a rational assessment”.16 |
| 2.10. | Professor Van-Tam also emailed Professor Whitty, noting that there had been no reported deaths to date but that the reported severity of the disease and hospitalisation rates were such that, in his view:
“established person-to-person transmission would cause serious hospital surge pressures on a par with a severe panflu virus”.17 |
| 2.11. | Also on 9 January 2020, Matt Hancock MP, Secretary of State for Health and Social Care from July 2018 to June 2021, received his first written briefing by email from the Department of Health and Social Care, which stated:
“[T]he assessed risk to people in Wuhan is low to moderate, and the risk to the UK is low. There is no evidence of human to human transmission.”.18 Mr Hancock informed Mr Johnson of the outbreak.19 Recalling their exchange, Mr Johnson told the Inquiry that he: “could tell he was serious. I said that I understood his concern but could see no reason to panic. I felt that I was familiar with zoonotic diseases and the public health scares they can cause.”.20 Those “scares” included “things like SARS [severe acute respiratory syndrome] and MERS [Middle East respiratory syndrome] and swine flu [the 2009 to 2010 H1N1 influenza pandemic]”, which had had an impact in Asia in particular, but, as Mr Johnson observed, “ultimately were relatively, if not wholly benign in the UK”.21 |
| 2.12. | On the same day, the World Health Organization reported that Chinese authorities had stated that the coronavirus did “not transmit readily between people”.22 It made no recommendations for any specific measures for travellers and advised against the application of any travel or trade restrictions with China. |
| 2.13. | On 13 January 2020, Thailand reported the first case imported from Wuhan.23 The National Incident Management Team of Health Protection Scotland (which facilitated the flow of advice and information to the Scottish Government) also met for the first time.24 |
| 2.14. | Similarly, that day, the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) met formally for the first time to consider the outbreak.25 It noted:
“[I]t has been stated that there has been no ‘significant’ human to human transmission, which implies there may be some evidence of limited human to human transmission which has not yet been made available. Given that the onset dates are over a period of almost one month, and now the case in Thailand, we should be cautious at this point in making conclusions about the absence[of]human to human transmission.26 |
| 2.15. | Professor Van-Tam attended the meeting and reported to the Civil Contingencies Secretariat in the Cabinet Office that NERVTAG was:
“watching closely; remain cautious that it is too early to rule out all person to person [transmission] but it so far looks very low or absent”.27 This was also reflected in a Department of Health and Social Care briefing note provided to Mr Hancock on 14 January 2020, which stated: “Although such transmission cannot yet be ruled out there does not appear to be a significant risk of human to human transmission at this time.”28 (emphasis in original) |
| 2.16. | On 14 January 2020, the World Health Organization announced:
“Preliminary investigations conducted by the Chinese authorities have found no clear evidence of human-to-human transmission.”.29 |
| 2.17. | Professor Van-Tam emailed Professor Whitty on 16 January 2020, after identification of a confirmed case in Japan, stating:
“[T]his does give me increased worry that the footprint of infections in Wuhan is far larger and more dispersed than we are being told and no longer market focused. And to note the interval between symptom onset and hospitalisation (assumed on clinical grounds) is 10 days – quite long. It does also reinforce that there is some form of P2P [person-to-person] transmission even if relatively inefficient. Do you agree?”.31 However, it informed the media that: “[f]rom the information that we have it is possible that there is limited human-to-human transmission, potentially among families, but it is very clear right now that we have no sustained human-to-human transmission.”30 Professor Whitty agreed.32 |
| 2.18. | That day, Professors Whitty, Vallance and Van-Tam received an email attaching a report from Professor Neil Ferguson, Mathematical Epidemiologist at Imperial College London. Professor Ferguson estimated that:
“between 189 and 3500 cases have occurred by 6th January, with a central estimate of 1149. Our analysis does not directly address transmission routes, but past experience with SARS and MERS-CoV [Middle East respiratory syndrome coronavirus] outbreaks of similar scale suggests currently self-sustaining human-to-human transmission should not be ruled out.”33 This was significantly higher than the official figure of 41 confirmed cases in Wuhan. The full report, published the following day, stated: “It is likely that the Wuhan outbreak of a novel coronavirus has caused substantially more cases of moderate or severe respiratory illness than currently reported … past experience with SARS and MERS-CoV outbreaks of similar scale suggests currently self-sustaining human-to-human transmission should not be ruled out.”34 |
| 2.19. | Professor Van-Tam said that, by 16 January 2020, it was:
“fairly clear that human to human transmission was occurring, and my view was that this would be a significant pandemic ”35 He recalled articulating his view to colleagues and ministers shortly after this, and that Professor Whitty agreed that “the situation may well escalate but for now we needed to wait and monitor developments closely”.36 |
| 2.20. | By mid-January 2020, Oxford University scientists had heeded the warnings and adapted a MERS-CoV vaccine research programme into a severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2, the virus that causes Covid-19) research programme.37 A number of other countries and territories had also introduced entry screening at airports of arrivals from China.38 However, in Europe, as noted in a permanent secretary meeting on 20 January 2020, attended by Professors Whitty and Van-Tam, both Italy and France had received direct flights from Wuhan and their governments had “currently not instigated port of entry screening”.39 |
| 2.21. | In a briefing provided on 17 January 2020 to the Scottish Government, NHS boards and others, Health Protection Scotland stated that there had been no confirmed cases outside China, Thailand and Japan but advised that the possibility of person-to-person transmission could not be excluded.40 This was the first briefing sent to Nicola Sturgeon MSP, First Minister of Scotland from November 2014 to March 2023. Although it was “an issue that was increasingly central to our thinking” by the end of January, Ms Sturgeon said that it was only one of a number of issues before her.41 There was also a lack of scientific consensus as to the significance of the virus at that stage. |
| 2.22. | However, there was growing awareness of the possibility of asymptomatic transmission. Sir Jeremy Farrar, Director of the Wellcome Trust from October 2013 to February 2023, alerted Professor Whitty on 19 January 2020 to an unpublished scientific paper that, in his view, suggested “transmission in absence of material symptoms”.42 Professor Whitty considered that it would be “actively unhelpful” to “do anything at a government level”.43 In forwarding this to Professor Van-Tam, Professor Whitty agreed that “it provides reasonable additional evidence of onward transmission, although he was:
“less convinced it shows people who are asymptomatic are infectious (whichwould be a major issue, so important not to jump the gun)”.44 Professor Van-Tam’s view was that the data showed “a possibility of asymptomatic transmission”.45 |
An increasing threats
| 2.23. | On 20 January 2020, in London, the first Wuhan Novel Coronavirus Officials’ meeting took place.46 It was chaired by Sir Christopher Wormald (Permanent Secretary to the Department of Health and Social Care from May 2016 to December 2024) and attended by Professors Whitty and Van-Tam.47 Sir Christopher Wormald stated that his personal involvement in the response “escalated” from this point.48 |
| 2.24. | By this time, both Professors Whitty and Van-Tam were “increasingly concerned”, although Professor Whitty stated that he:
“did not at this stage think it necessarily would become a significant threat to the UK, but thought the potential was increasing. The tempo of our response therefore increased from 20 January 2020 onwards .”49 Mr Hancock said that, by 20 January 2020, Professor Whitty had advised him that there was “a 50/50 chance of the virus going global and becoming a pandemic”.50 |
| 2.25. | On 21 January 2020, Professor Vallance raised the emerging novel virus with Sir Mark Sedwill (later Lord Sedwill), Cabinet Secretary and Head of the Civil Service from October 2018 to September 2020.51 That same day, NERVTAG concluded that it was clear that at least some person-to-person transmission was occurring, but that “the extent of transmissibility between people is not clear”.52 It remained unknown whether sustained transmission in the community was taking place in Wuhan.53 |
| 2.26. | On 21 January 2020, at a meeting of the NHS Wales Executive Board (which brought together the Chief Executives of NHS Wales), Dr (later Sir) Frank Atherton (Chief Medical Officer for Wales from August 2016) stated:
“[C]olleagues need to think about their plans for isolation and ambulances if it does come to the UK … This area would become of increasing importance. .”54 However, Dr Andrew Goodall (Director General of Health and Social Services in the Welsh Government and Chief Executive of NHS Wales from June 2014 to November 2021) confirmed that work was not initiated at this stage, although Dr Atherton’s comments raised “awareness” of the problem that might come.55 |
| 2.27. | Professor Mark Woolhouse (Professor of Infectious Disease Epidemiology at the University of Edinburgh) also emailed Dr Catherine Calderwood (Chief Medical Officer for Scotland from April 2015 to April 2020) on 21 January 2020. Professor Woolhouse set out his concerns that Scotland was not preparing for a pandemic that reflected the World Health Organization’s latest estimates and currently available evidence.56 He noted that there were some instructive parallels with H1N1 influenza, with “a widespread epidemic fuelled by mild cases but with mortality among vulnerable patients”.57 He warned that such an epidemic would be “difficult to track” and that the Scottish Government needed to put in place an “integrated surveillance set up that combines clinical surveillance, genomic surveillance, and serological surveillance [the study of bodily fluids as part of the monitoring and analysis of public health]” (noting that the latter required an appropriate test) in advance of the arrival of the virus.58 He cautioned that, in relation to H1N1 influenza, “we were slow off the mark”, and hoped that “history won’t repeat itself” here.59 Later that same Dr Calderwood replied to Professor Woolhouse. She noted his “fears that this might day, develop into a potential pandemic” and reassured him that “response plans are in place”.60 |
| 2.28. | Professor Whitty requested that SAGE meet, on a precautionary basis, to discuss the Covid-19 outbreak.61 That meeting took place on 22 January 2020. SAGE recorded:
“7. There is evidence of person-to-person transmission. It is unknown whether transmission is sustainable. … 12. There is no evidence yet on whether individuals are infectious prior to showing symptoms. 13. There is no evidence that individuals are more infectious when symptoms are more severe, but that is likely .”62 It also noted that the incubation period “appears to be within 5 to 10 days”.63 By 3 February 2020, the Scientific Pandemic Infections Group on Modelling, Operational sub-group (SPI-M-O) estimated it to be an average of 5 days (with a range of 1 to 11 days), which was “approximately twice as long as for influenza”.64 |
| 2.29. | In its Report 2: Estimating the Potential Total Number of Novel Coronavirus (2019-nCoV) Cases in Wuhan City, China , published on 22 January 2020, Imperial College London estimated that there were 4,000 cases in Wuhan by 18 January 2020. It concluded it was likely that the outbreak had “caused substantially more cases of moderate or severe respiratory illness than have currently been detected and reported”.65 That same day, Public Health England raised the current threat level to the UK population (ie the risk on that day, not future risk) from ‘very low’ to ‘low’ on the basis of “the emerging evidence regarding case numbers, potential sources and human to human transmission”.66 It was recorded that two of Professor Whitty’s triggers had been met:
|
| 2.30. | At this point, the UK had “good centralised diagnostic capacity” and was days away from developing a scalable test for deployment across the UK in weeks, having successfully developed an initial diagnostic test within three days of China publishing the genetic code.68 Although a test was developed, scaling up the ability to test was to prove challenging because of inadequate infrastructure and testing capacity (discussed further below). As noted in the Inquiry’s Module 1 Report, one of the recommendations from Exercise Alice (a February 2016 exercise to assess the challenges of a large-scale outbreak of MERS-CoV in England) was the development of a diagnostic test procedure, including a plan to scale up capacity – but it, like others, was not implemented.69 The UK government and devolved administrations could and should have invested in this infrastructure in advance of the Covid-19 pandemic, but had not done so.70 It is unsurprising therefore that testing remained a problem for a prolonged period, as is being examined in Module 7: Test, trace and isolate. |
| 2.31. | Criteria for testing and advice for healthcare workers on testing were being developed, along with plans for both isolation of the infected and contact tracing. Public Health England announced that health officials at Heathrow Airport would meet people returning on direct flights from Wuhan to ask “if they were feeling OK and handing out advice leaflets”.71 Mr Hancock was “concerned that this was too little but accepted the expert advice ”.72 Both Public Health England and NERVTAG, as well as officials at the Department of Health and Social Care, considered that port-of-entry screening was neither efficient nor effective.73 This reflected the “relatively long” incubation period, which increased the risk of a passenger infected with Covid-19 showing no symptoms.74 It was also noted that screening passengers from Wuhan on arrival in the UK would detect relatively few people and potentially only detect those who became unwell during a flight. Providing information to passengers and screening travellers attending healthcare settings was considered likely to be a better option.75 Mr Hancock did, however, request expansion of the enhanced monitoring from Heathrow Airport to all airports with direct arrivals from China.76 |
| 2.32. | Also on 22 January 2020, a briefing was provided to Robin Swann MLA (Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024) which explained that there was evidence to suggest that some limited person-to-person spread might be occurring.77 Public Health Wales invoked its Emergency Response Plan at enhanced level and queried when the Welsh Government would stand up the Emergency Coordination Centre (Wales), responsible for:
“information gathering and keeping Welsh Ministers and the UK Government informed of the implications of emergencies in Wales .”78 The precautionary SAGE minutes were shared with Dr Rob Orford, Chief Scientific Adviser (Health) for Wales from January 2017, Dr Goodall and Sir Frank Atherton. This was the first time Dr Orford became aware of the virus through official government communications.79 |
| 2.33. | In Northern Ireland, this period coincided with the re-establishment of power-sharing and there was little by way of government activity in relation to Covid-19. On 22 January 2020, it was noted that the Civil Contingencies Policy Branch of The Executive Office, which had responsibility for civil contingencies arrangements:
“was allocated responsibility for taking forward the sector resilience element of Pandemic flu preparations a few years ago … However, no work had commenced on it … This has resulted in Northern Ireland being more than 18 months behind the rest of the United Kingdom in terms of ensuring sector resilience to any Pandemic flu outbreak .”80 A submission dated 23 January 2020, sent to Chris Stewart (Director at The Executive Office of Northern Ireland with responsibilities for civil contingencies), stated that there was “a critical lack of resources” in the Civil Contingencies Policy Branch.81 Silver (Tactical) Command Structures involving the Public Health Agency, Health and Social Care Board and Business Services Organisation, however, were instituted.82 |
| 2.34. | On 23 January 2020, the World Health Organization’s Situation Report confirmed that “there is now more evidence that [Covid-19] spreads from human-to-human and also across generations of cases”.83 A briefing note prepared by Public Health Wales for the Welsh Government confirmed that:
“Due to the enlarging geographic area affected, and evidence of human to human transmission, it is increasingly likely that suspected cases … will be identified in the UK, including Wales.”84 |
| 2.35. | On the same day, Mr Hancock made the first statement to the UK Parliament about Covid-19.85 At this point, public transport (including outbound trains and flights) was suspended in Wuhan.86 However, a coach trip of tourists from Wuhan landed in England and drove unimpeded around the UK and into the Republic of Ireland. In Scotland, one of the party developed respiratory symptoms but tested negative for Covid-19. The tour group crossed over into Northern Ireland on about 25 January.87 No steps were taken to prevent this group from entering Northern Ireland and travelling on to the Republic of Ireland.88 A government official in Northern Ireland noted, at the time, that the “CMO [Chief Medical Officer] is not concerned”.89 Richard Pengelly, Permanent Secretary to the Department of Health (Northern Ireland) from July 2014 to April 2022, recorded that, as the individual tested negative for Covid-19 and other passengers were asymptomatic:
“NO action required. To do so would have been contrary to national and international protocols. We would have had no powers to insist .”90 |
| 2.36. | Two days later, Dominic Cummings, Adviser to the Prime Minister from July 2019 to November 2020, asked Mr Hancock in a WhatsApp message, “To what extent have you investigated preparations for something terrible like Ebola or a flu pandemic?”91 Mr Hancock responded that there were “full plans up to & including pandemic levels regularly prepped and refreshed” (see Figure 1). |
Figure 1: Message from Mr Hancock to Mr Cummings, 25 January 2020

Source: Extract from INQ000129180_0001
| 2.37. | Mr Hancock’s reassurance was likely to be a reference to the UK Influenza Pandemic Preparedness Strategy 2011 because, as set out in the Inquiry’s Module 1 Report, no UK-wide contingency plan for SARS, MERS or any other high consequence infectious disease was disclosed by the UK government.92 The Inquiry is not therefore satisfied that such plans ever existed.93 Based on the UK Influenza Pandemic Preparedness Strategy 2011, the UK remained in the first ‘detection’ phase as there were no recognised cases in the UK. The second ‘assessment’ phase would occur when there were isolated cases and clusters, traceable with no “sustained community transmission” with an aim of containment.94 For both phases, the primary action was enhanced surveillance, undertaken as set out above by Public Health England. Other actions included intelligence gathering, development of new tests, public health guidance and communications. |
| 2.38. | On 24 January 2020, COBR met for the first time to discuss Covid-19.95 This meeting was chaired by Mr Hancock (as the Secretary of State for the lead government department responsible for pandemic preparedness, response and recovery) and was attended by health ministers from the devolved administrations.96 Professor Whitty informed COBR that, in Wuhan, there were:
“around 850 confirmed cases and 25 confirmed deaths, however the true number was likely higher with modelling indicating between 1,000 – 10,000 cases. There was no clear evidence of sustained transmission (infectious spread across communities and not just within households) outside of Wuhan .”97 COBR was also informed that at least 2,500 people had travelled from Wuhan to the UK over the previous fortnight.98 Professor Whitty relayed the SAGE advice that “an infected person was likely to be infectious before the onset of symptoms, and very infectious when seriously ill”.99 His advice was: “that an individual case in the UK is likely at some point. The NHS is already well prepared to identify and treat infectious disease cases such as WN-CoV. In the case of a sustained human to human transmissions, we would explore surge measures in healthcare and public containment steps .”100 |
| 2.39. | The UK’s four Chief Medical Officers also met on 24 January 2020. They agreed:
“[T]he risk to the UK public remains low, but there may well be cases in the UK at some stage .”101 |
| 2.40. | Sir Frank Atherton recalled that it was “from around this time that Covid-19 was discussed as a real potential threat to the UK”.102 Professor Sir Michael McBride (Chief Medical Officer for Northern Ireland from September 2006) reflected that, by this time, he too became:
“fully aware of the potential gravity of the outbreak of Covid-19 in China, although the degree of uncertainty around this still remained very high ”.103 |
| 2.41. | In Scotland, on 24 January 2020, Ms Sturgeon received a briefing from the Scottish Government’s Health Protection Policy Team incorrectly stating: “We now know that people carrying the virus are only infectious to other people when experiencing symptoms.”104 Ms Sturgeon challenged the view that asymptomatic transmission was not possible.105 The following day she received advice from Health Protection Scotland, which explained that “it is likely that person to person transmission, when it does occur, mostly involves transmission of virus from people with symptoms” and that:
“infected people with symptoms (e.g., someone who is coughing) are much more likely to spread virus around than someone who is infected but free of symptoms ”.106 |
| 2.42. | In Wales, Mark Drakeford MS (First Minister of Wales from December 2018 to March 2024) was briefed about the COBR meeting. He recalled that Sir Frank Atherton told him on 24 January 2020 “that there was a significant risk the virus would arrive in Wales”.107 The Welsh Government confirmed that it was:
“closely monitoring the emergence of a novel coronavirus originating in Wuhan, China … We are treating this as an enhanced public health incident and we are working very closely with the other UK Nations .”108 |
| 2.43. | Based on a study of the first 41 patients admitted to hospital in Wuhan, published in The Lancet on 24 January 2020, the percentage of people diagnosed with Covid-19 who died from it (the case fatality ratio) appeared to be close to 3%.109 The article noted that 66% of those patients had been exposed to a wet market, that some healthcare workers had been infected and that several exported cases had been confirmed in other provinces in China and other countries.110 An accompanying commentary piece, co-authored by Professor Horby (who was Chair of NERVTAG), warned there was:
“no room for complacency … the increasing number of cases and widening geographical spread of the disease raise grave concerns about the future trajectory of the outbreak … every effort should be given to understand and control the disease, and the time to act is now ”.111 |
| 2.44. | The following day Imperial College London published its third report, Transmissibility of 2019-nCoV. It stated that self-sustaining person-to-person transmission was “the only plausible explanation of the scale of the outbreak in Wuhan”.112 It also concluded that R0 of the new virus (the basic reproduction number, based on the number of secondary infections generated from one initial case) was above 1 and most likely in the range of 2 to 3 (ie one person could infect two to three people).113 |
| 2.45. | In emails with Professor Ferguson and Sir Jeremy Farrar that day, Professor Woolhouse noted:
“The 2 key numbers reported in the WHO [World Health Organization] statement on Thursday are R0=2 and case fatality rate = 4%. Plus we can estimate or make a reasonable guess at the generation time. If we take those numbers at face value we quickly get a ballpark estimate of almost half the people in the UK (and many other countries) getting this infection over a year or so, at least a doubling of the gross mortality rate (much more during epidemic peak), and a completely overwhelmed health system. I know that, you both know that, anyone in the infectious disease modelling community knows that, PHE [Public Health England] must surely know that, and my undergraduate class could work it out with a pocket calculator ”.114 Professor Ferguson agreed, noting that he and Sir Jeremy Farrar had said “the same to Patrick Vallance and Chris Whitty last night”.115 |
| 2.46. | On 25 January 2020, Professor Woolhouse again contacted Dr Calderwood. He noted that Dr Calderwood’s reply to his earlier email of 21 January 2020 “did not give any indication that here in Scotland we are preparing” for a pandemic at this scale, where over the course of a year:
“at least half the population will become infected, the gross mortality rate will triple (more at the epidemic peak) and the health system will become completely overwhelmed ”.116 Professor Woolhouse said it was now his hope rather than expectation that the outbreak could be contained.117 Dr Calderwood subsequently shared this with the Chief Medical Officers for England, Wales and Northern Ireland and others.118 Reflecting on his reaction to Professor Woolhouse’s email of 25 January 2020 during his evidence to the Inquiry, Professor McBride said that this email “raised a level of concern”. However, he also said: “[A]t that time it had the potential not to be so significant, and I think that, you know, planning and preparing in uncertainty is extremely difficult. ”.119 |
| 2.47. | Professor Woolhouse also contacted Dr Calderwood the following day, reiterating the need for public health measures. He explained that case isolation, infection control and contact tracing would be “the mainstay of any control effort for this virus” and they became “more difficult to implement as the numbers of cases rise and resources are stretched”.120 He also emphasised the importance of public messaging and social distancing.121 |
| 2.48. | That same day, Dr Atherton met with Public Health Wales to agree strategic aims and actions, including monitoring and assessing the risk to the public, facilitating detection, case management and isolation, developing a diagnostic pathway for the virus (a route from a person presenting symptoms to being diagnosed), developing guidance for health professionals and facilitating communication across different partners in Wales.122 Regular meetings continued.123 |
| 2.49. | On 27 January 2020, the UK government advised that arrivals from Wuhan should self-isolate for 14 days.124 A few days later, the Welsh Government extended its self-isolation guidance to arrivals from all of mainland China who developed flu-like symptoms.125 Guidance was updated throughout January and February.126 |
| 2.50. | Health Protection Scotland initiated its Incident and Emergency Response Plan on 27 January 2020 as part of the planned response to an emergency where the scale of the actual or potential public health concern was deemed to be beyond normal response capabilities.127 Similarly, the Department of Health (Northern Ireland) activated its Emergency Operations Centre, which managed the flow of information through the department as part of its Emergency Response Plan.128 |
| 2.51. | On 28 January 2020, Professor Whitty emailed William Warr, Special Adviser to the Prime Minister for Health, Social Care, Life Sciences and Technology, about the possible scenarios that might develop in terms of the impact on the UK.129 He explained that only two of four potential scenarios were “probably worth considering for planning at this point”.130 One was a major outbreak in China that was brought under control, with any cases seeded in other countries, including the UK, not leading to “sustained onward transmission”.131 The other “opposite end of the risk scale” was that the virus could, within the next few weeks, “become widespread and turn into a significant pandemic relatively quickly”.132 He said that this was the “reasonable worst case scenario for which plans are also being developed”, using the influenza pandemic plans as “a base case”, without the benefit of a vaccine or antivirals.133 Professor Whitty noted:
“[T]he economic consequences of over-calling can be substantial, but the mortality and social consequences of under-calling are even more substantial ”.134 Professor Vallance agreed.135 Professor Whitty also explained: “The main aim of current UK planning in public health terms is [to] ensure we do not have outbreaks from index travellers, so that if the epidemic is brought under control it has had minimal impact on the UK”.136 This reflected the approach set out in the UK Influenza Pandemic Preparedness Strategy 2011.137 |
| 2.52. | At a meeting on 28 January 2020, SAGE set out its understanding of a number of important features of Covid-19, including:
This meant that Covid-19 was likely to spread quickly. At the meeting, the Scientific Pandemic Influenza Group on Modelling (a pre-existing standing science advisory group convened by the Department of Health and Social Care) was formally redeployed as SPI-M-O (a sub-group of SAGE). SPI-M-O was asked by SAGE to “advise on actions the UK could take to slow down the spread of the outbreak domestically, even if widespread globally”.139 In the early stages of the pandemic, one of SAGE’s main priorities was to establish the likely impact of Covid-19 if it arrived in the UK. The ability of the scientific advisory groups to do this was hampered by a lack of data at the time, which meant that a reasonable worst-case scenario could not easily be formulated. (As set out in Chapter 1: The context for pandemic decision-making, in this volume, a reasonable worst-case scenario is a tool used in risk assessment processes to prepare for “a challenging yet plausible manifestation of the risk”.)140 At the end of January 2020, SAGE agreed that the reasonable worst-case scenario for pandemic influenza where no vaccine or specific treatment is available – which anticipated 820,000 excess deaths – should be used for government planning purposes until sufficient data had emerged.141 |
| 2.53. | Professor Van-Tam described SAGE’s decision to base the reasonable worst-case scenario on pandemic influenza planning as:
“a perfectly reasonable approach to adopt. There was no other respiratory virus that had hitherto caused a known human pandemic that could reasonably direct our response ”.142 |
| 2.54. | SAGE considered that the triggers which would require a change in the UK government’s approach were “sustained human-to-human transmission outsideChina and or a severe UK case”.143 It also advised that “[p]andemic influenza infection control guidance should be used as a base case and adapted”.144 |
| 2.55. | Testing capacity across the UK was exceptionally limited in January and February 2020. For example, the SAGE minutes from 28 January recorded that there would only be capacity to “run 400 to 500 tests per day” by the end of the week in the UK.145 SAGE described this capacity as “limited” and noted that it could not “be substantially increased during this winter influenza season”.146 |
| 2.56. | Covid-19 was discussed by the Scottish Cabinet for the first time on 28 January 2020. It was noted that there was some evidence of pre-symptomatic transmission from China, which was considered “alarming”.147 The Scottish Government Resilience Room was activated on 29 January, following discussions between government officials and Jeane Freeman MSP (Cabinet Secretary for Health and Sport in the Scottish Government from June 2018 to May 2021) becoming aware that it was likely that the first positive case had reached the UK.148 |
| 2.57. | On 28 January 2020, NERVTAG advised that there was “no evidence to support that the wearing of face masks by the general public reduces transmission”, noting a risk that advising the public to do so “may add to fear and anxiety”.149 |
| 2.58. | That same day, Professor McBride noted in a WhatsApp group including the Chief Medical Officers for England, Wales and Scotland and Professor Van-Tam that reports appeared “to be consistent with asymptomatic transmission during the incubation period”.150 Professor Whitty agreed that it was:
“[c]ompatible, probable but not conclusive … But we should now assume it may be happening ”.151 Professor Whitty advised Mr Hancock and officials from the Department of Health and Social Care that there was: “now credible evidence of asymptomatic transmission within Germany (resulting from the timings of the transmission) ”.152 |
| 2.59. | Mr Hancock told the Inquiry that, on 29 January 2020, Professor Whitty proposed four elements to the plan: contain outbreaks, delay spread, mitigate the effects on the population and, throughout, research treatments and a vaccine.153 Professor Whitty described this strategy, which began to be identified in late January 2020, as being based on a “contain, delay, research and mitigate” framework.154 |
| 2.60. | At a COBR meeting on 29 January 2020, Professor Whitty stated:
“There were two scenarios to be considered. The first was that the spread was confined within China, the second was that the spread was not limited to China and there would be a pandemic like scenario, with the UK impacted. The second scenario was plausible but it may take weeks to months”.155 He described “a 10 per cent likelihood” (a 1 in 10 chance) of the reasonable worst-case scenario occurring, but stated that this had not been agreed by SAGE.156 |
| 2.61. | On the same day, an article was published by the Chinese 2019-nCoV Outbreak Joint Field Epidemiology Investigation Team. It estimated, based on research of the first 425 cases, that R0 was 2.2 (ie one person would infect, on average, 2.2 others) and stated that there was evidence that person-to-person transmission had occurred among close contacts since mid-December 2019.157 The article concluded:
“Considerable efforts to reduce transmission will be required to control outbreaks if similar dynamics apply elsewhere. Measures to prevent or reduce transmission should be implemented in populations at risk”.158 |
| 2.62. | On 30 January 2020, the World Health Organization declared a Public Health Emergency of International Concern – recognising Covid-19 as an extraordinary event that constituted a public health risk through the international spread of disease and could require immediate international action.159 That day, the UK risk level was raised from ‘low’ to ‘moderate’ by the UK’s four Chief Medical Officers.160 NHS England also declared a Level 4 Major Incident (the highest category of emergency under the NHS England Emergency Preparedness, Resilience and Response Framework), requiring NHS England National Command and Control to support the NHS response in England.161 As a result, NHS England was required to apprise the Department of Health and Social Care (as the lead government department) and ministers of progress and impact.162 The following day, the Department of Health and Social Care established a team to coordinate the procurement of personal protective equipment (PPE) and the Pandemic Influenza Preparedness Programme stockpile was made available for release to supplement usual supply chains.163 |
| 2.63. | Also on 30 January 2020, a briefing note to Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021, and Michelle O’Neill MLA (deputy First Minister of Northern Ireland from January 2020 to February 2022) provided an update from COBR. It noted that the Department of Health (Northern Ireland), “as the lead government department”, was closely monitoring the rapidly evolving situation.164 It also explained that the clinical effects of Covid-19 “range from asymptomatic to a relatively mild illness through to pneumonia” and that the elderly and those with existing health conditions would be disproportionately affected.165 |
| 2.64. | On 31 January 2020, Covid-19 was discussed for the first time at a meeting of the UK Cabinet. The advance briefing for Mr Johnson advised that COBR had agreed to:
“use the reasonable worst case for pandemic flu to guide planning, and build on the existing work that is continuously underway for pandemic flu”.166 Mr Hancock indicated to the Cabinet that if China “did not grip the situation it could become global. That would be very serious, including for the UK.”167 Mr Hancock told the Inquiry that he had informed the Cabinet that as many as 820,000 people in the UK might die in the reasonable worst-case scenario, although this was not recorded in the minutes.168 |
| 2.65. | By the end of January 2020, in addition to the 9,826 cases reported around the world across 18 countries, the first case of Covid-19 had been confirmed in the UK – a 23-year-old Chinese student who had travelled to York from Hubei province in China.169 On 31 January, it was announced that the student and his mother had tested positive for Covid-19.170 There were also four cases in both France and Germany.171 That same day, China imposed regional lockdowns and travel restrictions. |
The situation at the end of January 2020
| 2.66. | By the end of January 2020, it was clear that a fatal respiratory disease – more severe and lethal than H1N1 influenza (‘swine flu’) – was spreading across the world, transmitted person to person and possibly asymptomatically. It had reached the UK. There was, as yet, no drug to alleviate the disease and no vaccine to prevent it. |
| 2.67. | Although the existing procedures for the identification and testing of high consequence infectious diseases had revealed the first two confirmed cases of Covid-19, test and trace capacity was still limited throughout the UK.172 Professor Whitty acknowledged:
“Scale-up was our great weakness in our response at the start of the pandemic; we had significant scientific capability, but little scale-up capacity to meet the needs of an exponentially rising epidemic”.173 It is difficult to see, therefore, how the UK would be able to identify or contain a rapidly spreading disease. |
| 2.68. | The limited testing capacity, combined with a lack of adequate surveillance mechanisms, also meant that decision-makers did not appreciate the extent to which the virus was capable of spreading – and was indeed spreading – undetected. |
| 2.69. | This was compounded by uncertainty that lingered over the degree of asymptomatic transmission.174 As Mr Johnson said, this uncertainty:
“bedevilled our handling of the virus, certainly in the early weeks, and probably caused us to underestimate the speed with which it was seeding in the UK”.175 His approach at this point was recorded in the Cabinet meeting minutes on 31 January 2020: “[T]he tone of the Government should be reassurance, given the low mortality rate. People should not panic”.176 Mr Johnson further explained: “Initially, we completely misunderstood asymptomatic transmission and, as a result, it did not impact our decision making in relation to NPIs [non-pharmaceutical interventions]. However, by early April 2020 we did understand that Covid could be transmitted in the early stages of contracting the virus and we took that into account thereafter.”177 |
| 2.70. | Mr Hancock told the Inquiry:
“[T]he scientific consensus, reflected in the global scientific advice from the WHO until April 2020, was that there was no asymptomatic transmission … despite anecdotal feedback from January 2020 that the virus could pass from people who showed no symptoms”.178 Mr Hancock said that he “challenged the scientific advice on a number of occasions” but that he “could not simply over-rule this global scientific consensus on a lack of asymptomatic transmission”.179 With hindsight, he regretted not acting on the basis of asymptomatic transmission prior to April 2020.180 |
| 2.71. | Ms Sturgeon also said that there was a “significant degree of uncertainty in the advice being provided” in this period about the likely severity of the situation in the UK and the key characteristics of the virus.181 She noted that the understanding about asymptomatic transmission – although reflective of scientific consensus – turned out to be “wrong”.182 Professor McBride suggested that, in the absence of evidence, it would have been “premature” to assume that there was asymptomatic transmission.183 He said:
“[A]t this stage, there was a high level of uncertainty, and I think it would have been not appropriate to proceed on the basis of what we think … And at this point in time, NERVTAG, SAGE were not saying that there is asymptomatic transmission. But we were alert to the fact that we needed to keep this under review to see if there was or there wasn’t”.184 |
| 2.72. | According to Mr Drakeford, “during January and February there was some limited and preliminary evidence which suggested the possibility of asymptomatic spread”, but it was not “well-understood” until late April 2020.185 Mr Swann told the Inquiry that “acceptance of asymptomatic transmission came about May of 2020”.186 |
| 2.73. | However, as set out above, there were clear signs by late January 2020 that suggested asymptomatic transmission was taking place.187 Mr Hancock had been informed by a number of advisers, including the Chief Medical Officer for England, that there were indications that asymptomatic transmission was occurring in Europe. He himself opened a meeting on 27 January:
“by outlining his concern upon hearing the update from the Chinese government that the virus is transmissible when patients are asymptomatic”.188 On 28 January, Mr Hancock was further informed of: “now credible evidence of asymptomatic transmission within Germany (resulting from the timings of the transmission)”.189 |
| 2.74. | This, coupled with the discussion on the same date between the four Chief Medical Officers of the UK, in which it was noted that they should “assume it may be happening”, ought to have led the four governments to adopt the default assumption that asymptomatic transmission was occurring and was a potentially significant factor in how the virus was spreading.190 |
| 2.75. | Although there were difficulties caused by the lack of data and more precise knowledge of the characteristics of the disease, the absence of accurate data was not sufficient justification for the failures to prepare for a potentially significant health emergency. There was significant geographical spread beyond China, which gave a strong indication of sustained person-to-person transmission – one of Professor Whitty’s three triggers. There was emerging evidence that asymptomatic transmission could be taking place. In the absence of scaled-up test and trace capacity, there were no practical means available in the UK to prevent the spread of the virus. The virus therefore posed a serious and immediate threat. |
| 2.76. | UK government scientific advisory bodies had been convened in good time. Professors Whitty and Vallance also took appropriate steps to warn the UK government that, if Covid-19 turned into a pandemic, there was likely to be very significant loss of life in the UK. Some officials in the UK government and devolved administrations had been warned that, if the reasonable worst-case scenario materialised, there was likely to be very significant loss of life, but action was limited. At meetings on 28 January and 4 February 2020, UK ministers were told – and clearly understood in some cases – that the UK was “looking at the risk of an epidemiological human catastrophe on a scale not seen in the UK for a century”.191 However, the chances of that risk materialising were not sufficiently appreciated. |
| 2.77. | Mr Hancock said that he called Mr Johnson directly on at least four occasions during January 2020 to warn him of the risk and “to try and impress upon him my concerns as to the potential impact from the virus”.192 He also said he was astonished that others did not seem interested.193 For his part, Mr Johnson stated that he “did not minimise the possibility that this virus could be dangerous” and asked Mr Hancock to keep him updated.194 The emergence of a novel coronavirus was only “one of many issues crossing the Prime Minister’s desk” in January 2020.195 Lee Cain, Director of Communications at 10 Downing Street from July 2019 to November 2020, told the Inquiry that Covid-19:
“was a low priority at this time due to the uncertain nature of the threat combined with reassurance from the Cabinet Office and Department for Health that ‘pandemic planning’ was robust if required … While Covid was monitored in Downing Street in January 2020 it was not considered as the most pressing issue … or even in the top five”.196 |
| 2.78. | For their part, the devolved administrations failed to escalate consideration of the emerging crisis to their highest levels of government (Cabinets in Scotland and Wales and the Northern Ireland Executive Committee) with sufficient speed. It was only on 28 January 2020 that Humza Yousaf MSP, Cabinet Secretary for Justice in the Scottish Government from June 2018 to May 2021, suggested “significant alarm was raised in relation to the potential effect Covid-19 would have”.197 Neither the Welsh Cabinet nor the recently reconstituted Northern Ireland Executive addressed Covid-19 during January 2020.198 Instead, in Wales, the Cabinet focus was primarily on arrangements for the UK’s exit from the EU, budget concerns and adverse weather, with no Covid-19 cases reported in Wales. Mr Drakeford told the Inquiry that “at that point it is happening elsewhere”.199 However, given the warning sounded by Dr Atherton on 24 January 2020 and the clear signs of the virus’s growing threat, the Welsh Government should have recognised the potential danger in late January 2020. |
| 2.79. | Although it was understandable that directing the response to the outbreak was not yet the absolute priority of the leaders of the four nations, there was insufficient attention paid to the emerging crisis at the highest levels of the government machinery. The multitude of meetings and papers failed to translate into immediate action. |
| 2.80. | It should also have been more quickly appreciated by all four governments – in light of the emerging knowledge about the virus’s reproduction number, incubation period, severity and ability to transmit asymptomatically – that an approach based on the UK Influenza Pandemic Preparedness Strategy 2011 was flawed and reliance upon it was misplaced.200 It was clear by the end of January 2020 that the UK was facing a virus with different characteristics from the one for which it had planned. The knowledge about the precise degree of difference might still have been evolving, but enough was known to indicate that plans would have to be revised, with a proper consideration of a centrally led, cross-government strategy and response, including the identification of potential interventions. |
February 2020: The spread of the virus
| 2.81. | By 1 February 2020, about 12,000 cases of Covid-19 had been confirmed worldwide, 132 of which were in 23 countries outside China – 259 deaths had been reported.201 Assessments of key features of the virus had also developed further. In an email to Professor Whitty on 2 February, Professor Ferguson gave a central estimate of the case fatality ratio as “1.5-1.8%”.202 This would mean that, for every 100 diagnosed cases of a disease, 1.5 to 1.8 people would die. SAGE advised that “[s]ustained community transmission outside China should be expected”, although there was not yet “definitive evidence of a sustained outbreak/epidemic elsewhere”.203 |
| 2.82. | A UK-wide public information campaign was launched on 2 February 2020 by the Department of Health and Social Care, advising the population to adopt respiratory and hand-hygiene measures.204 |
| 2.83. | In early February 2020, travel restrictions were considered again by scientific advisers, but the consensus was that these would achieve only a limited delay.205 SPI-M-O concluded that “the average delay expected to result from a 90% reduction of travel from China may be up to two weeks”.206 SAGE noted that “draconian and coordinated measures” would be required to sufficiently reduce the number of imported infections and that “direct flights from China [were] not the only route for infected individuals to enter the UK”.207 Professor Whitty relayed this advice to COBR shortly afterwards.208 |
| 2.84. | On 3 February 2020, NERVTAG advised that people with Covid-19 symptoms should wear a face covering, but again stated that the precautionary use of face coverings by people without symptoms was not recommended.209 This was based on its view that the evidence for the use of face coverings by the general public was “near nil”, that risk of exposure in the community was hard to predict and it was likely that compliance would be poor.210 The following day, SAGE considered NERVTAG’s advice that there was “limited to no evidence of the benefits of the general public wearing facemasks as a preventative measure”.211 SAGE endorsed NERVTAG’s advice that face coverings should only be worn by people with Covid-19 symptoms and by health and social care workers who were visiting people who might be infectious.212 SAGE also provided advice on mass gatherings on 4 February.213 It advised there was little evidence that cancelling or banning mass gatherings would have a significant effect in reducing transmission of the virus. It reiterated this advice on 13 and 27 February.214 |
| 2.85. | In its Strategic Preparedness and Response Plan of 4 February 2020, the World Health Organization issued guidance recommending:
“[s]caling up country preparedness and response operations, including strengthening readiness to rapidly identify, diagnose and treat cases; identification and follow-up of contacts when feasible (with priority given to high-risk settings such as healthcare facilities); infection prevention and control in healthcare settings; implementation of health measures for travelers; and awareness raising in the population though [sic] risk communication and community engagement”.215 |
| 2.86. | At a departmental performance meeting on 4 February 2020 between the Prime Minister and the Department of Health and Social Care, Professor Whitty briefed Mr Johnson on Covid-19 for the first time.216 He informed Mr Johnson that a major pandemic with 100,000 to 300,000 deaths in the UK was possible.217 Mr Johnson was “in listening mode”, according to Sir Christopher Wormald.218 Following a discussion over possible fatality numbers, Mr Johnson noted that high fatality figures had been given for bovine spongiform encephalopathy (BSE, often referred to as ‘mad cow disease’ and causing variant Creutzfeldt–Jakob disease in humans) and swine flu. His demeanour was described as “concern mixed with a level of scepticism”.219 |
| 2.87. | According to Professor Whitty:
“My principal aim in this meeting was to ensure that the Prime Minister understood that if COVID-19 turned into a pandemic there was likely to be very significant loss of life in the UK. He heard the advice and in my view understood it; I have no way of telling whether he believed it. It was a relatively brief discussion”220 |
| 2.88. | Mr Johnson accepted generally that he did not take warnings seriously enough:
“[W]hen you read that an Asiatic pandemic is about to sweep the world … you think you’ve heard it before, and that was the problem”221 He explained that he had: “a basic confidence that things would turn out all right, on the fallacious inductive logic that we’d had Asian zoonotic scares before, and they had turned out all right”.222 Mr Johnson also acknowledged that he had been lulled into a false sense of security by his belief that earlier outbreaks had been “exaggerated”:223 “I think that in that period, January really to the end of February, towards the end of February, Covid was pretty much like a cloud on the horizon, no bigger than a man’s hand, and you didn’t know whether it was going to turn into a typhoon or not.”224 |
| 2.89. | On 4 February 2020, the Scottish Cabinet met in accordance with its usual schedule. Covid-19 received little attention at the meeting. It was noted that the virus had reached the UK, although no positive cases in Scotland had been identified. The Scottish Government Resilience Room continued to “monitor the situation” and preparations were said to be “in hand, based on a reasonable worst case scenario of a situation similar to an influenza pandemic”.225 An accompanying paper referred to directorates “planning, in the first instance, to stand up pandemic flu plans”.226 |
| 2.90. | The following day, Professor Woolhouse sought the involvement of Professor Dame Sally Davies, Chief Medical Officer for England from June 2010 to October 2019, telling her to “get Catherine [Calderwood] to listen to me, because she’s not listening”.227 Professor Davies then emailed Dr Calderwood to “introduce” Professor Woolhouse and suggested that Dr Calderwood might “benefit” from having a conversation with him, particularly in relation to Scotland’s preparedness.228 Although Dr Calderwood sought to reassure Professor Woolhouse that adequate steps were being taken, he was concerned by what he saw as her lack of engagement.229 |
| 2.91. | In Wales, Reg Kilpatrick, Director in the Welsh Government with responsibility for civil contingencies from 2013, convened a meeting of the Civil Contingencies Group (Wales) on 4 February 2020, in accordance with the Pan-Wales Response Plan, to allow officials to “begin to plan”.230 He told the Inquiry that it:
“seemed to me at the end of January we were in the position where there was a potential for coronavirus to come to the UK and therefore to come to Wales”.231 However, there was some confusion even in the latter part of February about the extent of the operations of the Emergency Coordination Centre (Wales) and whether it “was ready to ‘stand up’ if and when required”.232 While Dr Quentin Sandifer, Executive Director for Public Health Services and Medical Director at Public Health Wales from October 2012 to December 2020, was informed that the Emergency Coordination Centre (Wales) had been stood up, he “didn’t recognise its functions in terms of the Pan Wales Response plan”.233 Mr Kilpatrick accepted that “we should have been clearer”.234 The triggers for the establishment of the Emergency Coordination Centre (Wales) must be reviewed – something which the Welsh Government has acknowledged.235 |
| 2.92. | The Northern Ireland Executive Committee was first briefed by the Minister of Health “on protection measures against the Coronavirus” at its meeting of 3 February 2020, although its first substantive discussion did not take place until 2 March 2020.236 David Sterling (later Sir David Sterling), Head of the Northern Ireland Civil Service and Permanent Secretary to The Executive Office from June 2017 to August 2020, attended a ‘Wednesday Morning Colleagues’ meeting in the Cabinet Office on 5 February, at which Professor Whitty gave an update on Covid-19. Sir David Sterling recalled Professor Whitty saying that “in his view the Chinese government had not got to grips with this and that it would almost certainly become a global pandemic”.237 |
| 2.93. | On 5 February 2020, the daily commonly recognised information picture (CRIP, a summary of information from the Civil Contingencies Secretariat made available to COBR) stated that two of Professor Whitty’s triggers had “been met, resulting in the increase in risk assessment on 21 January”.238 |
| 2.94. | COBR met again on 5 February 2020.239 The health ministers and Chief Medical Officers for the devolved administrations were in attendance and were provided with the CRIP. COBR was informed that the case fatality ratio was estimated to be 2% to 3% and that the two most high-risk groups appeared to be the elderly and those with pre-existing illnesses.240 Mr Hancock also noted that “there were no legal powers in place to force nationals into isolation” and COBR decided not to close the borders for arrivals from China.241 It also resolved to develop plans for an emergency bill to support the UK’s pandemic response, with an action item for all departments and devolved administrations to finalise their policy inputs for the proposed legislation.242 The first coronavirus laws – the Health Protection (Coronavirus) Regulations 2020 – were introduced in the UK Parliament a few days later under the Public Health (Control of Disease) Act 1984.243 This enabled the Secretary of State to declare an emergency and activate emergency powers, which Mr Hancock did on 10 February.244 |
| 2.95. | On 6 February 2020, SAGE advised of a third UK case of a person testing positive for Covid-19.245 It stated that “[i]n light of new evidence of human-to-human transmission beyond China … the UK geographical case definition should be widened” to include individuals who were showing possible symptoms and had travelled from a number of other countries, including Thailand, Japan and the Republic of Korea.246 This evidence of transmission occurring outside China was the third of Professor Whitty’s three triggers. That same day, Mr Cummings sent a message to a 10 Downing Street WhatsApp group saying that the “Chief Scientist” had told him that “it’s prob out of control now and will sweep world”.247 |
| 2.96. | At a Cabinet meeting on 6 February 2020, Mr Johnson observed:
“[C]onfidence was also contagious, and it was important that the Government remain measured in its response … Often the significant economic damage of a crisis came from political overreaction rather than the problem itself. This had been true of Bovine spongiform encephalopathy (BSE).”248 Mr Hancock was similarly reassuring, stating: “Whilst the virus spread easily, it was better news that the mortality rate was only around 2 per cent … The central point to make was that the Government had a plan to deal with this illness, and this was guided by science.”249 As set out above, the only ‘plan’ was the UK Influenza Pandemic Preparedness Strategy 2011 , and it was inadequate to cope with the threat of the new virus.250 |
| 2.97. | That same day, Liz Redmond, Director of Population Health, advised The Executive Office that it was not necessary to activate the contingency arrangements for civil emergencies (Northern Ireland Central Crisis Management Arrangements, known as NICCMA) “unless or until” Covid-19 appeared in Northern Ireland.251 This was despite the NICCMA Protocol anticipating that, where there was a UK-wide risk and COBR was activated, Northern Ireland would convene an equivalent body.252 |
| 2.98. | Also on 6 February 2020, Professor McBride advised all Northern Ireland government departments and public authorities to ensure that staff were acquainted with contingency plans for responding to infectious diseases, but that otherwise no action was required at that stage.253 An aide-memoire prepared for Mr Pengelly set out:
“I do not consider it necessary to activate [NICCMA] at this time, however, this is an evolving situation and preparedness across NI [Northern Ireland] is critical.”254 As a result, the Department of Health (Northern Ireland) remained the lead government department for the response to the pandemic at this time.255 |
| 2.99. | On 7 February 2020, Public Health England announced the rollout of Covid-19 testing to 12 laboratories across the country.256 A joint letter from Public Health England, the National Medical Director, NHS England and Professor Whitty was also issued to NHS organisations implementing the earlier SAGE advice on travellers:
“[A]ll travellers who develop relevant symptoms, however mild, within 14 days of returning from mainland China, Thailand, Japan, Republic of Korea, Hong Kong, Taiwan, Singapore, Malaysia or Macau should self-isolate at home immediately and call NHS 111.” [the non-emergency NHS helpline].”257 Similar advice was issued in Wales, Scotland and Northern Ireland.258 |
| 2.100. | On 10 February 2020, Imperial College London published Report 4: Severity of 2019-Novel Coronavirus (nCoV), which gave an overall case fatality ratio for “all infections (asymptomatic or symptomatic) of approximately 1%”.259 A 1% case fatality ratio in all infections, as opposed to just in confirmed cases, represented a serious degree of lethality (the comparable rate for swine flu was approximately 0.01% to 0.02%).260 That same day, SPI-M-O advised that it was a realistic probability that outbreaks outside China could not be contained by isolation and contact tracing. If a high proportion of asymptomatic cases were infectious, then, it stated, containment was unlikely to be achieved through those policies alone.261 |
| 2.101. | That same day, following discussions with Mr Cummings, Professor Vallance met Mr Johnson for the specific purpose of briefing him on the pandemic and to ensure that Mr Johnson “understood how important and dangerous this was”.262 Professor Vallance said:
“I think the Prime Minister expressed a view that he thought the problem would be contained but there was no doubt that Mr Cummings and the No. 10 team understood the level of concern.”263 |
| 2.102. | Despite this, Mr Johnson told the Inquiry that, by mid-February:
“I think it would be fair to say that the scientific community within Whitehall at that stage was not telling us, I was not being informed, that this was something that was going to require urgent and immediate action.”264 Mr Cain also said that Mr Johnson was: “receiving assurances that … everything actually is being well prepared and we are in a good situation to handle things … nobody’s sort of setting up the warning flares to him or to the core team.”265 Stuart Glassborow, Deputy Principal Private Secretary to the Prime Minister from May 2019 to May 2022, told the Inquiry: “I do not believe the Prime Minister was advised at this early stage as to the likely scale of the impending challenge.”266 If Professor Vallance did advise the Prime Minister of the danger facing the UK – as seems likely – not enough was done in response. |
| 2.103. | On 10 February 2020, Mr Hancock commissioned “a coronavirus version” of the UK Influenza Pandemic Preparedness Strategy 2011 to be prepared.267 |
| 2.104. | By 11 February 2020, the UK had “8 confirmed cases, all of whom acquired the virus overseas”.268 |
| 2.105. | An estimate provided by SPI-M-O to the meeting of SAGE on 11 February 2020 suggested that the number of confirmed cases in China was 10 times higher than the number currently confirmed. SPI-M-O reiterated its earlier advice and stated:
“It is a realistic probability that there is already sustained transmission in the UK, or that it will become established in the coming weeks.”269 SAGE noted that it was “important to understand hospital bed requirements” and identified that SPI-M-O should: “work with NHSE [NHS England] and others on modelling the impact of the pandemic influenza reasonable worst case on the NHS, including the number of people requiring respiratory support”.270 SAGE advised that the UK government should continue to plan using the influenza pandemic assumptions, but again identified important differences between the viruses. In checking its understanding of Covid-19 against planning assumptions, it expressly compared characteristics of influenza viruses with those of Covid-19 in the form of a table. This table: “was adapted and updated repeatedly in February and March, with the intention of checking what was known about the virus against the planning assumptions that underlay the pandemic influenza [reasonable worst-case scenario], and hence assessing the extent to which planning for pandemic influenza served as a useful guide”.271 SAGE confirmed that asymptomatic transmission “cannot be ruled out”. Its working assumptions were that Covid-19 had a longer incubation period than pandemic influenza, a similar case fatality ratio, a longer duration of illness and potentially a longer average duration of infectivity to others (the length of time an infected individual remains able to transmit a virus).272 A longer incubation period was potentially significant because it would increase the window of opportunity for tracing people who had been in close contact with infected individuals before they became infectious themselves. |
| 2.106. | Mr Kilpatrick forwarded the table to officials within the Welsh Government, noting:
“This material needs to be shared internally and rapidly … for information and to underline the potential seriousness of the issue.”.273 |
| 2.107. | On 12 February 2020, a ministerial table top exercise – Exercise Nimbus – was held. Representatives of the health departments in the devolved administrations also attended.274 It imagined a fictional COBR meeting taking place in April 2020 in order to test decision-making processes and strategies.275 Ms Freeman (who did not attend the exercise herself) understood that the purpose of the exercise was to:
“update or double check planning against the flu pandemic … which had informed most of government planning prior to Covid-19”.276 |
| 2.108. | It is, however, unclear whether any practical benefits were achieved. Dr Ben Warner, Special Adviser to the Prime Minister from December 2019 to May 2021:
“did not think this exercise had stress tested the Government’s overall pandemic response in any meaningful way”.277 In particular, reflecting the UK Influenza Pandemic Preparedness Strategy 2011, Exercise Nimbus focused on health impacts and managing the large numbers of deaths that ‘occurred’ under the assumed reasonable worst-case scenario, rather than on controlling the spread of the virus or preventing deaths.278 |
| 2.109. | Mr Swann, who attended Exercise Nimbus on behalf of Northern Ireland, had no memory of it, which he thought was because it had no impact.279 Vaughan Gething MS, Minister for Health and Social Services in the Welsh Government from May 2016 to May 2021, said:
“We never got to the point that Operation Nimbus envisaged. So the choices that ministers were being asked to envisage there, I think it was a[s] real as it could have been, to have been helpful.”.280 Its utility was also limited by the absence of many relevant decision-makers. According to Mr Hancock, “most Government Departments had sent junior ministers, many of whom were about to be moved” in any event due to a reshuffle.281 |
| 2.110. | SAGE met again on 13 February 2020, noting:
“SAGE and wider HMG [Her Majesty’s Government] should continue to work on the assumption that China will be unable to contain the epidemic.”.282 |
| 2.111. | The UK Cabinet met the following day, on 14 February 2020. Mr Johnson warned that “the government and the country needed to be ready for the coronavirus situation to get worse”.283 This was the first occasion on which Professor Whitty briefed the Cabinet directly on Covid-19. He told them:
“If the virus spread beyond China to its neighbours and across the world, then the UK would not be immune. Either the whole world would be affected, or the virus would be effectively restricted to China. There was no in-between scenario.”284 Professor Whitty also advised: “[T]he spread of the virus would not be stopped by the suspension of flights from China. If the UK suspended flights, the modelling showed that it would only slow the spread of the virus by a maximum of five days. If the whole of the EU suspended flights from China then the virus may be slowed by two to four weeks.”285 This reflected the consistent advice given by scientists, that: “completely closing borders would achieve very little in the way of epidemiological protection; it would only delay and there were other reasons why it did not seem advisable at the time, for example, making sure we had access to supplies from overseas and the need to repatriate UK nationals”.286 Professor Whitty said that, if the virus became widespread in the UK, “[t]he plans that were already in place to tackle an influenza epidemic would be needed”.287 While it was possible that the virus would die out naturally as the seasons changed, if it did not, Professor Whitty expected up to 50% of the population to be affected with symptoms. Mr Hancock reiterated that “the Government had a plan, informed by science”.288 |
| 2.112. | That same day, NHS Supply Chain (a body that procures healthcare products for NHS trusts and healthcare organisations) was provided with delegated authority to conduct significant spending on the open market for items of PPE that were of most concern. This followed earlier instructions by the Department of Health and Social Care to purchase additional volumes of PPE.289 |
| 2.113. | The World Health Organization published guidance on 14 February 2020, which stated:
“There is ample evidence that mass gatherings can amplify the spread of infectious diseases … Such infections can be transmitted during a mass gathering, during transit to and from the event, and in participants’ home communities upon their return.”290 However, no decision was yet taken on cancelling mass gatherings throughout the UK. |
| 2.114. | The UK Cabinet was not convened between 14 and 25 February 2020. There was also no COBR between 19 and 26 February 2020. It was school half-term holidays and parliamentary recess. Mr Johnson, staying at Chevening House (a country residence used by Foreign Secretaries), continued to receive box notes and sent three returns back to 10 Downing Street.291 It does not appear that he was briefed, at all or to any significant extent, on Covid-19 and he received no daily updates.292 |
| 2.115. | Mr Cummings observed that his general view of the Cabinet Office and the Department of Health and Social Care at this time was that they “weren’t banging alarm bells at this point. Far from it, they were going skiing.”293 |
| 2.116. | On 17 February 2020, SPI-M-O noted:
“There were differing views within the group about the likelihood of sustained transmission in the UK both currently and in the near future. Some believe it is a realistic possibility that sustained transmission in the UK will become established in the coming weeks while others believe this likelihood is higher and that there may already be sustained transmission.”294 |
| 2.117. | John Swinney MSP, Deputy First Minister of Scotland from November 2014 to March 2023, chaired a Scottish Government Resilience Room meeting on 17 February 2020 to review the current situation.295 The Scottish Cabinet met the following day, noting that “extensive work” was under way to prepare for any outbreak in Scotland, including an assessment of the vulnerability of the social care sector.296 Analysis prepared in advance of the Cabinet meeting included one scenario involving a 12 to 15-week pandemic, with a mortality rate of 2.5%, or 68,000 people.297 The note of the Cabinet meeting does not record whether this potential scenario was specifically discussed, although Ms Sturgeon introduced the briefing paper (which covered a number of topics).298 |
| 2.118. | At its eighth meeting, on 18 February 2020, SAGE noted that Public Health England could cope with only five new Covid-19 cases per week (requiring isolation of 800 contacts), although:
“Modelling suggests this capacity could be increased to 50 new cases a week (8,000 contact isolations) but this assumption needs to be stress tested with PHE operational colleagues.”299 |
| 2.119. | Professor Yvonne Doyle, Medical Director at Public Health England from June 2019 to October 2021, explained to the Inquiry that this was not correct. The five cases were references to new cases imported into the country with the capacity to trace the chain of transmission generated from these, amounting to about 2,000 onward contacts for each case imported into the UK. The underlying point was that this “would rapidly get out of control”.300 It was correct that Public Health England had limited capacity – it was “not remitted to”, nor was it:
“set up – in manpower capacity, workforce, facilities or funding – to address a pandemic of the scale of COVID-19 and mass population-level testing.”301 |
| 2.120. | The London School of Hygiene & Tropical Medicine had concluded earlier in February 2020 that “60-80% of contacts must be traced (and transmission stopped) in order to achieve control in most scenarios, and more for some characteristics”.302 The UK did not have the ability to do so. Demand would rapidly outpace Public Health England’s capacity. Nonetheless, Public Health England retained responsibility for testing and tracing until early April. |
| 2.121. | A meeting of COBR was also held on 18 February 2020 (chaired by Mr Hancock but attended for the first time by the leader of a devolved administration, Mr Drakeford). Professor Whitty stated:
“Both escalation to a global pandemic, and isolation of the majority of cases to China remained realistic possibilities.”303 A legislative policy paper presented to COBR confirmed that a “full response to an outbreak of Covid-19 in the UK will require additional UK legislation”.304 Mr Drakeford stated that his “very clear impression” was that the choice of legislation under which emergency powers would be exercised would be a decision for the UK government.305 Ms Sturgeon agreed.306 (This is considered further in Chapter 13: Legislation and enforcement, in Volume II.) The Civil Contingencies Secretariat also provided an update on planning, noting: “[T]here was work to be done to create a clear plan of activity (across the UK Government) from the moment of sustained transmission to its estimated peak, which was likely to be a period of three months.”307 |
| 2.122. | At its meeting on 20 February 2020, SAGE noted that individual cases in England could already have been missed.308 The minutes highlighted that, before consideration of measures to reduce the spread could be meaningfully undertaken by SAGE, it was essential to:
“understand the objectives behind seeking to manage the epidemiological curve (for example flattening the peak, spreading the duration, avoiding winter) informed by key challenges the NHS is seeking to mitigate. Once there is clarity on those issues, SAGE should review all potential methods to limit spread (schools, travel, large gatherings, home working), including their likely relative effectiveness.”309 |
| 2.123. | NHS England was also given the task of providing SPI-M-O with “a list of precise and essential criteria upon which NHS planning depends”, for example “an estimate of the percentage of patients needing respiratory support, and for how long”, in order for SPI-M-O to model these in different outbreak scenarios.310 The UK government had not, by this point, communicated to SAGE in sufficient detail – if at all – the objectives of its plan for responding to the virus. |
| 2.124. | SAGE again discussed the need for a UK-wide surveillance study, proposals for which were to be drafted by Public Health England in conjunction with the devolved administrations.311 Professor Vallance said that, by this point:
“[I]t had already become apparent to me and to others on SAGE that we were struggling, and would continue to struggle to collect, share, and analyse the data that we needed to inform our response to the pandemic. This was true for NHS data and for community infection data.”312 |
| 2.125. | Nonetheless, no action was taken until April 2020, when a UK-wide surveillance programme led by the Office for National Statistics was introduced.313 That became the Office for National Statistics-led Coronavirus (Covid-19) Infection Survey. |
| 2.126. | On 20 February 2020, for the first time, there was a meeting of the Civil Contingencies Group (Northern Ireland), which brought officials together.314 Dr Naresh Chada, Deputy Chief Medical Officer for Northern Ireland from 2019, advised:
“Departments should consider pandemic influenza planning as a starting point to rapidly advance planning for the reasonable worst case scenario for COVID-19. The elderly and those with existing health conditions will be disproportionately affected. These planning assumptions predict excess deaths, massive impacts across government, school closures, rail and road transport issues, and huge costs.”315 (emphasis in original) There was discussion on, for example, the lack of isolation facilities in Northern Ireland, the need to consider storage facilities in relation to excess deaths, and the need to review business continuity plans in light of reasonable worst-case scenario parameters.316 NICCMA had still not been instituted – an aide-memoire prepared for Mr Pengelly on 21 February repeated that it was not necessary to do so at this time.317 NICCMA was not ultimately activated until mid-March 2020.318 |
| 2.127. | At a NERVTAG meeting on 21 February 2020, it was noted that “the evidence suggests that 40% of virologically confirmed cases are asymptomatic”.319 This was an alarmingly high percentage and suggested that official case numbers in China (and likely internationally) were a significant underestimate of the true spread of the virus. |
| 2.128. | Professor John Edmunds, Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine and a member of NERVTAG from 2014 to 2022, advocated for the risk level to be raised from ‘moderate’ to ‘high’ as there was evidence of ongoing transmission in China, Korea, Japan and Singapore. Unfortunately, NERVTAG did not support this view.320 At the time, Professor Edmunds felt:
“[S]tating that the risk was ‘moderate’ when all indications suggested that we were about to experience a very severe epidemic could be misconstrued and could lead to complacency amongst decision-makers.”321 |
| 2.129. | Also on 21 February 2020, NHS England noted that it needed to raise with the Department of Health and Social Care that its initial modelling suggested:
“[E]ven with continued mitigation work, the NHS would be overwhelmed well before the peak without significant interventions to flatten the curve.”322 |
| 2.130. | Later that day, a situation update noted a cluster of cases in northern Italy, with 7 out of 16 new cases in intensive care. None involved travel to China and the reports indicated that five were healthcare workers. Cases were also reported in Iran, Canada and Lebanon. Fatality and severity indicated that there were substantially more cases. Professor Ferguson told Professor Whitty:
“[T]he epidemiological data – while patchy – suggests that we should be acting on the assumption that sustained transmission is happening now in the UK.”323 Professor Ferguson also called for systematic surveillance to be established, with de-escalation only if that demonstrated sustained transmission was not occurring.324 |
| 2.131. | By 21 February 2020, Professor Ferguson said that he:
“felt it was a matter of when rather than if local community transmission would be discovered in the UK, and thus that the UK should move away from its stated ‘containment’ strategy (i.e. focussing on border measures, which in my view were ineffective) to an evidence-based mitigation strategy (i.e. targeted, layered use of NPIs to reduce transmission). Chris Whitty disagreed regarding the inevitability of local spread and felt it was premature to talk about ending containment. Overall, I felt there was insufficient urgency in government planning at that time, a view shared by John Edmunds and Jeremy Farrar.”325 |
| 2.132. | Professor Ferguson sent a number of emails to Professors Whitty and Vallance and others in government, expressing his concerns and setting out his:
“initial analysis of the potential impact of a variety of non-pharmaceutical interventions (NPIs) on COVID-19 spread.”326 He emphasised the most important conclusion of the analysis, which was: “[A] package combining multiple measures could likely have a major effect. Social distancing which reduces community contacts outside the household and school/workplace might have the single largest impact, if practical and affordable. Akin to the measures in operation in parts of China, Italy and South Korea now.”327 |
| 2.133. | UK passengers from a cruise ship, the Diamond Princess, arrived back in the UK on 22 February 2020, having been quarantined by the Japanese government after a passenger tested positive for Covid-19. Of some 2,600 passengers and 1,000 crew, over 600 people became infected with Covid-19.328 Early reports showed that about 50% of the people infected had no symptoms when they tested positive. Using data from passengers on board, Professor Edmunds and his team initially estimated the overall case fatality ratio and infection fatality ratio to be about 1.1% and 0.5% respectively.329 The infection fatality ratio was estimated to be more than 7% in those over 70 years old.330 These were significant levels of lethality for a virus that could infect up to 80% of the population.331 |
| 2.134. | The Department of Health and Social Care reported 4 more cases in England on 23 February 2020, bringing the total number of cases in the UK to 13.332 |
| 2.135. | That same day, the Italian government imposed a lockdown in 11 municipalities following outbreaks of Covid-19.333 This followed the confirmation of the first two Covid-19 cases on 31 January (as in the UK) and subsequently the first death on 22 February, with a further six deaths by 24 February. It included strict containment measures: prohibition of leaving the area, closure of schools at all levels and suspension of all events, museums and public offices, commercial and work/business activities, with the exception of essential services. This was in response to the threat of hospitals being overwhelmed, with a shortage of beds, ventilators and health professionals. |
| 2.136. | On 24 February 2020, Imran Shafi, Private Secretary to the Prime Minister for public services from March 2018 to March 2021, emailed Professor Vallance, Ms Hammond and senior officials and key advisers to Mr Johnson. He stated:
“At some point soon, I’d like to start exposing the PM to the potential decisions he might have to take in short order on this – at the moment it’s been fairly abstract with him I think.”334 |
| 2.137. | On 24 February 2020, Scottish Government Resilience Room (Officials) met.335 Derek Grieve, Deputy Director to the Health Protection Division, recorded that the Chief Medical Officer gave “everyone both barrels on the impact of COVID19. Felt like a few were starting to appear interested.”336 This was one of many examples of Mr Grieve’s growing frustration at the slow pace of the Scottish Government’s response to the virus during this period. On 26 February 2020, he recorded in his notebook that he had attended a COBR meeting with Ms Freeman and that it was “clear all [departments] in UK Govt are fully engaged [and] mobilised in a way that the [Scottish Government] simply isn’t”.337 On 27 February 2020, he recorded that he had attended a meeting of senior officials within the Scottish Government and there was “still no real engagement. They then spent 20 mins talking about internal SG [Scottish Government] comms. Completely amazed!”338 |
| 2.138. | The concern that departments were not engaged and mobilised also applied to Northern Ireland. The Executive Committee continued to be briefed on the pandemic but had yet to have a substantive discussion about it. At a meeting on 24 February 2020, Mr Swann “briefed the Executive on the COVID 19 (Coronavirus)” under “Any Other Business”.339 Although the substance of this is unclear, a briefing note prepared for Mr Swann in advance of the meeting contained details of the Cabinet Office’s reasonable worst-case scenario planning and advised that the working assumption at the time was:
“[T]he first wave of the pandemic will last approximately 15 weeks with over 50% of the population falling ill and up to 20% off work during the peak weeks.This would lead to a huge surge in demand for health and social care services which would have a knock-on impact on current provision.”340 The note highlighted: “Besides very severe levels of stress on [the health and social care system], the level of excess deaths would stretch capacity within organisations involved in the management of deaths.”341 However, these planning assumptions do not appear to have been shared with the Executive Committee at this time. The speaking note provided to Mr Swann for the meeting made no reference to the reasonable worst-case scenario planning assumptions, nor were they recorded in the handwritten notes of the meeting.342 |
| 2.139. | At the weekly Scottish Cabinet on 25 February 2020, Ms Sturgeon stated that she would chair the Scottish Government Resilience Room meeting later that day, with a fuller discussion at the following week’s Cabinet. A brief discussion of the virus took place under “Any Other Business”.343 |
| 2.140. | At a meeting between Mr Johnson, Mr Hancock, Dominic Raab MP (Secretary of State for Foreign and Commonwealth Affairs and First Secretary of State from July 2019 to September 2021), Professors Vallance and Whitty, and others on 25 February 2020, Mr Cummings stated:
“No10 [10 Downing Street] should see all the plans for what the UK would do in a worst case scenario, including comms plans. The Health Secretary confirmed that there would be a discussion on this with No10 the following day, and that all these plans would be shared.”344 A note highlighting “the most significant choices should a pandemic occur in the UK” was to be shared by 28 February.345 |
| 2.141. | Covid-19 was not included on the formal agenda for the UK government Cabinet meeting on 25 February 2020. Mr Johnson acknowledged that its absence was “a measure of the focus we then had on other things”.346 Notwithstanding this, Covid-19 was raised during the meeting. Mr Hancock reported that case numbers had risen in northern Italy and that Professor Vallance had changed his advice, suggesting:
“[T]hose with symptoms returning from the region North of Pisa should self-isolate for 14 days. Those returning from areas now quarantined should self-isolate regardless of symptoms.”347 |
| 2.142. | The Welsh Government did not discuss Covid-19 in the Welsh Cabinet until 25 February 2020.348 Mr Drakeford told the Inquiry that the signal to start discussing matters in Cabinet was:
“the moment when chief medical officers advised that the risk level to the United Kingdom and to Wales has moved from low to moderate. Right until the point at which the Cabinet begins to discuss things, the advice from our chief medical officers is the risk to Wales is low, and when that is your primary signal it doesn’t read to me like a signal that we need to start mobilising in that purposeful way.”349 As noted above, however, the Chief Medical Officers’ assessment of risk had in fact changed from ‘low’ to ‘moderate’ on 30 January 2020. |
| 2.143. | Work had been ongoing in SAGE with regard to potential interventions. At its meeting on 27 February 2020, SAGE:
“reviewed a table summarising the impacts of non-pharmaceutical interventions – to be finalised at its next meeting”.350 SAGE discussed a report from Imperial College London regarding potential interventions, as well as modelling and examination of a ‘flattening the peak’ strategy. It also endorsed planning assumptions of an overall 1% infection fatality ratio and that 80% of the UK population could become infected.351 This reflected “deaths as a direct result of infection, not those related to NHS overload or other [secondary] effects”.352 A report before SAGE confirmed that, without action, demand on NHS beds would overtake supply before the peak was reached.353 |
| 2.144. | Consequently, SAGE noted two action points in relation to NHS England. Firstly, it should confirm to SPI-M-O “the variables for which it needs numbers in order to model NHS demand”.354 Secondly, UK academic modelling groups and NHS England planners should organise a working group to analyse key clinical variables for reasonable worst-case scenario planning for the NHS, which would then be reviewed by SPI-M-O and discussed at SAGE.355 This working group met on 1 March 2020 (see Chapter 3: The first 12 days of March 2020, in this volume). |
| 2.145. | The delay between Imperial College London making available the first estimate of the infection fatality ratio on 10 February 2020, its accepted use by SAGE at its 27 February 2020 meeting for planning purposes, and its eventual sign-off in early March was described by Professor Ferguson as “understandable given the magnitude of the decisions”, but:
“frustrating for me at the time and clearly regrettable in retrospect. It is difficult for me to establish a clear cause, other than the caution felt by SAGE in accepting estimates with a high level of uncertainty until that uncertainty (slightly) declined. The further delay until broad government acceptance that the RWCS [reasonable worst-case scenario] was a likely rather than just a ‘worst case’ scenario was even more regrettable”.356 |
| 2.146. | At COBR on 26 February 2020, Mr Hancock noted:
“[T]he reasonable worst case planning assumptions looked close to becoming the reasonable planning assumptions … [and] all departments should step up preparations”.357 |
| 2.147. | Internationally, case numbers indicated sustained person-to-person transmission, including in Italy – which received a high number of travellers to and from the UK.358 COBR also discussed the UK’s legislative response. An emergency bill was deemed the appropriate legislative vehicle to address the pandemic.359 However, Mr Drakeford’s impression from this meeting was that the proposed emergency bill would largely mirror the framework of the Civil Contingencies Act 2004, with primary decision-making power remaining with the UK government and implemented by the devolved administrations.360 This was not to be the case. Instead, as discussed in Chapter 13: Legislation and enforcement, in Volume II, public health legislation was used to enforce restrictions in each nation, enabling each government to make its own decisions about the appropriate response in its nation. |
| 2.148. | On 27 February 2020, Mr Johnson stated that he was “keen to really step up activity on Coronavirus”.361 That same day, Northern Ireland identified its first case of Covid-19.362 |
| 2.149. | Following the meeting between Mr Johnson, Mr Hancock and others three days earlier, the Civil Contingencies Secretariat circulated ‘Covid-19: The UK’s preparedness’ on 28 February 2020. This had been drafted in consultation with Mr Hancock and Professors Whitty and Vallance.363 A draft of what would become the Coronavirus: Action Plan, published on 3 March 2020, was also shared.364 |
| 2.150. | The paper acknowledged: “Covid-19 looks increasingly likely to become a global pandemic, although this is not yet certain.”365 It further stated:
“Based on existing assumptions for a severe pandemic flu outbreak, in a reasonable worst case scenario about half of the UK’s population would become ill (many with mild symptoms), and up to 520,000 people could die as a direct result of Covid-19.”366 It went on to explain: “[I]n the reasonable worst case scenario, the risk of Covid-19 to the UK is similar to that of a severe pandemic flu outbreak, although it may well be less severe than this.”367 |
| 2.151. | The paper noted that the UK’s tactical aims were to “contain the infection if possible, delay the peak if not” (emphasis in original).368 It explained that the response would proceed through the phases if the outbreak escalated, and stated:
“The triggers for moving between phases will be provided by the Chief Medical Officers, informed by an assessment of the Scientific Advisory Group for Emergencies (SAGE) and the World Health Organization … we cannot wait until there is sustained transmission in the UK before taking steps to protect the UK. Once the outbreak spreads here we will not have time to both prepare and respond.”369 |
| 2.152. | Mr Johnson believed that the first time he saw the “containment, delay, mitigation” sequence was in this paper (which is considered further in Chapter 3: The first 12 days of March 2020, in this volume).370 He also told the Inquiry that he was “puzzled” after reading the briefing:371
“Which was it? Half a million deaths or a bad flu epidemic? I remember asking my team – and no one seemed to be sure.”372 |
| 2.153. | At a meeting between Mr Johnson, Mr Hancock, Mr Raab, Rishi Sunak MP (Chancellor of the Exchequer from February 2020 to July 2022), Professor Whitty and others to discuss the paper on 28 February 2020, it was concluded:
“We need a major ramp-up of OGD [other government department] activity on domestic preparedness – and we should use the COBR meeting on Monday to land this point with Secretaries of State.”373 However, Mr Shafi’s notes recorded Mr Johnson as saying: “What’s the strategy. – When are we going to take big decisions, of what evidence. – biggest damage done by overreaction.”374 |
| 2.154. | On the same day, Wales confirmed its first positive case of Covid-19 and the World Health Organization raised its alert to ‘very high’ (its highest level of alert).375 |
| 2.155. | Between the end of February and the beginning of March 2020, four cases had been detected through GP surveillance in the UK, one of which was in intensive care.376 None were linked to foreign travel. Professor Ferguson viewed this as:
“the first definitive evidence indicating that community transmission was ongoing in the UK.”377 |
Border controls and restrictions
| 2.156. | By this time, despite the confirmation of cases of infection in the UK, the UK government had no effective border controls in place. Historically, the restriction of movement across borders has been a longstanding practice in the control of communicable diseases. However, in the modern era, the closure or restriction of borders is immensely complex, politically divisive and difficult to put into practice. |
| 2.157. | In order to be effective, border restrictions must be stringent and accompanied by a system of quarantine. There are economic, trade, diplomatic and legal implications, as well as various harmful consequences, including for the importation of food and supplies. This is both particularly relevant and particularly challenging for the UK, which has extensive international travel and trade links. It is also made more complex because the UK comprises England, Scotland and Wales (which have a common outer border) and Northern Ireland (which borders the Republic of Ireland and, therefore, the EU), with borders crossed daily by people who work and live on either side of them. |
| 2.158. | A number of countries introduced port-of-entry measures in response to Covid-19, including border closures, travel restrictions, temperature screening and diagnostic testing (when available). For example, in early January 2020, the Chinese government implemented exit screening for international flights leaving its major airports. Thermal scanning was used to identify passengers with a fever, who could then be tested for Covid-19 before boarding.378 By mid-January, it was reported that a number of other countries and territories – including Hong Kong, Taiwan, Thailand and Singapore – had introduced entry screening at airports of arrivals from China.379 |
| 2.159. | UK decision-makers therefore faced public and political pressure to restrict international travel from affected countries to control the spread, or even the influx, of Covid-19. Mr Johnson said that “the public believed that we had to close the borders and, politically, closing borders was seen as a panacea”.380 |
| 2.160. | The scientific and public health advice, however, was that such measures were ineffective. The focus from January and into February 2020 was on self-isolation for those arriving from China and other affected countries.381 Professor Whitty told the Inquiry that, from a public health perspective:
“unless we closed borders to all nations for a prolonged period we would at best have delayed by a short period the onset of Covid-19”.382 As explained to Mr Johnson in late February, “not everyone with Coronavirus will have a temperature, and not everyone with a temperature will have Coronavirus”.383 |
| 2.161. | Other countries tried, with varying degrees of success, to impose mandatory border restrictions.384 A range of border controls was subsequently utilised in the UK. This included bans on travel from specified countries (such as South Africa in December 2020) and provisions for mandatory quarantine.385 Permitted travel corridors were suspended in January 2021, following the identification of a new Covid-19 variant in Brazil.386 |
| 2.162. | Early in the pandemic, the UK government itself had no detailed plans in place, let alone developed procedures, for imposing stringent border controls such as mandatory quarantine. A more effective system of restrictions or closures would have to have been in place, at the latest by mid-February, to attempt to control the spread of Covid-19 – and would likely have gained the UK only a short breathing period. In May 2020, the UK government and devolved administrations agreed in principle to a joint approach to international travel.387 This underlines the practical and legal impediments during the early months of the Covid-19 pandemic. Having the tools in place (including for a coordinated approach across all four nations), in the event that travel restrictions are required in the future, should be part of the UK’s pandemic preparedness. |
The situation at the end of February 2020
Figure 2: Reported cases in selected European countries in February 2020
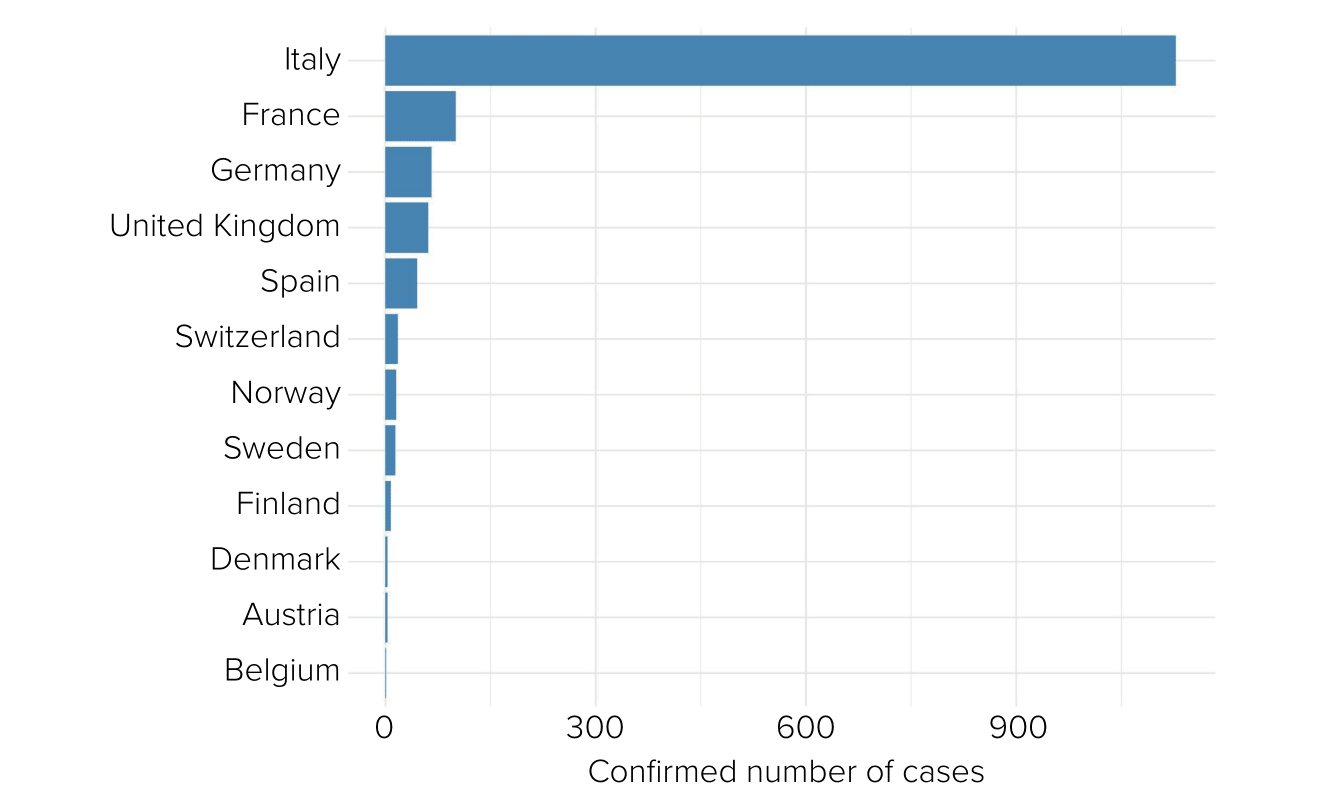
Source: Our World in Data, World Health Organization (https://ourworldindata.org/coronavirus)
| 2.163. | By the end of February 2020, the number of confirmed cases globally had risen to more than 83,000, with more than 4,500 outside China.388 Almost 3,000 deaths had been confirmed globally, of which 73 had occurred outside mainland China.389 The total number of confirmed cases in the UK had increased to 23.390 |
| 2.164. | According to Professor Edmunds:
“[T]he risk for an individual in this country in February was very, very low … So could you take national restrictive measures, would people come along with that? … I think that would be difficult. I think it would be a hard sell … you’re kind of jumping to the nuclear option.”391 The Inquiry considers that the answer lies in adequate planning, ensuring the available options are clearly understood by decision-makers and, when the time comes, preparing the public for the threat on the basis of considered advice. |
| 2.165. | The available data might not have shown many confirmed cases but, given the lack of testing capacity, the potential scale of asymptomatic infection and delays in receiving accurate data, there was a real possibility that the data were masking the real picture. Indeed, genomic analysis published in 2021 showed Covid-19 had been circulating undetected in Scotland one to two weeks before the first detected cases.392 It is now also understood that widespread importation of cases from Spain, Italy and France into the UK had occurred from mid-February 2020.393 As Professor Van-Tam observed in relation to the first two confirmed cases of community transmission in the UK on 28 February 2020, “it was inevitable and … this was just the beginning”.394 |
The adequacy of plans
| 2.166. | The lack of planning for issues concerning border control is unsurprising given that, at the end of February 2020, the plan for the response to Covid-19 was still being developed. Mr Hancock had nevertheless emphasised to the UK Cabinet “time and time again” that the UK was well equipped to respond to Covid-19.395 As considered in the Inquiry’s Module 1 Report, this was likely in part as a consequence of assurances and reassurance he had received that the UK was well prepared – for example, by virtue of the existence of the UK Influenza Pandemic Preparedness Strategy 2011, by the World Health Organization or by the UK’s ranking on the 2019 Global Health Security Index.396 |
| 2.167. | Helen MacNamara, Deputy Cabinet Secretary from January 2019 to February 2021, understood Mr Hancock to mean that he was well versed with the plans. She:
“assumed he’d seen them and been through them and thought they were adequate. I thought that’s what he was saying.”397 |
| 2.168. | Any confidence that there were detailed and carefully considered procedures in place was misplaced. As Mr Cummings explained:
“[I]n the course of February we realised gradually, as we pushed and probed and asked questions for these plans, that they fundamentally didn’t exist.”398 |
| 2.169. | Such departmental plans that existed had not been shared with the Civil Contingencies Secretariat and the Cabinet Office.399 There was no overarching plan beyond the UK Influenza Pandemic Preparedness Strategy 2011.400 The work that was under way was predominantly approached as a health issue, with limited if any planning across other departments. Professor Whitty described the UK Influenza Pandemic Preparedness Strategy 2011 as “woefully deficient” – it did not give him “much that was of any great use”.401 |
| 2.170. | It is likely that Mr Johnson, acting in accordance with his own optimistic disposition, was content to accept the assurances of others, in particular those of Mr Hancock, that all reasonable precautions were being taken. The Inquiry saw no evidence that Mr Johnson challenged the assurances that he was receiving. |
| 2.171. | The response from the devolved governments was also inadequate. |
| 2.172. | There was an absence of any real strategy pursued by the Welsh Government in January and February 2020. Dr Goodall told the Inquiry that, although he did not recall the Welsh Government:
“specifically deciding to formally trigger the Pan Wales Response Plan, this plan did inform and form the basis of much of our action during this initial phase”.402 Dr Sandifer did “not recall being informed that the Pan Wales Response Plan had been activated, if that was the case”.403 Mr Drakeford said there was “no plan to prevent the virus from spreading into Wales” and it was from 25 February that there were “very practical things being discussed about how we would respond to coronavirus when it arrives”.404 |
| 2.173. | In Northern Ireland, there was no cross-government strategy in January and February 2020. This period coincided with the restoration of power-sharing and there was little meaningful, cross-governmental coordination in relation to Covid-19. The Department of Health (Northern Ireland) was leading on the response, and its general approach in these early months is perhaps best encapsulated in Professor McBride’s email to Professor Whitty on 25 January 2020, in which Professor McBride noted:
“As ever you are/will be doing a lot of the heavy lifting for us and providing much appreciated expert advice”.405 |
| 2.174. | In Scotland, Ms Sturgeon said:
“Between January and March, a considerable amount of work was done to ensure that Scotland was as prepared as possible for the situation that was developing.”406 The Scottish Government Resilience Room had been activated. However, in this early period, there appears to have been no real strategy other than monitoring the situation. |
| 2.175. | The devolved administrations failed adequately to conduct their own planning with regard to the implications of Covid-19. Although the Inquiry acknowledges that they were entitled to rely upon advice and assistance from the UK government in combatting an unknown common threat, the devolved administrations became too dependent on the UK government response, which resulted in each devolved administration being significantly underprepared for what was to come. |
Lack of leadership
| 2.176. | Mr Hancock had chaired the first five COBR meetings in January and February 2020, in accordance with guidance that COBR may be chaired by the Prime Minister or any minister (or indeed by a civil servant whose brief is most directly affected). Mr Johnson described Mr Hancock as “the right chair for the job” and neither Mr Johnson nor his advisers suggested that Mr Johnson chair COBR until the end of February.407 |
| 2.177. | Mr Johnson stated that, on 27 February 2020, he asked to chair a full COBR meeting in person.408 Mr Glassborow responded on the same day, agreeing and noting that this would “signal your active involvement on this issue”, although they proposed that Mr Hancock should afterwards resume chairing.409 Mr Hancock said that he contacted Mr Johnson directly on 28 February, telling him that he “had to show that he was engaged on this and that he had to chair a COBR meeting”.410 |
| 2.178. | While it was not wrong for Mr Hancock to chair initial COBR meetings, the fact that it met so regularly, together with the obviously escalating nature of the crisis, made it surprising that COBR was not chaired by the Prime Minister until early March 2020. Alex Thomas, expert witness on political and administrative decision-making, told the Inquiry that, had the Prime Minister chaired an earlier COBR meeting, it would have sent a signal that:
“this required a whole-government response, the Prime Minister was personally engaged in that, and that all departments needed to give their maximum possible attention to this crisis”.411 Mr Johnson should have been advised – and should himself have appreciated earlier – that this was an emergency that required prime ministerial leadership. At the latest, he should have chaired COBR on 18 February 2020. The chairmanship and authorityof the Prime Minister would have conveyed how serious the matter was and would likely have added greater impetus to the UK government’s response. |
| 2.179. | The leaders of the devolved administrations also did not attend all the COBR meetings. |
| 2.180. | The Welsh Government was represented by Mr Gething at the first three COBR meetings.412 Mr Drakeford did not attend until 18 February 2020 because the “meetings focused on health-related issues and that was [Mr Gething’s] portfolio”.413 Sir Frank Atherton reflected more generally that, in Wales, Covid-19 was “managed too long as a health issue rather than as a cross-government issue”.414 |
| 2.181. | Ms Sturgeon did not attend a COBR meeting on behalf of Scotland until 2 March 2020. She stated:
“The attendance of my Health Secretary at the first five COBR meetings was considered appropriate as these meetings were chaired by her counterpart, the UK Health Secretary and attended by relevant Health Ministers of the other devolved governments … In my judgement, this has no impact on the effectiveness of governments’ response to risks and threats.”415 |
| 2.182. | Ms Foster and Ms O’Neill also did not attend COBR until the Prime Minister first chaired it – an assumption having been made that Mr Swann should attend because Mr Hancock, his equivalent, would chair.416 Mr Swann told the Inquiry that the attendance from the outset of the Prime Minister and the First Minister and deputy First Minister of Northern Ireland would have created a stronger sense of cohesion.417 Given the obviously escalating nature of the crisis, in addition to the Prime Minister, all the First Ministers (including the deputy First Minister of Northern Ireland) should also have attended COBR by the middle of February 2020 – only Mr Drakeford did. The attendance of the senior leadership of all four nations would have signified the importance of dealing with the crisis and facilitated lines of discussion. It could potentially have prompted an earlier recognition of the need for a robust cross-government response, in particular for Northern Ireland, which might then have activated NICCMA earlier. |
Lack of urgency
| 2.183. | The highest levels of the UK government failed to respond with sufficient urgency in early and mid-February 2020. As the chronology above demonstrates, there was an element of drift and a failure to take control of the emerging crisis. There were, for example, no COBR meetings between 6 and 17 February (during the school half-term holidays) and Covid-19 was not officially on the agenda for the Cabinet meeting of 25 February. According to Mr Cain, this lack of political engagement reflected “the perceived importance of Covid-19 from those inside Downing Street”.418 |
| 2.184. | Mr Glassborow recalled that it was “business as usual” in 10 Downing Street until late February 2020.419 Ms MacNamara became “increasingly concerned about the confidence of the tone of any discussion about the virus”.420 She described the atmosphere of the Prime Minister’s morning meetings as “confident and macho”.421 Professor Edmunds agreed that the UK government:
“did not really take the pandemic very seriously until March, by which time it was very late. Much of the lead time had been wasted.”422 |
| 2.185. | Mr Johnson suggested that, in January 2020, there was “no loud klaxon of scientific alarm, certainly not in the heart of government”, and that even by the middle of February 2020 this was still not being communicated.423 However, Mr Hancock, as well as Professors Whitty and Vallance, had sought to impress upon Mr Johnson the gravity of the situation; Mr Johnson’s advisers had received briefings to similar effect; and Professor Whitty had advised that the country was looking realistically at two scenarios, one of which had the potential to spiral rapidly in weeks into a pandemic. The threat level to the UK population had been raised to ‘medium’, NHS England had already declared the highest level of emergency and the first cases of Covid-19 had been detected in England. There was evidence of sustained transmission in China and Italy and credible estimates of the case and infection fatality ratios, along with the potential for 80% of the population to be infected. This, accompanied by the experience of lockdown in Italy, should have prompted a far higher level of concern and action. |
| 2.186. | Nonetheless, Mr Johnson maintained that the scientific community had not made the risks clear.424 He said: “I am afraid at that stage there were just too many things we did not understand or underestimated.” However, he accepted that:
“It is clear that we were far too complacent about what might happen, and about the state of our national preparedness. It was not the case that I was somehow distracted by other things.”425 |
| 2.187. | Mr Johnson’s failure to appreciate the nature of the impending crisis was, in part, because of his optimism that it would amount to nothing, his scepticism arising from earlier UK experiences of infectious diseases and, inevitably, his attention being on other government priorities – with Covid-19 not even being in the top five issues crossing his desk in early to mid-February 2020. This was most likely exacerbated by the assurances he was receiving that plans were in place. |
| 2.188. | That said, even as late as 28 February 2020, Mr Johnson was being advised by the Civil Contingencies Secretariat that “Covid-19 looks increasingly likely to become a global pandemic, although this is not yet certain.”426 The focus on certainty was reflected in and compounded by the nature of the scientific advice. Professor Edmunds stated that SAGE’s advice “attempted to be neutral”.427 It did not generally recommend interventions but advised on efficacy. For example, on 27 February 2020, SAGE noted that modelling suggested “earlier and or combined interventions will have more significant impact”.428 As Professor Edmunds remarked, this “implies that a package of interventions should be introduced quickly but falls short of actually recommending it”.429 SAGE’s advice was also tempered by an anticipation that “certain measures would be unpalatable or difficult to implement”.430 Professor Edmunds observed:
“The neutral (scientific) tone of the advice from SAGE met with this optimistic outlook, may well have led to significant delays to effective action taking place.”431 In the view of Professor Dame Angela McLean (Chief Scientific Adviser to the Ministry of Defence from 2019 to 2023 and Government Chief Scientific Adviser from April 2023), “advisers should err on the side of giving unequivocal advice earlier in the context of advising on time-sensitive matters”.432 |
| 2.189. | The Inquiry acknowledges the expertise and skill of SAGE. Its advice was – and must remain – evidence-based, measured and objective, providing “a unified, rounded statement of scientific advice” as described by Dame Deirdre Hine in her July 2010 review of the UK response to the swine flu pandemic.433 However, the advice given to the UK government by SAGE, although making clear the available information and the risks posed by the virus, failed to reflect the need for immediate action. In part, this could have been due to the constraints on SAGE’s own functions – SAGE did not regard itself as empowered to recommend specific actions.434 |
| 2.190. | This resulted in a disconnect between the way in which SAGE’s advice was imparted and the way in which it was received. With regard to the latter, this might have been because, as Professor Whitty stated, the system underplayed “relative to other threats … natural threats, including health threats” – with these not being understood to be as tangible or ‘real’ as, for example, threats to national security.435 Nevertheless, the overarching system under which ministers received technical and scientific advice – and acted accordingly in light of all the available information – failed to lead to sufficiently speedy and robust action being taken to respond to the virus. This had extremely serious consequences. |
| 2.191. | Similarly, the communication of risk might also have contributed to a false sense of security and affected some decision-makers, who suffered from what Professor Woolhouse described as “optimism bias”.436 |
| 2.192. | Risk levels rose from ‘very low’ at the outset of the pandemic in January through to ‘moderate’ in February 2020. Professor Van-Tam told the Inquiry:
“[W]here the risk assessment system has failed us … is that it relates to the current moment and that, unfortunately, when you then try to say, ‘Oh, what does it mean for the future?’ you get into massive uncertainty … I think it’s very unfortunate that this can be read as ‘Oh, well, it’s low, just forget about it’.”437 |
| 2.193. | The nature of the reasonable worst-case scenario also remained elusive for those who were not experts and resulted in a similar discounting of risk. In the Cabinet Office, it was not understood that the reasonable worst-case scenario was a scenario that was to be planned for, rather than a possible projection. Lord Sedwill told the Inquiry:
“I think we wouldn’t have understood that to be inevitable … this was a discussion of the reasonable worst-case scenario and in late January, early February, I think Cabinet, for example, the Chief Medical Officer, gave that around a 1 in 10 probability, and by the end of February I think it was about 1 in 5.”438 He also noted: “[T]he scientific advice is essentially suggesting that the worst-case scenario is unlikely, is indeed very unlikely, and so that undoubtedly will have informed the way ministers were thinking about this.”439 |
| 2.194. | The low statistical likelihood appears to have given false reassurance. Mr Johnson said that, by mid-February 2020, the UK government was “not yet believing that the [reasonable worst-case scenario] or anything like it [was] going to happen”.440 Sir Simon Stevens, Lord Stevens of Birmingham, Chief Executive of NHS England from April 2014 to July 2021, told the Inquiry:
“There was too much ambiguity about what the status of this reasonable worst-case scenario was during the course of February and the first part of March and the probability that the reasonable worst case was actually going to become the case … there needs to be much greater clarity about what is the probability that is being assigned to these different potentials, so that policymakers can understand what exactly they’re being told.”441 |
| 2.195. | Professor Whitty acknowledged that the reasonable worst-case scenario is a “slippery concept”.442 It was insufficiently clear. As he explained, efforts to communicate its meaning to “people who are not used to it” can cause considerable confusion, because “they will say: well, how likely is that? To which the answer is: extraordinarily unlikely, and then everyone relaxes.”443 It led to differing understandings of what was actually meant and contributed to governments failing to act with sufficient urgency. The emphasis on the ‘worst-case’ scenario was an unhelpful distraction. As set out in Recommendation 3 of the Inquiry’s Module 1 Report, there must be a better approach to risk assessment, including the communication of risk. |
| 2.196. | The lack of understanding of the risks posed, the neutral tone adopted and the focus on certainty in a situation beset with uncertainties and imperfect data are likely to have contributed to the UK government’s – and in particular Mr Johnson’s – failure to appreciate the urgency of the situation. |
| 2.197. | In Scotland, throughout February 2020, Professor Woolhouse continued to contact Dr Calderwood to offer assistance and advice, including meeting with her and providing briefing papers regarding developments.444 Professor Sir Gregor Smith (interim Chief Medical Officer for Scotland from April to December 2020 and Chief Medical Officer for Scotland from December 2020) told the Inquiry that the advice Professor Woolhouse was giving was “straight out of the health protection playbook”.445 Professor Woolhouse’s impression was that Dr Calderwood had not engaged adequately with his concerns.446 Although Dr Calderwood shared Professor Woolhouse’s concerns with the Chief Medical Officers for England, Wales and Northern Ireland – and eventually met Professor Woolhouse – Dr Calderwood did not herself advise the Scottish Government to implement the type of actions that Professor Woolhouse was recommending. Although steps were being taken to ensure that health boards across Scotland were making immediate preparations, Covid-19 received insufficient or no attention in Scottish Cabinet meetings. The Scottish Government’s approach during this period was broadly one of monitoring the situation and resting on the existing plans for an influenza pandemic.447 |
| 2.198. | Mr Drakeford, Mr Gething and the Welsh Government also failed to sufficiently engage with the risk until late February 2020. Although a Technical Advisory Cell was established (which evolved later into a coordination function and an expert advisory group), the risk was not discussed at Cabinet before 25 February and Public Health Wales was not adequately consulted at a ministerial level.448 Given the warning sounded by Dr Atherton on 24 January 2020 and the clear signs of the virus’s growing threat, this was too late. Discussing Covid-19 at a Welsh Cabinet level might have led to a quicker cross-government response, and Mr Drakeford, as First Minister, should have brought Covid-19 to official meetings of the Cabinet prior to the final week of February. |
| 2.199. | Both Mr Drakeford and Mr Gething relied significantly upon the UK government and on UK-wide risk assessments, without adequately considering the specific circumstances in Wales. Mr Drakeford told the Inquiry that his belief throughout the period from 1 January “right up until 20 March” 2020 was predicated on the basis that:449
“the essential decisions would remain in the hands of the UK Government and that devolved governments would be implementers of those decisions”.450 He said that the virus had no direct impact in Wales in January and February 2020 and that “as we entered March 2020, Covid-19 and its seriousness became more apparent”.451 |
| 2.200. | Mr Drakeford’s belief that “the response to Covid-19 would be a UK response and the decisions would be taken by the UK Government” is not surprising.452 The central structures of the UK government, including COBR and SAGE, could only be activated by the UK government and were better equipped to respond to an emergency that would potentially impact the entirety of the UK. However, this did not mean that the Welsh Government should not have recognised the severity of the situation in January and February 2020 and taken its own steps to prepare for the arrival of Covid-19 in Wales. Mr Gething and Mr Drakeford were aware of the growing risks from Covid-19. Mr Gething attended the first three meetings of COBR and the outcome of those meetings was reported back to Mr Drakeford. Mr Drakeford chose to attend the next meeting of COBR because “the situation escalated”.453 |
| 2.201. | The ability of the Northern Ireland Executive to respond to the emerging virus was undoubtedly and obviously impacted significantly by the prolonged period without a functioning government. As Sir David Sterling suggested, the absence of political direction in Northern Ireland between 2017 and 2020 had left public services in a state of “decay and stagnation”.454 The depletion in the capacity of the Civil Contingencies Policy Branch – which was responsible for the regular review of plans prepared by individual departments and public authorities – was part of that stagnation. It had “a critical staff resources, experience and skills deficit” and was impacted by “EU exit preparations”.455 Its lack of capacity was not remedied prior to the end of February 2020. As accepted by Mr Stewart, the Northern Ireland Executive “ought not to have been 18 months behind in our planning for an influenza pandemic”.456 |
| 2.202. | Despite the gravity of the situation, by the end of February 2020 only one meeting of the Civil Contingencies Group (Northern Ireland) had taken place and the need for any central civil contingency arrangements was yet to be declared. This was, plainly, inadequate. A number of senior officials suggested that this was because they were not needed at this stage or that their instigation would have required too many officials being taken from other departments.457 The reality is that neither ministers nor officials comprehended the risk that Covid-19 posed to Northern Ireland. There was little or no concept that responding to a prospective pandemic would require cross-government planning, encompassing every government department. |
| 2.203. | In part, this absence of cross-government response from January until the end of February 2020 reflected the fact that Northern Ireland government departments operate with a significant degree of autonomy and operational independence. This, compounded by its role as lead government department, meant that the Department of Health (Northern Ireland) had very substantial control over the initial response to the pandemic in Northern Ireland and that there was very little meaningful oversight or interrogation as to what its preparations for the pandemic were. On the other hand, the fact that the Department of Health (Northern Ireland) was the lead government department gave licence to other ministers to view the pandemic as a health crisis that required a health response. As such, this failure is not that of the Department of Health (Northern Ireland) alone. The risks of Covid-19 to Northern Ireland ought to have been apparent to all ministers. Ms Foster and Ms O’Neill, as well as the Northern Ireland Executive Committee, ought to have led a robust, coordinated response to the situation that was developing throughout February. They should have interrogated advisers as to what arrangements were being made (eg for testing) as the pandemic gathered momentum. While it is recognised that the Executive Committee had just recently been re-established and was therefore in the process of agreeing a Programme for Government and establishing working relationships, the Executive Committee ought to have considered, at the earliest point, how it was going to discharge its responsibilities to the people of Northern Ireland in light of these risks and how it was going to oversee the cross-government preparations (including those of the Department of Health (Northern Ireland)) and response to the pandemic. |
Lost time
| 2.204. | The Inquiry accepts that when the novel coronavirus first emerged in 2020, there was good reason to maintain a ‘watching brief’. There were dangers to overreacting as well as to under-reacting. |
| 2.205. | However, the Inquiry does not accept that the UK government and devolved administrations can rely on a lack of certainty about the characteristics of the new virus to justify their failure to take effective action from mid-February 2020. By that time, it was known that the virus was spreading around the world and had reached Europe and the UK. There was likely sustained community transmission in the UK. Yet it was clear that the test and trace system was inadequate for a pandemic. There was a lack of adequate diagnostic capacity and an inability to scale up manufacturing and laboratory capacity.458 This meant that by 27 February, only approximately 2,100 tests were being undertaken per day.459 In Northern Ireland, as at 10 February, it stood at 40 tests a day.460 By the middle of February:
“Wales had the capacity to carry out 100 tests a day … it clearly was not going to be sufficient to meet a mass testing regime.”461 In Scotland, only 350 tests could be carried out each day.462 Moreover, the known extent of asymptomatic infection and potential for significant asymptomatic transmission meant that the verified cases could only be the ‘tip of the iceberg’ of undetected infections. |
| 2.206. | The four governments knew enough to spur them into action. Accordingly, the Inquiry finds that the lack of urgency (particularly during the mid-February school half-term holidays) and the failure of the four governments to take a grip of the situation and make adequate preparations are inexplicable. They failed to anticipate the scale and speed of the oncoming pandemic and to act accordingly. |
| 2.207. | As the Independent Panel for Pandemic Preparedness and Response (established by the World Health Organization) reported in May 2021, February 2020 was “a lost month”.463 This was certainly the case in the UK. |
- Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, p55, para 10 (https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642)
- INQ000151286_0002
- INQ000151286_0001
- INQ000151286_0001; INQ000151289_0001; INQ000151291_0001
- INQ000238826_0024 para 63
- INQ000047484_0001
- INQ000047484_0001
- INQ000251645_0071 para 7.10
- INQ000251645_0071 para 7.12
- INQ000151293_0001
- INQ000147248
- INQ000235212_0024-0025 paras 81-82; INQ000147237; INQ000188992_0001; INQ000147248; INQ000425573
- INQ000251906_0149 paras 656-667. The protocol was published later in January 2020 (INQ000061497) with analyses being reported in daily Situation Reports (SitReps) from 13 February; see for example INQ000223365.
- INQ000119453_0003. This was endorsed by NERVTAG on 13 January 2020 (INQ000023107_0006).
- INQ000251645_0075 para 7.33
- INQ000251645_0075 para 7.33
- INQ000151296_0002
- INQ000233737_0001; see also INQ000232194_0024-0025 paras 92-97
- INQ000232194_0025 para 98; INQ000255836_0010 para 20
- INQ000255836_0010 para 20. Zoonotic diseases are those caused by pathogens that originated from animals other than humans.
- Boris Johnson 6 December 2023 51/1-7
- ‘WHO statement regarding cluster of pneumonia cases in Wuhan, China’, World Health Organization, 9 January 2020, p1 (https://www.who.int/hongkongchina/news/detail/09-01-2020-who-statement-regarding-cluster-of-pneumonia-cases-in-wuhan-china;
INQ000236523); see also INQ000183385 - INQ000023107_0005 para 3.7
- INQ000360968_0006 para 2.6; INQ000339576_0010 para 1.4.4
- NERVTAG is an expert committee with a specific focus on novel respiratory illnesses and its members have a variety of expertise, including clinical, epidemiology, virology and behavioural sciences (INQ000248853_0053 para 5.164).
- INQ000023107_0003 para 3.2. It also stated that “[w]ith the evidence that is currently available, the novel virus does not look to be very transmissible” (INQ000023107_0003 para 3.3).
- INQ000269203_0032-0033 para 6.18
- INQ000047493_0002; see also INQ000269203_0034-0035 para 6.22
- INQ000236435
- INQ000151316_0002-0003
- INQ000047501_0001
- INQ000047501_0001
- INQ000151324_0002; INQ000183386_0002
- INQ000183386_0002; INQ000151324_0002
- INQ000269203_0076 para 6.109
- INQ000269203_0042 para 6.34; see also Jonathan Van-Tam 22 November 2023 178/8-10
- INQ000474401_0015 para 5.1
- INQ000119453
- INQ000106057_0002
- INQ000291499_0002-0003
- INQ000339033_0061 para 158
- INQ000047509_0002
- INQ000047509_0002
- INQ000047509_0002
- INQ000269203_0041 para 6.32
- INQ000269203_0042 para 6.36
- INQ000106057_0001
- INQ000280628_0035 para 69
- INQ000251645_0072 para 7.17
- INQ000232194_0005 para 16
- INQ000250229_0021 para 78; INQ000182321_0002
- INQ000023119_0003 para 2.5
- INQ000023119_0003 para 2.5
- INQ000262076_0003
- Andrew Goodall 5 March 2024 47/5-13
- INQ000103352_0005-0006. Dr Calderwood did not give evidence on these issues due to having been excused on medical grounds.
- INQ000103352_0005
- INQ000103352_0006
- INQ000103352_0006
- INQ000103352_0005-0006
- INQ000047510; see also Chapter 9: Scientific and technical advice, in Volume II
- INQ000061509_0003 paras 7-13
- INQ000061509_0003 para 8
- INQ000074895_0002 para 15
- Report 2: Estimating the Potential Total Number of Novel Coronavirus (2019-nCoV) Cases in Wuhan City, China, Imperial College London, 22 January 2020, pp2-4 (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/disease-areas/covid-19/report-2-update-case-estimates-covid-19; INQ000236275
- INQ000223314_0003;
‘DHSC and PHE statement on coronavirus’, Department of Health and Social Care and Public Health England, 22
January 2020 (https://www.gov.uk/government/news/dhsc-and-phe-statement-on-coronavirus; INQ000051719_0002) - INQ000056148_0006
- INQ000061509_0004 para 23
- Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 5 (https://covid19.public-inquiry.uk/documents/module-1-full-report); see also INQ000238826_0031-0032, 0047 paras 89-90, 140
- See Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 5
(https://covid19.public-inquiry.uk/documents/module-1-full-report) - INQ000232194_0029 para 117
- INQ000232194_0029 para 117
- INQ000106057_0002; INQ000023107_0008 para 5.8; INQ000051708_0005
- INQ000023107_0007-0008 para 5.6
- INQ000023119_0005 paras 4.4, 4.9; see also INQ000061509_0003-0004 paras 18-20, 25
- INQ000232194_0027, 0029 paras 105, 117
- INQ000103626_0002 para 5
- INQ000267867_0006, 0014 paras 26, 56; INQ000107119_0016 para 3.1
- INQ000390618_0032 para 92; INQ000309705
- INQ000092712_0001-0002 para 3
- INQ000183632_0001 para 1
- INQ000411550 0033 para 83
- INQ000573860_0001
- INQ000147265_0001
- INQ000232194_0030 para 122
- INQ000279874_0002
- INQ000398416_0001
- Michael McBride 10 May 2024 55/20-56/16; INQ000398416_0001
- Michael McBride 10 May 2024 55/20-56/16
- INQ000398416_0001
- INQ000048313_0005
- See UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 3 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, p27, para 3.13 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000056214; see also INQ000279876
- INQ000092893_0014 para 2.28; INQ000273841_0024-0025 para 43
- INQ000056214_0004 para 2
- INQ000056214_0005 para 9
- INQ000056214_0004 para 4
- INQ000279876_0001
- INQ000237557_0002
- INQ000391115_0011 para 41
- INQ000421704_0106 para 229
- INQ000339033_0055 para 147
- INQ000339033_0056 para 149(b)
- INQ000292534_0001
- INQ000371209_0023-0024 paras 72, 74; Mark Drakeford 13 March 2024 52/16-54/21
- INQ000227810_0001
- ‘A novel coronavirus outbreak of global health concern’, C. Wang, P.W. Horby, F.G. Hayden, G.F. Gao, The Lancet (2020), 395(10223), 470-473 (https://doi.org/10.1016/S0140-6736(20)30185-9; INQ000222003_0003)
- ‘Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China’, C. Huang, Y. Wang, X. Li, L. Ren, J. Zhao, Y. Hu, et al., The Lancet (2020), 395(10223), 497-506 (https://www.doi.org/10.1016/S0140-6736(20)30183-5; INQ000408060_0001)
- ‘A novel coronavirus outbreak of global health concern’, C. Wang, P.W. Horby, F.G. Hayden, G.F. Gao, The Lancet (2020), 395(10223), 470-473 (https://doi.org/10.1016/S0140-6736(20)30185-9; INQ000222003_0003-0005)
- Report 3: Transmissibility of 2019-nCoV, Imperial College London, 25 January 2020, p1 (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/disease-areas/covid-19/report-3-transmissibility-of-covid-19; INQ000236276).
This was published on 25 January 2020 but shared with the UK government and the World Health Organization two days earlier (INQ000249526_0039
para 122). - INQ000249526_0039 para 122; Report 3: Transmissibility of 2019-nCoV, Imperial College London, 25 January 2020, p1 (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/disease-areas/covid-19/report-3-transmissibility-of-covid-19; INQ000236276)
- INQ000103233_0002
- INQ000103233_0001
- INQ000103352_0004
- INQ000103352_0004
- INQ000047559_0002
- Michael McBride 10 May 2024 54/1-8, 61/19
- INQ000103352_0003
- INQ000103352_0001-0002
- INQ000267867_0007-0008 para 31
- INQ000235212_0055-0056 para 181; Quentin Sandifer 6 March 2024 6/4-23
- ‘Wuhan coronavirus: Health Secretary’s statement to Parliament’, Department of Health and Social Care and Matt Hancock, 27 January 2020 (https://www.gov.uk/government/speeches/wuhan-coronavirus-health-secretarys-statement-to-parliament; INQ000237587_0002)
- ‘Statement from the Chief Medical Officer for Wales about Coronavirus (2019-nCoV)’, Welsh Government, 31 January 2020 (https://www.gov.wales/statement-chief-medical-officer-wales-about-coronavirus-2019-ncov; INQ000048722)
- INQ000068530_0001; INQ000068531_0001; INQ000087249_0001; INQ000068537_0001
- INQ000300280_0020 para 2.4
- INQ000411550_0015, 0033 paras 29, 82
- INQ000146557_0001-0002
- INQ000146557_0001
- INQ000146557_0001
- INQ000146557_0002
- INQ000146557_0001-0002
- INQ000146557_0002 para 3
- INQ000146557_0001
- INQ000146557_0001 para 1
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000061510_0003 paras 10-12, 16; see also Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 1 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000061510_0004
- INQ000147775_0004 footnote 3; INQ000147768_0009; INQ000147770_0005
- INQ000061510_0004 para 27
- INQ000269203_0074 para 6.105
- INQ000061510_0004 para 28
- INQ000061510_0003 para 20
- INQ000061510_0003 para 8
- INQ000051925_0003 para 26
- INQ000238707_0005 para 17; INQ000273956_0029 para 136
- INQ000257364; INQ000339033_0061 para 160
- INQ000047820_0008 para 4.1
- INQ000282744_0002
- INQ000282744_0002-0003 (Professor Whitty was listed as “the owner of the cell phone”)
- INQ000233747_0002
- INQ000232194_0036 para 147; see also INQ000251645_0077-0078 para 7.43; Chapter 1: The context for pandemic decision-making, in this volume Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 4 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000251645_0077-0078 para 7.43
- INQ000056226_0005 para 3
- INQ000056226_0005 para 4
- ‘Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia’, Q. Li, X. Guan, P. Wu, X. Wang, L. Zhou, Y. Tong, et al., The New England Journal of Medicine (2020), 382(13), 1199-1207 (https://doi.org/10.1056/NEJMoa2001316; INQ000308705_0002)
- ‘Early transmission dynamics in Wuhan, China, of novel coronavirus-infected pneumonia’, Q. Li, X. Guan, P. Wu, X. Wang, L. Zhou, Y. Tong, et al., The New England Journal of Medicine (2020), 382(13), 1199-1207 (https://doi.org/10.1056/NEJMoa2001316; INQ000308705_0002)
- INQ000238826_0028-0029 para 80
- ‘Statement from the 4 UK Chief Medical Officers on novel coronavirus’, Department of Health and Social Care, 30 January 2020 (https://www.gov.uk/government/news/statement-from-the-four-uk-chief-medical-officers-on-novel-coronavirus; INQ000203938_0002)
- INQ000269892; INQ000269973; INQ000087445; INQ000116811_0005 para 11
- INQ000116811_0031 para 110
- INQ000144792_0066 para 204
- INQ000391226_0003; Michelle O’Neill 14 May 2024 146/13-147/25
- INQ000391226_0003; Michelle O’Neill 14 May 2024 146/13-147/25
- INQ000056142_0009
- INQ000056125_0011
- INQ000056125; INQ000232194_0038 para 159
- INQ000223324_0018
- INQ000237635_0002
- ‘CMO confirms cases of coronavirus in England’, Department of Health and Social Care, 31 January 2020 (https://www.gov.uk/government/news/cmo-confirms-cases-of-coronavirus-in-england; INQ000056166_0002)
- INQ000061510_0003 para 8
- INQ000251645_0231 para 16.26
- INQ000057492_0002 para 16; INQ000047820_0002-0004 paras 2.4-2.13
- INQ000255836_0011 para 30
- INQ000056125_0011
- INQ000255836_0194 para 667
- INQ000232194_0009-0010 para 37
- INQ000232194_0010 paras 37, 39
- INQ000273833_0008 para 32
- INQ000339033_0056 para 149
- INQ000339033_0056 para 150
- Michael McBride 10 May 2024 69/9-10
- Michael McBride 10 May 2024 70/17-71/1
- INQ000371209_0027 para 83
- Robin Swann 13 May 2024 179/20-21
- INQ000233747_0002; INQ000282744
- INQ000106067_0001
- INQ000233747_0002
- INQ000282744_0002-0003
- INQ000232194_0034-0035 para 142
- INQ000232194_0027 para 107
- Matt Hancock 30 November 2023 86/22-87/13
- INQ000255836_0010 para 22
- INQ000302484_0018 para 64
- INQ000252711_0004 paras 16, 18
- INQ000273956_0029 para 136; INQ000238707_0004-0005
- INQ000129852; INQ000371209_0025 para 77; INQ000255838_0005 para 17
- Mark Drakeford 13 March 2024 46/19-24
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan, World Health Organization, 4 February 2020, p6 (https://www.who.int/publications/i/item/strategic-preparedness-and-response-plan-for-the-new-coronavirus; INQ000087457)
- INQ000047653_0001
- INQ000051883_0002 para 13; INQ000051925_0003 para 27
- ‘Coronavirus public information campaign launched across the UK’, Department of Health and Social Care, 2 February 2020 (https://www.gov.uk/government/news/coronavirus-public-information-campaign-launched-across-the-uk; INQ000237306)
- INQ000212206_0001
- INQ000051882_0001
- INQ000061511_0003 para 3
- INQ000056215_0005 para 6
- INQ000119615_0009 paras 3.40-3.42
- INQ000119615_0008-0009 paras 3.29, 3.37
- INQ000051925_0004 para 40
- INQ000051925_0004 paras 40-42
- INQ000061512_0003 para 5
- INQ000052045_0003 para 8; INQ000061519_0004 paras 14-15
- 2019 Novel Coronavirus (2019-nCoV): Strategic Preparedness and Response Plan, World Health Organization, 4 February 2020, p8 (https://www.who.int/publications/i/item/strategic-preparedness-and-response-plan-for-the-new-coronavirus; INQ000087457)
- INQ000251645_0080 para 7.52
- INQ000251645_0011 para 2.10
- INQ000280628_0040 para 80
- INQ000280628_0040 para 80
- INQ000251645_0080-0081 para 7.53
- Boris Johnson 6 December 2023 71/16-18
- INQ000255836_0020 para 80
- INQ000255836_0010 para 22
- Boris Johnson 6 December 2023 45/24-46/3
- INQ000238704_0004 para 19
- INQ000348708_0004
- Mark Woolhouse 24 January 2024 30/24-25; INQ000352401
- INQ000103215_0004
- INQ000103352_0004-0005;
INQ000352401_0001-0002 - Reg Kilpatrick 6 March 2024 153/11-154/19; INQ000321239
- Reg Kilpatrick 6 March 2024 151/12-22
- INQ000321228_0003; INQ000129852_0006 para 5.4
- INQ000267867_0036 para 148
- Reg Kilpatrick 6 March 2024 158/21-159/1
- INQ000187578_0019; Reg Kilpatrick 6 March 2024 158/15-159/1
- INQ000048442_0004; INQ000048441_0002; Robin Swann 13 May 2024 104/24-105/13
- INQ000449440_0037 para 115
- INQ000056148_0006
- INQ000056215
- INQ000056215_0005 para 2; INQ000056148
- INQ000056215_0005 para 5
- INQ000056215_0008 para 9
- The Health Protection (Coronavirus) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/129/contents); Public Health (Control of Disease) Act 1984 (https://www.legislation.gov.uk/ukpga/1984/22/contents)
- The Health Protection (Coronavirus) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/129/contents). As discussed in Chapter 13: Legislation and enforcement, in Volume II, these regulations were subsequently revoked by the Coronavirus Act 2020, which largely replicated their provisions.
- INQ000061513_0003 para 5
- INQ000061513_0002 paras 2-3
- INQ000236371_0037
- INQ000056137_0007
- INQ000056137_0006
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000218470_0002
- INQ000092739_0006-0007 para 13
- INQ000254430_0003 paras 20-21
- INQ000185378_0003
- INQ000469468; INQ000212916_0002 para 6
- ‘PHE novel coronavirus diagnostic test rolled out across UK’, Public Health England, 7 February 2020 (https://www.gov.uk/government/news/phe-novel-coronavirus-diagnostic-test-rolled-out-across-uk; INQ000582848)
- INQ000087249_0001
- INQ000048723; INQ000357279; INQ000254430
- Report 4: Severity of 2019-Novel Coronavirus (nCoV), Imperial College London, 10 February 2020, p1 (https://www.imperial.ac.uk/media/imperial-college/medicine/sph/ide/gida-fellowships/Imperial-College-COVID19-severity-10-02-2020.pdf; INQ000236277)
- INQ000207453_0001
- INQ000237386_0001-0002 para 7
- INQ000238826_0039 para 113
- INQ000238826_0039 para 114
- Boris Johnson 6 December 2023 70/2-71/23
- Lee Cain 31 October 2023 11/16-21
- INQ000302484_0018-0019 para 65
- INQ000106107; Matt Hancock 30 November 2023 111/17-18; UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000075784_0002 para 5
- INQ000237386_0001-0002 paras 1, 13
- INQ000075784_0004 para 33
- INQ000238826_0041 para 117; INQ000320718
- INQ000249526_0039 para 123; INQ000320718
- INQ000320721_0001
- INQ000232194_0044-0045 para 187
- INQ000052022; INQ000273915
- Jeane Freeman 29 January 2024 168/5-9, 167/23
- INQ000269182_0012 para 38; see also Robin Swann 13 May 2024 91/6-17; Vaughan Gething 11 March 2024 61/4-62/11
- INQ000052022; UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- Robin Swann 13 May 2024 90/19-91/17
- Vaughan Gething 11 March 2024 61/4-62/11
- INQ000232194_0044-0045 para 187. The same was true of Scotland (INQ000320642_0002 paras 7-8).
- INQ000106109_0002 para 5
- INQ000056138_0006
- INQ000056138_0006; INQ000248853_0039 para 5.125
- INQ000056138_0008; INQ000106109_0002 para 1
- INQ000255836_0083-0084 para 315
- INQ000056138_0007
- INQ000056138_0007
- INQ000144792_0066 para 204. (The Inquiry is considering procurement of healthcare-related supplies in Module 5: Procurement.)
- INQ000087520
- Boris Johnson 6 December 2023 81/20-82/13
- Martin Reynolds 30 October 2023 71/18-72/2; INQ000273872_0030 para 149; INQ000226185_0038-0042
- Dominic Cummings 31 October 2023 167/22-24
- INQ000310090_0002 para 16
- INQ000233531
- INQ000238703_0004 para 16
- INQ000362666_0003
- INQ000238703
- INQ000052098_0002-0003 para 7
- Yvonne Doyle 2 November 2023 200/2-202/22; INQ000273878_0010 para 28
- INQ000273878_0009-0010 paras 26-27
- ‘Feasibility of controlling COVID-19 outbreaks by isolation of cases and contacts’, J. Hellewell, S. Abbott, A. Gimma, N.I. Bosse, C.I. Jarvis, T.W. Russell, et al., The Lancet Global Health (2020), 8(4), E488-E496 (https://doi.org/10.1016/S2214-109X(20)30074-7; INQ000092645_0001)
- INQ000056227_0005 para 2
- INQ000049396_0001
- Mark Drakeford 13 March 2024 33/19-21
- INQ000339033_0196 para 615
- INQ000056227_0007 para 17
- INQ000061517_0004 para 11
- INQ000061517_0003 paras 8-9
- INQ000061517_0003
- INQ000061517; INQ000238826_0047 paras 139-140
- INQ000238826_0047 paras 139-140
- INQ000238826_0018 para 45b
- INQ000023220
- INQ000425536_0016
- INQ000023220
- INQ000425535
- David Sterling 1 May 2024 180/15-20
- INQ000119469_0006 para 3.4
- INQ000119469_0005 paras 2.4-2.5
- INQ000273553_0053 para 8.26
- INQ000116811_0042, 0226-0227 paras 6-9, 152
- INQ000148969_0003
- INQ000148969_0003-0004
- INQ000249526_0055 para 175
- INQ000216096_0001
- INQ000216096_0001
- ‘Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the Diamond Princess cruise ship, February 2020’, T.W. Russell, J. Hellewell, C.I. Jarvis, K. van Zandvoort, S. Abbott, R. Ratnayake, et al., Euro Surveillance (2020), 25(12), 2000256 (https://doi.org/10.2807/1560-7917.ES.2020.25.12.2000256; INQ000262586_0001)
- ‘Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the Diamond Princess cruise ship, February 2020’, T.W. Russell, J. Hellewell, C.I. Jarvis, K. van Zandvoort, S. Abbott, R. Ratnayake, et al., Euro Surveillance (2020), 25(12), 2000256 (https://doi.org/10.2807/1560-7917.ES.2020.25.12.2000256; INQ000262586_0001)
- INQ000273553_0048 para 8.17; ‘Estimating the infection and case fatality ratio for coronavirus disease (COVID-19) using age-adjusted data from the outbreak on the Diamond Princess cruise ship, February 2020’, T.W. Russell, J. Hellewell, C.I. Jarvis, K. van Zandvoort, S. Abbott, R. Ratnayake, et al., Euro Surveillance (2020), 25(12), 2000256 (https://doi.org/10.2807/1560-7917.ES.2020.25.12.2000256; INQ000262586_0001)
- INQ000310090_0001 para 6
- ‘CMO for England announces 4 new cases of novel coronavirus’, Department of Health and Social Care, 23 February 2020 (https://www.gov.uk/government/news/cmo-for-england-announces-four-new-cases-of-novel-coronavirus; INQ000237541_0002)
- INQ000303288_0007
- INQ000136744_0001
- INQ000233292
- INQ000346137_0013
- INQ000346137_0014
- INQ000346137_0014
- INQ000048445_0005;
INQ000065693_0009-0010 - INQ000425518_0004 para 12
- INQ000425518_0004 para 13
- INQ000425518_0008-0012
- INQ000238705_0009 para 44
- INQ000146565_0001
- INQ000146565_0001
- INQ000255836_0019 para 70
- INQ000056140_0004
- INQ000129852_0006
- Mark Drakeford 13 March 2024 50/1-9
- INQ000106129_0003 para 10
- INQ000106129_0002-0003
- INQ000106129_0002 para 9
- INQ000409251_0078 para 321
- INQ000106129_0002-0003
- INQ000106129; INQ000116811_0045 para 163
- INQ000249526_0047 para 146
- INQ000056216_0006 para 11
- INQ000056216_0005 para 1
- INQ000056216_0006 para 11
- Civil Contingencies Act 2004 (https://www.legislation.gov.uk/ukpga/2004/36/contents); INQ000273747_0008 para 23
- INQ000136747_0002
- INQ000411550_0046-0047 para 124
- INQ000146569; INQ000221567_0017 para 52
- INQ000174667_0003; INQ000182332; Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3
March 2020 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380) - INQ000146569_0001 para 1
- INQ000146569_0001 para 2
- INQ000146569_0002 para 6
- INQ000146569_0002 para 8
- INQ000146569_0003, 0005 paras 11, 20
- INQ000255836_0024 para 104; INQ000146569
- INQ000255836_0024 para 102
- INQ000255836_0024 para 102
- INQ000136750_0002
- INQ000146636_0021
- INQ000371209_0025 para 79; ‘Coronavirus: WHO issues “highest alert” over coronavirus’, BBC News, 28 February 2020 (https://www.bbc.co.uk/news/live/world-51669434; INQ000573842)
- This was one of two surveillance systems launched in late February in an effort to understand the prevalence of Covid-19 infections (INQ000273553_0045
para 8.13). - INQ000249526_0079 para 240
- ‘Effectiveness of airport screening at detecting travellers infected with novel coronavirus (2019-nCoV)’, B.J. Quilty, S. Clifford, CMMID nCoV working group, S. Flasche, R.M. Eggo, Euro Surveillance (2020), 25(5), 2000080 (https://doi.org/10.2807/1560-7917.ES.2020.25.5.2000080; INQ000255395_0004)
- INQ000023107
- INQ000255836_0083 para 315
- ‘Wuhan coronavirus: Health Secretary’s statement to Parliament’, Department of Health and Social Care and Matt Hancock, 27 January 2020 (https://www.gov.uk/government/speeches/wuhan-coronavirus-health-secretarys-statement-to-parliament; INQ000237587_0002); ‘Statement from the Chief Medical Officer for Wales about Coronavirus (2019-nCoV)’, Welsh Government, 31 January 2020 (https://www.gov.wales/statement-chief-medical-officer-wales-about-coronavirus-2019-ncov; INQ000048722); INQ000254430_0002 para 12
- INQ000251645_00181 para 9.20
- INQ000146564_0002
- INQ000232194_0027 para 108; INQ000269203_0117 para 8.9; INQ000183899_0001; INQ000106058_0002; INQ000091660_0008-0009 para 22
- ‘Travel ban implemented to protect public health following South Africa COVID-19 outbreak’, Department for Transport, 23 December 2020
(https://www.gov.uk/government/news/travel-ban-implemented-to-protect-public-health-following-south-africacovid-19-outbreak; INQ000054383);
‘Government confirms mandatory hotel quarantine to be introduced from 15 February’, Department of Health and Social Care, 5 February 2021 (https://www.gov.uk/government/news/government-confirms-mandatoryhotel-quarantine-to-be-introduced-from-15-february; INQ000054610) - INQ000216567
- INQ000216505; INQ000216513
- INQ000251645_0086 para 7.76
- INQ000049464_0002-0003; INQ000237603_0001
- INQ000049470_0006
- John Edmunds 19 October 2023 53/23-54/9
- Incident Management Team Report Conference Outbreak – March 2020, Public Health Scotland, 5 October 2021, p31
(https://publichealthscotland.scot/media/9575/incident-management-team-report-conference-outbreak-march-2020-oct21-english.pdf; INQ000147544) - INQ000251645_0086 para 7.76
- INQ000269203_0058 para 6.72
- INQ000273841_0020 para 32(vii); INQ000056137_0006; INQ000056138_0007
- Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 4 (https://covid19.public-inquiry.uk/documents/module-1-full-report); UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- Helen MacNamara 1 November 2023 27/2-4
- Dominic Cummings 31 October 2023 159/24-160/2
- INQ000272142; INQ000048313_0009
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- Christopher Whitty 22 June 2023 95/7-10; Christopher Whitty 21 November 2023 121/1-7; UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000396878_0081-0082 para 318
- INQ000267867_0036 para 150
- Mark Drakeford 13 March 2024 61/19-62/25
- INQ000047559_0004
- INQ000339033_0058 para 151
- INQ000255836_0010-0011, 0021 paras 25, 85; INQ000136747_0001
- INQ000255836_0021 para 84
- INQ000136747_0001
- INQ000232194_0053 para 222
- Alex Thomas 13 October 2023 30/5-16
- INQ000391237_0038 para 152
- INQ000273747_0007 para 20
- Frank Atherton 4 March 2024 27/15-18
- INQ000235213_0006 para 18
- O’Neill 14 May 2024 42/2-17
- INQ000412903_0069 para 217; Michelle O’Neill 14 May 2024 41/23-42/17; INQ000317453
- INQ000252711_0005 para 21
- INQ000302484_0017 para 62(a)
- INQ000273841_0014 para 26
- INQ000273841_0015 para 27
- INQ000273553_0103-0104 para 16.5
- INQ000255836_0015 para 48; Boris Johnson 6 December 2023 70/2-71/23
- Boris Johnson 6 December 2023 70/2-71/23
- INQ000255836_0020 paras 78-79
- INQ000146569_0001 para 1
- INQ000273553_0102 para 16.2
- INQ000061519_0004 para 13
- INQ000273553_0102 para 16.2
- INQ000273553_0102 para 16.2
- INQ000273553_0102 para 16.2
- INQ000309529_0038-0039 para 129
- INQ000238826_0015-0016 para 35; The 2009 Influenza Pandemic: An Independent Review of the UK Response to the 2009 Influenza Pandemic,
Dame Deirdre Hine, para 4.49, recommendation 10 (https://assets.publishing.service.gov.uk/media/5a7975f1ed915d0422068a10/the2009influenzapandemic-review.pdf; INQ000022705_0077) - Christopher Whitty 21 November 2023 48/16-49/3, 57/10-59/23; INQ000251645_0020 para 2.42
- Christopher Whitty 21 November 2023 163/1-164/24
- INQ000250231_0020 para 105
- Jonathan Van-Tam 22 November 2023 173/4-25
- Mark Sedwill 8 November 2023 30/1-9
- Mark Sedwill 8 November 2023 48/6-9
- Boris Johnson 6 December 2023 76/1-3
- Simon Stevens 2 November 2023 39/17-21, 40/7-10
- Christopher Whitty 21 November 2023 187/2-3
- Christopher Whitty 21 November 2023 184/11-13, 183/9-12
- INQ000103216; INQ000352140; INQ000352261
- Gregor Smith 22 January 2024 111/15-112/14
- Mark Woolhouse 24 January 2024 30/24-31/21
- INQ000238704_0004 para 19; INQ000339033_0059 para 153
- INQ000129852; Mark Drakeford 13 March 2024 57/14-25
- Mark Drakeford 13 March 2024 38/15-16
- Mark Drakeford 13 March 2024 38/15-19
- INQ000273747_0006 para 16; Mark Drakeford 13 March 2024 46/19-24
- INQ000273747_0007-0008 para 22
- INQ000371209_0024 para 74
- INQ000449440_0003-0004 para 4
- INQ000183597_0001; INQ000183632;
INQ000092712_0001-0002 para 3 - Chris Stewart 2 May 2024 53/23-54/11
- David Sterling 1 May 2024 103/10-24, 150/12-20
- See Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 5 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000273878_0012 para 35
- Michael McBride 10 May 2024 73/6-7
- Mark Drakeford 13 March 2024 52/7-14
- INQ000346190; Nick Phin 19 January 2024 192/12-193/9
- COVID-19: Make it the Last Pandemic, The Independent Panel for Pandemic Preparedness and Response, 17 September 2020, p29 (https://theindependentpanel.org/wp-content/uploads/2021/05/COVID-19-Make-it-the-Last-Pandemic_final.pdf; INQ000183545)
Chapter 3: The first 12 days of March 2020
Introduction
| 3.1. | By 1 March 2020, it was clear that Covid-19 had reached the UK and was a dangerous virus that potentially transmitted asymptomatically, and that sustained community transmission had likely occurred. In the absence of a scaled-up system for test, trace and isolate, the number of cases could not be calculated with any accuracy. The testing capacity in England was limited to only 2,100 samples per day.1 Additional testing was being carried out in the devolved nations, but this was also limited.2 |
| 3.2. | During the first 12 days of March 2020, it became apparent that containment of the virus had been lost. Community testing was ended and the next phase of the response commenced. This chapter examines the approach pursued by the UK government and devolved administrations to attempt to slow the growth of the virus during those crucial few days as it – and its appalling impact – spread around the UK. |
Figure 3: Daily confirmed cases from 1 to 12 March 2020 across the UK
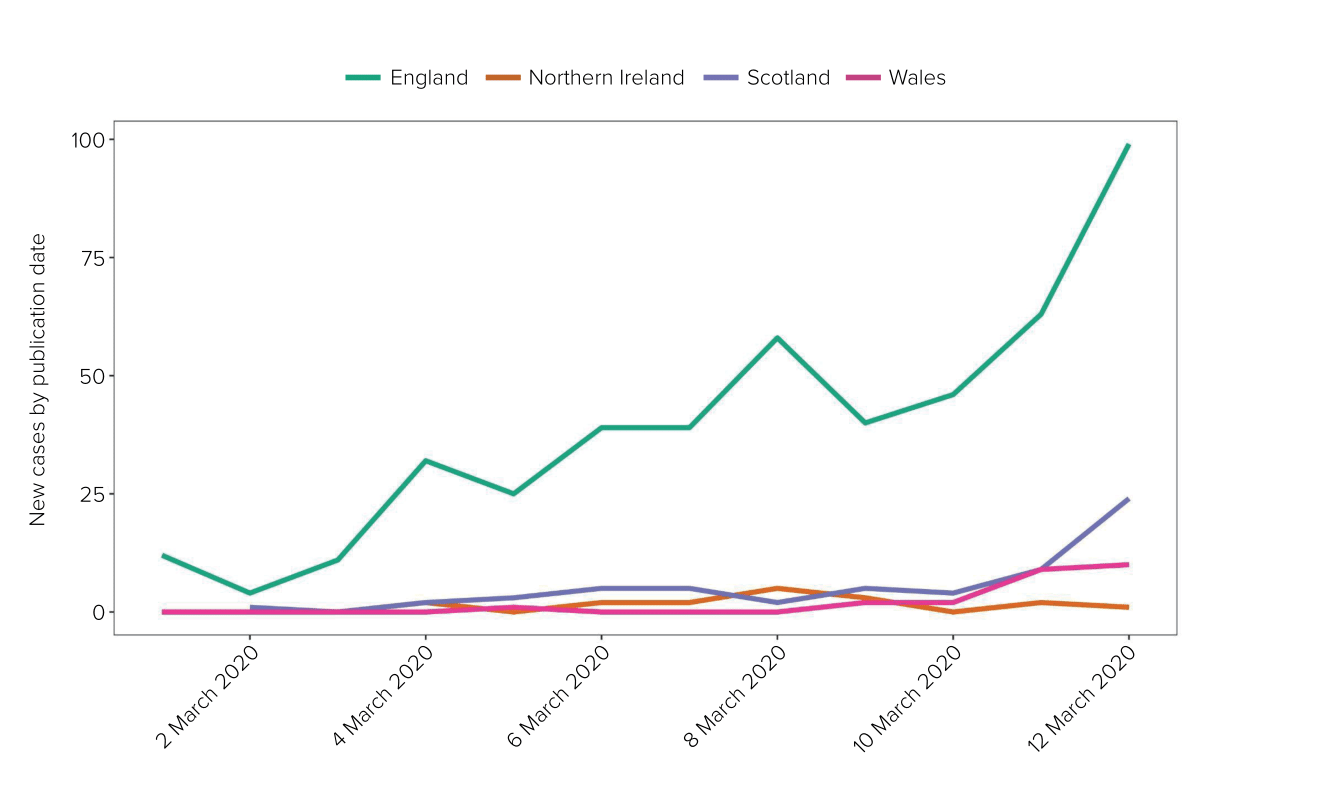
Source: UK Health Security Agency Covid-19 data dashboard archive
(https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
1 to 3 March 2020
| 3.3. | On 1 March 2020, Professor (later Sir) Christopher Whitty, Chief Medical Officer for England from October 2019, announced that a further 12 people had tested positive for Covid-19 in England. This brought the total number of confirmed cases to 33 in England and 35 across the UK, including those previously reported in Northern Ireland and Wales.3 Jeane Freeman MSP, Cabinet Secretary for Health and Sport in the Scottish Government from June 2018 to May 2021, confirmed the first positive test in Scotland from someone who had recently travelled from northern Italy.4 |
| 3.4. | On the same day, the UK government announced that a public health information campaign and “battle plan” for Covid-19 would be published later that week.5 Covid-19 would be:
“a standing item on the weekly Cabinet agenda, with the PM [Prime Minister]continuing to oversee the government approach.”6 The battle plan was also stated to be: “based on the government’s existing contingency plans for responding to a pandemic flu outbreak, but has been adapted to take account of the differences between COVID-19 and pandemic influenza.”7 |
| 3.5. | Modelling groups from Imperial College London, Oxford University and the London School of Hygiene & Tropical Medicine met with NHS England clinical leaders and planners at Imperial College London on 1 March 2020.8 The purpose of this meeting was “to test whether the emerging view that the NHS would not have sufficient capacity to cope was correct”.9 NHS England explained that the meeting established:
“a shared ground and common set of model parameters in modelling upon which to work out what would need to be done for the NHS to be able to cope. A key omission in the initial SPI-M-O [Scientific Pandemic Infections Group on Modelling, Operational sub-group]work that was resolved in this workshop, was that it did not include accurate model parameters about the length of stay; the correction of which rapidly increased some of the concerns about lack of capacity.”10 The subsequent modelling estimated: “that under a [reasonable worst-case] scenario, the NHS would be unable to meet all demands placed on it, with demand on beds being likely to overtake supply well before the peak was reached”.11 |
| 3.6. | This modelling, which was presented at a meeting of the Scientific Advisory Group for Emergencies (SAGE) on 3 March 2020 (see below), should have been available well before 1 March.12 SPI-M-O was responsible for producing modelling to inform UK government decision-making about implementing restrictions.13 However, its ability to produce robust modelling was contingent on information being provided to it by NHS England to ensure that modelling parameters were accurate.14 Professor Graham Medley (Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine and Co-Chair of SPI-M-O from January 2020 to February 2022) explained that the modelling variables required clinical input from NHS colleagues.15 SAGE had therefore noted as an action point on 20 and 27 February 2020 the need for NHS England to provide information to enable SPI-M-O to carry out robust modelling on the impact of Covid-19 on the NHS.16 NHS England, in turn, required input from SAGE and SPI-M-O in terms of agreed parameters and assumptions to work to.17 |
| 3.7. | SPI-M-O modellers and NHS England met on 1 March 2020.18 It was only when they did so that they reached a consensus on modelling parameters necessary to enable SPI-M-O to produce robust modelling on NHS England capacity in the reasonable worst-case scenario.19 NHS England explained that the correction of model parameters relating to length of hospital stay at this meeting “rapidly increased some of the concerns about lack of capacity”.20 |
| 3.8. | It is clear that efforts were made by all parties to achieve agreement on these parameters and assumptions to inform the modelling from mid to late February 2020, including the attendance of NHS England at a SPI-M-O meeting on 26 February, where it presented NHS modelling.21 Further, all were working in a period of uncertainty and with incomplete and evolving data. However, it is likely that the model presented to SAGE on 3 March 2020 would have been available sooner had there been swifter coordination and discussion between the parties about what was required. |
| 3.9. | Helen MacNamara (Deputy Cabinet Secretary from January 2019 to February 2021) described the tone of meetings in early March 2020 with Boris Johnson MP (Prime Minister from July 2019 to September 2022) as “jovial” and told the Inquiry there was a general view that “in implementing containment measures and suspending work and schooling, the Italians were overreacting”.22 Edward Udny-Lister, Lord Udny-Lister (Chief Strategic Adviser to the Prime Minister from July 2019 to November 2020 and Chief of Staff to the Prime Minister from November 2020 to February 2021), said that there was a sense that the UK would not be as badly impacted by Covid-19 as Italy:
“[T]here was a feeling that we are going to do better than this, it’s not going to be as bad as that.”23 |
| 3.10. | The Northern Ireland Executive Committee held its first substantive discussion about Covid-19 on the morning of 2 March 2020.24 Professor (later Sir) Michael McBride, Chief Medical Officer for Northern Ireland from September 2006, advised that most people would experience minor illness, with about 5% of cases requiring hospital care and a case fatality ratio of 2% to 3%. He advised that the peak could last up to 15 weeks but that a widespread pandemic was not inevitable and planning should consider all eventualities.25 |
| 3.11. | Robin Swann MLA (Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024) accepted that, as at 2 March 2020, the message that the Department of Health (Northern Ireland) was conveying to ministers in Northern Ireland was that Covid-19 would not necessarily become a pandemic.26 He conceded:
“[T]he failure may have been in the level of the alert or the seriousness that was moved up … I’m not sure as each level went up that we were ringing the bell loud enough as it went on, for other departments, other ministers in other areas actually to take up their actions and their responsibilities as well.”27 |
| 3.12. | COBR met on the morning of 2 March 2020.28 This was the first COBR meeting about Covid-19 chaired by Mr Johnson. His involvement signalled to UK government departments that the crisis was a whole-system civil emergency and required a whole-of-government response. As a result, the role of the Department of Health and Social Care as lead government department fell away, with key decisions and overall policy responsibility taken over by 10 Downing Street and the Cabinet Office.29 This meeting was attended by the First Ministers and deputy First Ministers of the devolved nations, health ministers and Chief Medical Officers. Professor Whitty advised COBR that:
“contact tracing for the source of infection for the last two cases in the UK had not been successful and that in both France and Germany there was now sustained community transmission … the aim for the DELAY phase, if CONTAIN failed, was to delay the peak of infections, to reduce the peak, and to minimise loss of life”.30 Professor Whitty also noted that SAGE was “looking at measures for social distancing” and “this advice would be ready in the following few days”.31 COBR agreed that parliamentary time would be allocated for new legislation (discussed further in Chapter 13: Legislation and enforcement, in Volume II) as well as the primary response document of the four governments, the Coronavirus: Action Plan, discussed below.32 |
| 3.13. | Vaughan Gething MS, Minister for Health and Social Services in the Welsh Government from May 2016 to May 2021, recalled that, at the meeting, Mr Johnson said “people should go about business and lives in normal manner”.33 Mark Drakeford MS, First Minister of Wales from December 2018 to March 2024, said that Mr Johnson’s views created “a certain inhibition on some of the advice being taken as seriously as I think it was being proposed to us”.34 |
| 3.14. | Following the COBR meeting, Nicola Sturgeon MSP (First Minister of Scotland from November 2014 to March 2023) chaired a ministerial-led Scottish Government Resilience Room meeting.35 There was a discussion about measures such as social distancing at this meeting, but this was not “in relation to any immediate concern” in Scotland.36 Dr Catherine Calderwood, Chief Medical Officer for Scotland from April 2015 to April 2020, said that it was not expected that Scotland would need to move from the containment phase for a number of months, as there was only one positive case in Scotland.37 However, she noted that it was necessary to have in place “a clear exit strategy from Social Distancing” before Scotland moved to the ‘delay’ phase and started to implement restrictions.38 |
| 3.15. | Mr Drakeford updated the Welsh Cabinet about COBR discussions and confirmed that a Welsh Cabinet sub-group would be formed (known as the Covid-19 Core Group), including ministers and key officials involved in the response.39 On 2 March 2020, the Chair and the Chief Executive of Public Health Wales wrote a joint letter to Mr Gething, advising him that Public Health Wales continued to operate at an “enhanced” emergency response level and was mobilising as if it was in a major incident.40 |
| 3.16. | Richard Pengelly, Permanent Secretary to the Department of Health (Northern Ireland) from July 2014 to April 2022, had written to the Chief Executives of health and social care trusts on 26 March 2020, warning them that:
“In the weeks and months ahead, it will be more important than ever for Trusts to implement effective discharge arrangements for patients as soon as they are well enough to leave hospital in order to release beds for newly admitted patients. Trusts should also work to maximise and utilise all spare capacity in residential, nursing, and domiciliary care.”41 |
| 3.17. | On 2 March 2020, Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, advised Matt Hancock MP (Secretary of State for Health and Social Care from July 2018 to June 2021) and officials in the Department of Health and Social Care and 10 Downing Street that there was a “1 in 5 chance” of the reasonable worst-case scenario materialising.42 |
| 3.18. | On the same day, Health Protection Scotland was notified that a delegate who had attended a conference at a central Edinburgh hotel between 25 and 27 February 2020 had tested positive for Covid-19 while overseas.43 On 3 March, Health Protection Scotland recorded a further positive case in Scotland of an individual who had also been at the conference.44 A multi-agency Incident Management Team was activated and tracing of the delegates was undertaken. Of the 71 delegates at the conference, 23 subsequently tested positive for the virus – there were also 16 secondary cases among people who had direct contact with delegates.45 Subsequent genomic sampling of the virus as part of investigations into the outbreak determined that hundreds of viral strains had been introduced into Scotland in February and March 2020.46 The Incident Management Team later found that it was likely that:
“[T]he first introductions of SARS-CoV-2 in Scotland dated back as far as 19 February. This indicates that community transmission was likely to have occurred undetected up to 1–2 weeks earlier than the first detected cases.”47 Although Ms Sturgeon was in favour of disclosing the link between the conference and the first positive cases in Scotland to the public, she was ultimately persuaded not to by Dr Calderwood due to concerns about patient confidentiality.48 |
| 3.19. | At a press conference on 2 March 2020, Mr Drakeford described Wales and the UK more generally as “well prepared”:
“We have implemented our planned response and we have robust infection control measures in place to protect public health.”49 |
| 3.20. | SAGE met on 3 March 2020.50 It considered a paper from SPI-M-O, whose advice had developed significantly since February 2020. SPI-M-O now agreed that it was “highly likely” that there was sustained transmission of Covid-19 in the UK.51 It was no longer only a “realistic possibility” but “almost certain” that sustained transmission would become established in the UK in the coming weeks.52 The doubling time (the length of time that it would take for the number of new Covid-19 infections to double) was estimated to be four to six days.53 |
| 3.21. | This was a critically important measure for understanding how much time remains before a wave of infections will become large enough to overwhelm resources and reach its natural peak, although it is unclear whether or when SPI-M-O’s advice about the high likelihood of sustained transmission in the UK reached decision-makers. It was likely that transmission had outpaced the UK’s test and trace capacity by 3 March 2020 and therefore that containment had already been lost. SAGE was also hindered by a lack of knowledge about how many infections there were within the UK at this time, as a result of the limited number of tests available. |
| 3.22. | SAGE also considered a paper produced by modellers from the London School of Hygiene & Tropical Medicine in collaboration with NHS England following the meeting on 1 March 2020, which advised that an unmitigated epidemic, in which people did not change behaviour, could:
“result in 570,000 deaths … in England and result in a peak demand of 990,000 non-ICU [intensive care unit]beds … and 130,000 ICU beds … at peak”.54 This was many times greater than the estimated 3,654 intensive care unit beds in England at the end of January 2020 (of which 83.3% were then occupied). In any event, not all of these beds would have been capable of providing invasive mechanical ventilation.55 |
| 3.23. | On 3 March 2020, SAGE discussed the impact of potential behavioural and social interventions on the spread of a Covid-19 epidemic in the UK.56 In a paper presented to COBR the following day, it advised:
“In the event of a severe epidemic, the NHS will be unable to meet all demands placed on it. In the reasonable worst-case scenario, demand on beds is likely to overtake supply well before the peak is reached.”57 The paper proposed implementing restrictions to change the curve (ie the number of new cases over time), “making the response of the NHS and other sectors more sustainable”,58 but stated: “It should be noted that whatever the reduction in peak NHS bed demand achieved by these interventions, in the reasonable worst-case scenario demand will still greatly exceed supply.”59 Discussions within SAGE therefore focused on “non-clinical interventions to reduce and delay Covid-19 transmission”, to be implemented during the delay phase of the response, including social distancing for over-65s.60 It also remained of the view that there was no evidence that banning very large gatherings would reduce transmission.61 |
| 3.24. | This followed advice on the use of behavioural and social interventions from the Scientific Pandemic Insights Group on Behaviours (SPI-B), which noted that the UK government “should advise against greetings such as shaking hands … as a signal about the importance of hand hygiene”.62 SPI-B also warned that “the efficacy of each intervention will be reliant on peoples’ willingness to adhere, as well as the practicality of adhering to each measure” and that:
“A number of measures will require Government to rethink existing financial arrangements, e.g. home isolation for those on zero hours contracts who are ineligible for sick pay, people who are in receipt of universal credit or job seekers allowance unable to present themselves at job centres.”63 SPI-M-O’s advice to SAGE was that restrictions reducing contact would flatten the peak. Stringent measures would be expected to have greater impact but “a large increase in cases would be expected” once they were lifted.64 The London School of Hygiene & Tropical Medicine’s advice included an assessment of a range of measures, including closing schools, ‘cocooning’ the elderly, social distancing measures and case isolation (as well as combinations of these).65 It stated that the restrictions needed to be implemented near the peak for maximum effect.66 |
| 3.25. | During Scottish Cabinet discussions on 3 March 2020, it was noted that “there was little evidence of community transmission in the UK, and new cases tended to be in ‘clusters’” and a “relatively slow increase in the number of cases” of the virus was foreseen.67 Although only two positive cases had been detected in Scotland by this time, this reflected a lack of testing rather than a genuine absence of cases. In early March, Scotland had capacity for just 350 daily tests.68 Although community sampling programmes were being implemented, just 914 people had been tested for the virus in Scotland by 3 March.69 The Scottish Cabinet recognised that the response would move to the delay phase in the “near future”.70 |
| 3.26. | At a UK Cabinet meeting on 3 March 2020, Mr Hancock said that there were 39 Covid-19 cases in the UK and the number was expected to rise.71 He explained that “the scientific advice was that a global pandemic could be averted but that was increasingly unlikely”.72 Mr Hancock confirmed that the Coronavirus: Action Plan would set out how the government might respond and that public health messaging would emphasise the importance of good hygiene, but “other than that, it was business as usual”.73 Mr Johnson confirmed that the UK was still in the ‘contain’ phase.74 |
| 3.27. | The first 10 Downing Street press conference was held on 3 March 2020.75 Mr Johnson stressed that the country was “extremely well prepared” and that “for the vast majority of the people of this country, we should be going about our business as usual”.76 His confident announcement failed to reflect the gravity of the situation. |
| 3.28. | Mr Johnson also stated that he:
“was at a hospital the other night where I think there were actually a few coronavirus patients and I shook hands with everybody … and I continue to shake hands”.77 On 3 March 2020, SPI-B advised SAGE that: “[T]he Government should advise against greetings such as shaking hands and hugging, given existing evidence about the importance of hand hygiene.”78 Mr Johnson told the Inquiry that this advice had not reached him by the time of the press conference.79 Nonetheless, it was unwise of him to have shaken hands with people and then to have publicly spoken about it. |
| 3.29. | Dominic Cummings (Adviser to the Prime Minister from July 2019 to November 2020) and James Slack (Director of Communications from November 2020 to March 2021) were concerned that Mr Johnson had not struck the appropriate tone at the press conference on 3 March 2020 and that he would need to be “forcibly stopped” from saying it was business as usual.80 In a message on the same day to Lee Cain (Director of Communications at 10 Downing Street from July 2019 to November 2020), Mr Cummings said that Mr Johnson:
“doesn’t think it’s a big deal … his focus is elsewhere, he thinks it’ll be like swine flu and he thinks his main danger is talking economy into a slump”.81 |
| 3.30. | Following the COBR meeting on 2 March 2020, Mr Gething asked for his diary to be cleared. Mr Drakeford said this was to allow Mr Gething to “focus exclusively on coronavirus”.82 However, on 3 March, an official who led the Resilience Team (the group within the Welsh Civil Service responsible for leading the response to civil emergencies in Wales) described the Emergency Coordination Centre (Wales) (discussed in Chapter 2: The emergence of Covid-19, in this volume) as “operating in support of the health agenda”.83 It was not considered “a civil emergency situation”.84 Dr Quentin Sandifer, Executive Director for Public Health Services and Medical Director at Public Health Wales from October 2012 to December 2020, was:
“astonished at this. I mean, we’re at the beginning of March, and Welsh Government resilience team were telling us that they didn’t think we were approaching, if we weren’t already there, a civil emergency.”85 |
| 3.31. | When asked when Covid-19 became the most significant matter on the Welsh Government’s priority list, Mr Drakeford said:
“probably 4 March … we are now meeting every week as a Cabinet specifically on this matter, so our core group is established”.86 The Inquiry notes that Mr Drakeford did not attend the Welsh Cabinet meeting on 4 March 2020, having travelled to Brussels as part of St David’s Day celebrations.87 The first case of Covid-19 had been announced in Wales just days earlier. It is unfortunate that Mr Drakeford was not in attendance, particularly as the response to Covid-19 was, at this stage, by Mr Drakeford’s admission, the Welsh Government’s priority.88 |
| 3.32. | It was only on 3 March 2020 that the Scottish Cabinet appears to have prioritised discussion of Covid-19 in its meetings.89 It was agreed at this meeting that the Covid-19 outbreak should “continue to be treated as an urgent priority across all portfolios”.90 |
| 3.33. | A briefing note prepared by the Civil Contingencies Policy Branch of The Executive Office, Northern Ireland on 3 March 2020 advised that “[a]s the preparations move beyond the health space there is an increasing need for co-ordination of the wider non-health work”.91 It recommended that the First Minister and deputy First Minister “note the escalating position in relation to Covid-19 and the need to make preparation for dealing with a potential outbreak of the disease” in Northern Ireland.92 It suggested: “The Executive may wish to meet to consider the impacts of an outbreak of Covid-19 in NI.”93 Nevertheless, The Executive Office did not, at that time, seek formally to initiate a coordinated, cross-governmental civil contingencies response. Consequently, the Department of Health (Northern Ireland) remained the lead government department and the Northern Ireland Executive Committee continued to have a relatively limited role. |
| 3.34. | The gravity of the situation was yet to be fully appreciated by the UK government and devolved administrations or reflected in their actions. |
The initial plan for the response
| 3.35. | Having been agreed by COBR the previous day, the Coronavirus: Action Plan was published on 3 March 2020.94 It set out in extremely high-level terms the plan that the four nations of the UK intended to follow in their responses to the virus, including the following phases:
“Contain: detect early cases, follow up close contacts, and prevent the disease taking hold in this country for as long as is reasonably possible Delay: slow the spread in this country, if it does take hold, lowering the peak impact and pushing it away from the winter season Research: better understand the virus and the actions that will lessen its effect on the UK population; innovate responses including diagnostics, drugs and vaccines; use the evidence to inform the development of the most effective models of care Mitigate: provide the best care possible for people who become ill, support hospitals to maintain essential services and ensure ongoing support for people ill in the community to minimise the overall impact of the disease on society, public services and on the economy.”955 This reflected the “contain, delay, research and mitigate” framework that began to be identified in late January 2020, as discussed in Chapter 2: The emergence of Covid-19, in this volume, although Mr Johnson believed that the first time he saw this sequence was in a briefing presented on 28 February 2020.96 |
Contain phase: Stopping the spread of the virus through test and trace
| 3.36. | As explained in the Coronavirus: Action Plan, the UK government and devolved administrations sought first to stop the spread of the virus by using test and trace to find cases and requiring those infected people to self-isolate, as well as requiring individuals who returned from areas abroad where cases were reported to quarantine.97 This was the contain phase. |
| 3.37. | This was an entirely sensible approach to take. However, containment of any virus is heavily reliant upon the ability to test and to detect cases and trace close contacts, as well as on the generation time of the virus being long enough for contact tracing efforts to keep pace. Two diseases with the same reproduction number (R) can spread at different speeds, depending on the generation time. As explained by Professor John Edmunds (Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine), viruses with a short generation time, such as pandemic influenza, move so fast that “it’s really impossible to keep up with it with contact tracing” (identifying the source and contacts linked to a confirmed case of an infectious disease).98 |
Three available options, should containment fail
| 3.38. | In the event that test and trace capacity was outpaced by the spread of the virus and its spread could therefore no longer be prevented through that means, the contain phase would be over. |
| 3.39. | At that point there were, on the Inquiry’s analysis, three distinct options available to the four governments for the next immediate phase of their response:
|
Option 1: No restrictions and allow the virus to spread at its natural pace
| 3.40. | Governments could choose to put no restrictions in place and allow the virus to spread through the population (sometimes known as ‘unmitigated spread’). In this approach, R would not be affected and the virus would therefore spread exponentially through the population over a relatively short period of time. |
| 3.41. | The perceived benefit of this approach is that the population would become infected with the virus and most would recover over a relatively short period of time. A potential consequence of this is that it may create a degree of immunity in the population among people who have been infected with the virus (known as population immunity or ‘herd immunity’) relatively quickly. Population immunity is a complex scientific concept.99 In general terms, it refers to the point where there is a large number of people in the population who have some immunity to the virus (either through infection or vaccination), there are fewer people able to be infected and, as a result, the amount of the virus in circulation begins to decline until it dies out and the pandemic comes to an end. |
| 3.42. | Any such immunity would reduce the risk of the population being severely impacted by a second wave of infections. However, this consequence is not guaranteed, as some viruses do not lead to population immunity through infection. This can be the case if reinfection is possible because individual immunity is not particularly high or does not last a long time. In those circumstances, as Professor Whitty explained, population immunity “will fail to control the virus, which will continue to spread in the community”.100 It was not known in March 2020 whether population immunity through infection was in fact possible in relation to Covid-19. |
| 3.43. | The obvious downside of this approach is that large numbers of people may die and become ill with the virus. Additionally, this is likely to happen over a short period of time, therefore creating a severe strain on health services as well as other public services and the economy, as large numbers of people become too ill to work. |
Option 2: Some restrictions to slow the spread of the virus (a mitigation strategy)
| 3.44. | Governments could put in place some restrictions to slow down the spread of the virus among the population (known as a mitigation strategy). Examples of relevant restrictions include advising people with virus symptoms to self-isolate and advising everyone to limit their social contacts. |
| 3.45. | The effect of these restrictions is that R is reduced, but it would remain above 1. The epidemic would continue to grow, but not as quickly as it otherwise would have. |
| 3.46. | The benefit of implementing restrictions to slow the spread of the virus is that it prevents as many people becoming infected with the virus at the same time as would have been the case in the absence of restrictions. This creates some time for effective treatments to be developed and reduces the strain on the health service as a result of an infection over a longer period of time. The downside of the approach of slowing the spread is that it still allows the number of infections to grow and therefore a significant number of people will still become infected with the virus. |
| 3.47. | As explained above, a possible consequence of this may be that, when the restrictions are lifted, there is a degree of population immunity, thereby reducing the population’s vulnerability to any future waves of the virus. However, this is far from guaranteed, since infection may not lead to immunity. Further, even if immunity through infection were possible, there is a possibility that the public would voluntarily start to reduce its social contact out of fear of the virus, thereby reducing the possibility of population immunity being achieved through this approach. |
Option 3: Stringent restrictions to stop the spread of the virus (a suppression strategy)
| 3.48. | The final option would be to put in place stringent restrictions – such as a mandatory ‘stay at home’ order or ‘lockdown’ – to stop the spread of the virus (known as a suppression strategy). |
| 3.49. | The effect of these stringent restrictions is that R is reduced below 1, so that the number of people infected with the virus begins to decline. The benefit of this approach is that there will be fewer infections and deaths than under either of the other approaches. However, the downside is that stringent restrictions come with significant social and economic impacts. This is particularly so if the restrictions remain in place for a prolonged period of time. A suppression strategy is also not a solution in itself. The number of infections will quickly start to grow again once restrictions are lifted, as the population will not have any immunity to the virus (known as an ‘exit wave’). |
| 3.50. | An exit strategy from the stringent restrictions therefore needs to be put in place to prevent or reduce the impact of this exit wave of infections. The exit strategy could involve the development of effective treatments or a vaccine, or driving down infections to a level that can be contained within test and trace capacity. However, this may take considerable time and, as a result, restrictions may need to be periodically reintroduced until effective countermeasures are available. |
Delay phase: Slowing the spread of the virus through restrictions
| 3.51. | On the Inquiry’s analysis, the three options above were available to the four governments for the next phase of their response after the contain phase was over. They pursued a mitigation strategy of imposing some restrictions to slow the spread of the virus (Option 2). This was known as the delay phase. |
| 3.52. | The Coronavirus: Action Plan explained that, during the delay phase of the response, restrictions would be put in place to slow the spread of the virus and reduce the peak by spreading out Covid-19 infections over a longer period.101 This effect was also described as “flattening the peak”, “reducing the peak”, “delaying the peak”, “flattening the curve”, “a one peak strategy” and “squashing the sombrero”.102 Mr Johnson told the Inquiry that this approach was based on Professor Whitty’s advice that:
“[A]t a certain number of cases, the NHS becomes overwhelmed and collapses. The consequences would be catastrophic and therefore, as the curve increases, we have to flatten it.”103 |
| 3.53. | It is clear from statements made by Professors Whitty and Vallance in mid-March 2020 that the intended purpose of the delay phase was to slow the spread of the virus in order to reduce the number of cases at any one time, rather than to stop its spread entirely. Professor Whitty told COBR on 9 March that the delay response was intended to change “the shape of the virus curve, as opposed to suppressing it”.104 Similarly, at a COBR meeting on 12 March, Professor Vallance explained that the aim of implementing the interventions under consideration “was not to completely suppress the spread of the disease”.105 He explained:
“[N]ot only was this not possible, but it would likely lead to a larger second peak later in the year when the NHS may be under increased pressure.”106 |
| 3.54. | Even if it was practically possible, it was probably politically impossible for the UK government and devolved administrations to choose to do nothing in response to the virus (Option 1). On 5 March 2020, during a TV interview, Mr Johnson stated:
“[P]erhaps you could take it on the chin, take it all in one go and allow the disease, as it were, to move through the population, without taking as many draconian measures.”107 |
| 3.55. | Media reporting of Mr Johnson’s comments gave rise to public concern that this was the intention.108 However, Mr Johnson clarified during the interview that the plan for the UK government’s response was to “take all the measures that we can now to stop the peak of the disease being as difficult for the NHS as it might be”.109 Indeed, the Inquiry heard from a number of witnesses that it was never the UK government’s plan to take no action at all and to allow the virus to spread through the population unchecked.110 |
| 3.56. | There was, however, a discussion at a meeting chaired by Mr Johnson on 12 March 2020 about whether it was possible to shield older people and the vulnerable while allowing the virus to spread among the rest of the population. At this meeting, Sir Mark Sedwill (later Lord Sedwill), Cabinet Secretary and Head of the Civil Service from October 2018 to September 2020, suggested that members of the public could be told it was better for them to catch the virus and get it over with, using an analogy of ‘chickenpox parties’ to spread the virus.111 Lord Sedwill told the Inquiry that he was seeking to explore whether there was a way of managing it spreading through those people:
“for whom the disease was likely to be unpleasant rather than dangerous, and that we could quarantine and shield those for whom it would be dangerous”.112 Mr Johnson confirmed that this formed part of: “a free-flowing discussion … to assess whether it might be sensible to allow the vast majority of younger people to get the disease (and therefore become immune) while protecting the elderly”.113 But Mr Johnson said that the idea was “immediately dispensed with”.114 Lord Sedwill explained that he dropped the ‘chickenpox parties’ analogy because he realised that it was causing confusion as to whether he had misunderstood the seriousness of Covid-19.115 In any event, it ultimately became clear that the capabilities were not in place to make this approach a viable option in March 2020.116 |
| 3.57. | However, the Inquiry heard that no proper debate took place prior to the publication of the Coronavirus: Action Plan about whether it was appropriate to attempt to stop the spread entirely rather than simply slow it (Option 3). Dr Ben Warner, Special Adviser to the Prime Minister from December 2019 to May 2021, said that he was:
“not aware of any meeting where the Prime Minister was asked to choose between a mitigation or suppression strategy”.117 Imran Shafi, Private Secretary to the Prime Minister for public services from March 2018 to March 2021, told the Inquiry: “I don’t think there was a proper discussion in February about suppress [stopping the spread] or mitigate[slowing the spread].”113 |
| 3.58. | The approach of slowing, rather than stopping, the spread of the virus pursued in the first half of March 2020 (Option 2) had its origins in the UK Influenza Pandemic Preparedness Strategy 2011. This was intended to be adaptable to another type of virus.119 It stated:
“[I]t almost certainly will not be possible to contain or eradicate a new virus in its country of origin or on arrival in the UK. The expectation must be that the virus will inevitably spread and that any local measures taken to disrupt or reduce the spread are likely to have very limited or partial success at a national level and cannot be relied on as a way to ‘buy time’.”120 It explained that to attempt to stop the spread of a new pandemic influenza virus “would be a waste of public health resources and capacity”.121 Instead, it suggested that the spread should be slowed through limited measures, such as advising those infected with the virus to stay at home, minimising close contacts and adopting hygiene practices.122 |
| 3.59. | The approach to a response to a pandemic therefore long anticipated that – in the absence of scaled-up test, trace and isolate capacity – the spread of a virus would have to be managed, as any measures intended to stop the spread would not be successful. |
| 3.60. | Sir Christopher Wormald (Permanent Secretary to the Department of Health and Social Care from May 2016 to December 2024) told the Inquiry that, in the Department of Health and Social Care, “the presumption was that we would be following, basically, the flu plan”.123 Similarly, Mr Shafi explained:
“I think the system, Number 10 [Downing Street] included, defaulted into accepting that the pandemic flu … approach, which is more of a mitigate approach [slowing the spread]rather than a suppress [stopping the spread]approach, was the right way forward.”124 |
| 3.61. | Mr Hancock understood that the UK government’s approach, as set out in the Coronavirus: Action Plan, was “predicated, explicitly, on the inevitability of global spread”.125 Lord Sedwill explained that “the scientific advice was … not that the virus could be stopped, but that its spread and serious incidence could only be managed”.126 Mr Cain said:
“[I]t was felt that a widespread Covid-19 infection could not realistically be stopped so government planning needed to focus on how it could be managed.”127 |
| 3.62. | This was reflected in the Coronavirus: Action Plan, which stated:
“[I]t may be that widespread exposure in the UK is inevitable; but slowing it down would still nonetheless be beneficial.”128 |
| 3.63. | There was also a widely held view that putting in stringent restrictions to stop the spread of the virus would only lead to a wave of infections later in the year when the restrictions were lifted. This was articulated in a SPI-M-O consensus statement of 2 March 2020, a London School of Hygiene & Tropical Medicine paper of 3 March, a Civil Contingencies Secretariat paper of 6 March, by Professor Vallance at COBR on 12 March, on the BBC Radio 4 Today programme on 13 March, by SAGE on 13 March and in a WhatsApp message to Mr Johnson on 14 March.129 |
| 3.64. | Professor Whitty explained this concern to the Inquiry:
“If you go for a suppression strategy [of stopping the spread], for however long you do it … at a certain point you will have to release it, and then the pandemic is still with you and then you will have what is called in epidemiology an exit wave … So essentially the wave comes at the point you choose to release the measures … So this is trying to make clear to people: if you go for suppression, don’t think that that’s your problem done, you just have to suppress for a bit and you’re done. At some point you’re going to have to face this, and the question is: at what point do you want to? … But the idea that you can, absent an extremely effective vaccine, suppress and then not have an exit wave, is not realistic.”130 |
| 3.65. | A severe exit wave could only be avoided if stringent restrictions were maintained until an effective vaccine or treatment was widely available. This was not considered to be a realistic prospect because of concerns that the public might not be able to comply with stringent restrictions for a long time. Mr Cain told the Inquiry that the UK government had been advised that “a suppression strategy wouldn’t work, people could only sort of undergo … 12 weeks of this kind of … hard measures”.131 |
| 3.66. | It was also likely to be politically unpalatable to have stringent restrictions in place for such a long time, given their social and economic downsides. It was therefore understood that, as Professor Vallance advised COBR on 12 March 2020, attempting to stop the spread of Covid-19 in the initial months of 2020 would simply postpone a wave of infections, potentially to a time when the NHS was already under strain from seasonal illnesses like influenza.132 |
| 3.67. | The possibility of population immunity arising as a result of slowing rather than stopping the spread was seen as a welcome potential by-product of this approach.133 At the COBR meeting on 12 March 2020, Professor Vallance described:
“a good outcome being that by September 2020 herd [population] immunity would be established”.134 |
| 3.68. | At a 10 Downing Street press conference the same day, Professor Vallance explained that, in the context of the response during the delay phase:
“It’s not possible to stop everybody getting it. And it’s also actually not desirable because you want some immunity in the population. We need to have immunity to protect ourselves from this in the future.”135 Professor Vallance made similar comments in the media on 13 March 2020 and estimated that 60% of the population would need to have some immunity to Covid-19 for population immunity to be achieved.136 He told the Inquiry that he had been trying to explain that “an increased level of immunity in the population was a by-product of the policy of ‘flattening the curve’”.137 |
| 3.69. | It was not known in early 2020 whether a vaccine could be developed. The plan to slow the spread of the virus was premised on an assumption that imposing some restrictions to keep the spread of Covid-19 more manageable would offer the most likely exit strategy from the pandemic in the absence of effective treatments, a vaccine or scaled-up test and trace. It was thought that it would enable population immunity through natural infection to be built up and therefore reduce the risk of waves of infection occurring later in the year when the NHS might be under more strain from seasonal influenza. However, this was not guaranteed, since it was not known in March 2020 whether people could be infected more than once. The risk of reinfection and the mutation of the virus into new variants could have meant population immunity would not be achieved through infection. |
| 3.70. | The intention for the response to Covid-19 during the delay phase was therefore to slow the spread of the virus, based on an assumption that population immunity was an important potential, if not guaranteed, consequence of adopting this approach. |
| 3.71. | However, some in the UK government did not appreciate that being infected with Covid-19 would not necessarily give rise to immunity from the virus subsequently.138 Professor Whitty told the Inquiry that, while population immunity was discussed by some at the centre of the UK government, he was “not certain that they had always fully understood it”.139 For example, Ms MacNamara explained:
“[I]n March 2020 our working assumption was that getting immunity was a once-and-done event, at least for the foreseeable future. There was no discussion I remember about the risk of being re-infected or that the virus might mutate so rapidly.”140 Similarly, Lord Udny-Lister said there was a belief in the UK government that “the quicker we actually all caught it, the quicker we would have immunity from it”.141 |
Objectives of the delay phase
| 3.72. | The delay phase had two high-level objectives, which were implied in the Coronavirus: Action Plan:
|
| 3.73. | The Coronavirus: Action Plan explained that slowing the spread of the virus would also be beneficial as it “buys time for the testing of drugs and initial development of vaccines and/or improved therapies or tests to help reduce the impact of the disease”.144 It explained that restrictions would be implemented during the delay phase to slow the spread of the virus to achieve these objectives, while also seeking “to minimise the social and economic impact”.145 |
Restrictions to be implemented during the delay phase to achieve objectives
| 3.74. | The Coronavirus: Action Plan set out only very limited detail about the restrictions that could be implemented during the delay phase. It referred to these as:
“population distancing strategies (such as school closures, encouraging greater home working, reducing the number of large scale gatherings).”146 |
| 3.75. | Given the plan was only to slow the spread of the virus rather than to stop it, no mention was made in the Coronavirus: Action Plan of more stringent restrictions, such as a stay at home order or other forms of lockdown. However, it stated:
“[O]ur experts are considering what other actions will be most effective in slowing the spread of the virus in the UK, as more information about it emerges.”147 |
| 3.76. | Indeed, the day before its publication, Professor Whitty had advised COBR that SAGE was preparing advice on options for social distancing.148 The plan for the response during the delay phase was therefore far from fully formed when the Coronavirus: Action Plan was published. Mr Hancock told the Inquiry that, on reflection, there were “not nearly as much” action points in the Coronavirus: Action Plan as he wished there had been.149 |
The timing of implementation of restrictions during the delay phase
| 3.77. | The Coronavirus: Action Plan did not set out how or when decisions would be taken about the implementation of restrictions during the delay phase. It said only that these decisions would be “based on … scientific evidence, and take into account the trade-offs involved”.150 While it was understandable that, as a public-facing document, the Coronavirus: Action Plan did not set out this level of detail, there should have been an internal plan that did so. |
| 3.78. | However, prior to mid-March 2020, scientific advice was provided on the timing of the implementation of the restrictions during the delay phase. Professors Whitty and Vallance advised that the implementation of restrictions should be delayed so that they were in place during the peak of infections and for the shortest time necessary to reduce the strain on the NHS. For example, on 2 March 2020, Professor Whitty advised COBR: “The interventions to delay the spread of the virus must not be implemented too early in order to ensure maximum effectiveness.”151 |
| 3.79. | In March 2020, a number of UK government scientific advisers privately and publicly explained that restrictions should not be implemented too early in order to limit the period of time during which they were in place.152 It was critical to have high compliance with the restrictions over the peak, and scientific advisers made clear on a number of occasions that restrictions should not therefore be implemented too soon, due to the perceived risk of ‘behavioural fatigue’.153 This was most clearly put by Professor Whitty at a 10 Downing Street conference on 12 March, when he said:
“[I]f people go too early, they become very fatigued. This is going to be a long haul. It is very important we do not start things in advance of need … an important part of the science on this is actually the behavioural science. What that shows is probably common sense to everybody … which is that people start off with the best of intentions, but enthusiasm at a certain point starts to flag … So we do need to do it at the last point which is reasonable so that people maintain their energy and enthusiasm to get through what will be quite difficult things to do.”154 The impact of the notion of behavioural fatigue on the timing of the implementation of restrictions in the initial months of 2020 is discussed in detail in Chapter 4: Realisation and lockdown, in this volume. |
| 3.80. | At the time these comments were made, it was already clear from NHS modelling that, if the reasonable worst-case scenario did materialise, the NHS in England would be overwhelmed, even if the restrictions of self-isolation, household isolation and shielding were implemented.155 |
| 3.81. | On 13 March 2020, in light of comments made concerning the risk of behavioural fatigue, SAGE felt it necessary to assert that this notion was not an appropriate basis on which to delay the intervention of restrictions:
“There is no strong evidence for public compliance rates during a major emergency … Difficulty maintaining behaviours … should not be taken as a reason to delay implementation where that is indicated epidemiologically.”156 |
The trigger for moving from ‘contain’ to ‘delay’
| 3.82. | The Coronavirus: Action Plan stated:
“The decision to step up the response from Contain to Delay and then Mitigate will be taken on advice from the UK’s [Chief Medical Officers], taking into account the degree of sustained transmission and evident failure of measures in other countries to reduce spread.”157 The UK Influenza Pandemic Preparedness Strategy 2011 contained a similar trigger of “evidence of sustained community transmission of the virus” for moving on from its initial response stage of ‘detection’.158 |
| 3.82. | Although the Coronavirus: Action Plan placed reliance on there being some evidence of sustained transmission before the trigger for the response to move to the delay phase would be met, it did not quantify the extent of transmission that was required. While this was understandable, given the public-facing nature of the Coronavirus: Action Plan, the four governments (with input from their Chief Medical Officers) should have ensured that there was an internal plan for the response which set out a more specific test that the Chief Medical Officers would apply to determine when decision-makers should be advised that this point in the response had been reached. |
The Coronavirus: Action Plan
| 3.84. | As outlined in Chapter 2: The emergence of Covid-19, in this volume, the Coronavirus: Action Plan was commissioned by Mr Hancock on 10 February 2020 as “a coronavirus version” of the UK Influenza Pandemic Preparedness Strategy 2011.159 Professor Whitty described it as “the best account of policy planning undertaken in February 2020”.160 |
| 3.85. | While the Coronavirus: Action Plan was a four-nations publication, its development and content were primarily driven by the UK government.161 Although Professor Vallance reviewed scientific aspects of the Coronavirus: Action Plan and Professor Whitty contributed to it, it was not seen or approved by SAGE.162 Professor McBride explained that it was discussed and “signed off” by the Minister of Health (Northern Ireland) and the First Minister and deputy First Minister at COBR.163 Mr Drakeford told the Inquiry that its substance “was driven by the UK Government”, with engagement with the devolved administrations to ensure that it was “unanglocentric”.164 Nonetheless, he agreed that:
“At the time the Plan was written it seemed to me to be an accurate reflection of the assessments made by the people best placed to understand the data and respond to it.”165 The Scottish Government anticipated that there might be a need for a “differential Scottish approach”, reflecting “potential differences” between Scotland and the rest of the UK, including “distinctive features” (such as its remote, rural and island communities), but ministers also recognised that “a consistent, simple message covering all of the UK would be preferable”.166 |
| 3.86. | It took more than three weeks to draft and publish the Coronavirus: Action Plan.167 This was despite it being thought that the UK Influenza Pandemic Preparedness Strategy 2011 was sufficiently adaptable to deal with other respiratory diseases. As discussed in the Inquiry’s Module 1 Report, its approach was described as “ready for flu, ready for anything”.168 |
| 3.87. | Having taken too long to produce, the Coronavirus: Action Plan came too late and failed to reflect the spread of Covid-19 as known at the time of publication. When it was published, the UK was said still to be in the contain phase, but containment had effectively been lost. Professor Whitty told the Inquiry that “the contain stage of things was near or at its end pretty well at the point that this document hit the printing presses”.169 As was subsequently understood, there had also been “a huge influx from Spain, France and Italy over half term and beyond”, which Professor Vallance acknowledged “meant that we probably had lost control”.170 A study subsequently published on 11 June 2020 by the COVID-19 Genomics UK Consortium (a UK-wide collaborative network for Covid-19 genomics research and training) showed that the introduction of Covid-19 to the UK following the end of the February school half-term holidays was highly significant.171 |
| 3.88. | Mr Cain told the Inquiry that the Coronavirus: Action Plan “had little detail and was clearly only useful as a communications device”, commenting that it was a “strange document for people to be referring to as an actual government plan”.172 Dr Warner also described it at the time as a “comms [communications] plan”.173 He told the Inquiry that he had assumed there would be “a much more detailed internal document that addressed the complexity of the problem”.174 Ms MacNamara described the Coronavirus: Action Plan as:
“an extraordinary document, given that so many of the assertions about how well prepared we were would turn out to be wrong only weeks later … much of what was in the document had not been adequately tested or just was not true for the circumstances we were in.”175 |
| 3.89. | The Coronavirus: Action Plan was commissioned as “a public facing document, primarily for public reassurance”.176 While it was suitable as a public-facing document, there should have been a fully detailed internal four-nations plan that – unlike the Coronavirus: Action Plan – contained clearly defined and sufficiently specific objectives that the response sought to achieve, either collectively or in each nation. These objectives could have included, for example, the mortality number the four governments were willing to tolerate or the level of NHS capacity that could not be breached. The internal plan should also have outlined the relevant actions, trigger points and designated responsibilities for each potential restriction to enable them to be put into operation at the necessary time to achieve the intended objectives. As outlined in Chapter 2: The emergence of Covid-19, in this volume, such a plan was required by the end of February 2020, if not earlier. There was no such detailed plan. |
4 to 12 March 2020
| 3.90. | On 4 March 2020, the UK government launched a public health information campaign that focused on the importance of handwashing.177 |
| 3.91. | On the same day, COBR met again. It was chaired by Mr Hancock and attended by health ministers from the devolved administrations.178 |
| 3.92. | A SAGE paper prepared for the meeting stated: “In the event of a severe epidemic, the NHS will be unable to meet all demands placed on it.”179 It also outlined the scientific evidence for a number of proposed interventions (not including a stay at home order, since this was not in contemplation at this stage).180 As outlined above, it highlighted, even with these interventions:
“[W]hatever the reduction in peak NHS bed demand achieved by these interventions, in the reasonable worst-case scenario demand will still greatly exceed supply.”181 However, the minutes of the COBR meeting do not contain any discussion of this.182 |
| 3.93. | The SAGE paper also explained that any interventions implemented would need to be government policy for a significant duration, since relaxing them too early could “result in further peaks and potentially extend transmission of the virus into Winter 2020”.183 It noted that, the following day, SAGE would consider the optimal combination of interventions, the optimal point at which they should be implemented and the duration for which they should be in place to delay the peak (mitigation) or to contain the outbreak (suppression).184 Dr Stuart Wainwright, Director of the Government Office for Science from December 2019 to June 2023, informed COBR that combinations of the interventions in the SAGE paper had not yet been modelled and this would be done in the coming days.185 Mr Hancock stated that “the science was guiding them towards self isolation”.186 |
| 3.94. | COBR noted that analysis of the economic impact of the interventions had been completed, but analysis of the social impacts – noted by SAGE as potentially affecting society, individuals, the workforce and businesses, as well as the operation of government and public services – was still being undertaken.187 The Cabinet Office was asked to ensure that analysis of social distancing measures took into account their social and economic impact.188 UK government departments – and the devolved administrations – were asked to provide information on the impacts, challenges, cross-government interdependencies and societal impacts of various restrictions (giving the closure of schools as an example).189 This was work that the Cabinet Office regarded as likely to be already taking place in departments. |
| 3.95. | The Welsh Government responded to the request on 7 March 2020 and subsequently discussed provision of further information, including comparative data on the “demographic differences between England and Wales”.190 In Northern Ireland, Bernie Rooney, Deputy Director at The Executive Office from September 2019 to September 2020, contacted the Department of Health (Northern Ireland) but was told that it had not planned to reply.191 Professor McBride said:
“[W]e simply do not have the modelling capability to replicate and provide such granularity and have not previously sought to provide same. Given the unrealistic time frames it is not possible to provide any meaningful analysis.”192 Professor McBride considered that timeframes were being driven by the rapidly changing epidemic curve (or epicurve, a visual representation of the number of cases over time) and the need for imminent implementation of behaviour interventions in England. Notwithstanding evidence of community transmission in the Republic of Ireland, he thought Northern Ireland “was probably some few weeks behind”.193 The Inquiry saw no evidence that the Scottish Government responded |
| 3.96. | The Top Management Group within the Department of Health (Northern Ireland) had agreed to the full activation of the health Gold Command to provide strategic direction and advice (although only on 4 March 2020).194 This was not a cross-government coordination body. Ms Rooney also advised Chris Stewart (Director at The Executive Office with responsibilities for civil contingencies) of “strong views” about the need for an “NI Hub [a coordination centre for Northern Ireland] to be established as a matter of priority”, as well as a:
“[l]ack of structures and staff to respond to Cabinet Office requests – particularly the legislative requests for input to emergency Bill”.195 |
| 3.97. | Derek Baker (Permanent Secretary to the Department of Education (Northern Ireland) from February 2017 to November 2020) enquired about ‘standing up’ the NI Hub but was advised by David Sterling (later Sir David Sterling), Head of the Northern Ireland Civil Service and Permanent Secretary to The Executive Office from June 2017 to August 2020, that, at that time, this “would be premature”.196 |
| 3.98. | The Welsh Cabinet met on 4 March 2020. It noted:
“[T]he Welsh Government and partners had plans in place to deal with pandemic flu, which would now be tested.”197 The Cabinet was briefed about a new operating model that “outlined cross-government activities and support for Ministers and Cabinet”, including “specific issues, such as dealing with excess deaths, proposed emergency legislation and communications”, and that it would take “around three to four weeks to build the necessary capacity to support the structure”.198 (See Chapter 11: Government decision-making, in Volume II, regarding the establishment of the Covid-19 Project Team.) The minutes of the meeting reflected the lack of urgency among ministers in the Welsh Government, stating that ministers would “have a further opportunity to discuss developments at its regular meeting the following Tuesday”, which was six days later.199 |
| 3.99. | In contrast to their ministerial counterparts, following a meeting of officials within the Civil Contingencies Group (Wales), it was confirmed that:
“[W]hat was clear to us all this morning is that our work on COVID-19 must now pick-up pace and intensity.”200 |
| 3.100. | On 4 March 2020, in a message to Mr Cummings, Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021 and Minister for the Cabinet Office from February 2020 to September 2021, raised concerns about the Cabinet Office’s ability to deliver on government priorities and to deal with Covid-19 (see Figure 4). |
Figure 4: Exchange of messages between Mr Cummings and Mr Gove on 4 March 2020
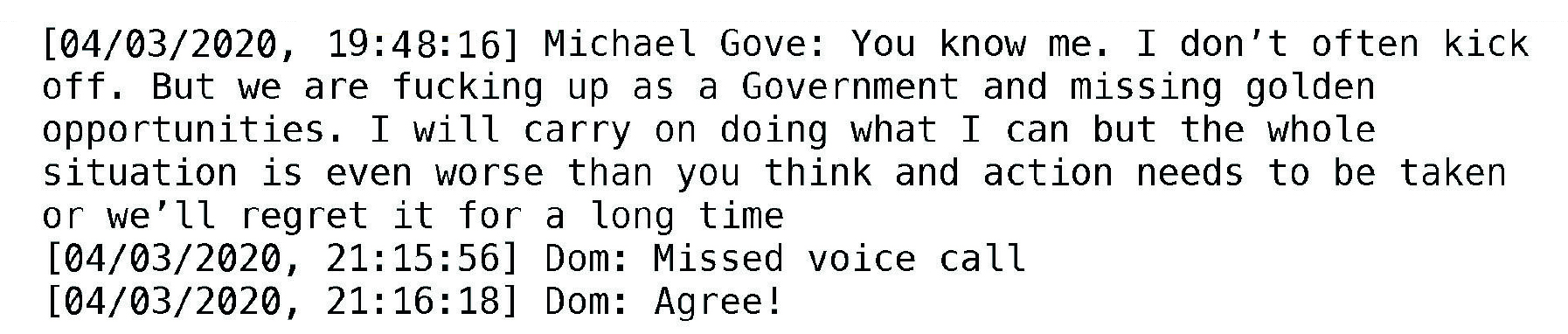
Source: INQ000275436_0003
| 3.101. | On 5 March 2020, the first death of a patient with Covid-19 in England was reported.201 A further 25 cases in England were identified, bringing the total number of cases in the UK to 115.202 |
| 3.102. | At a meeting of COBR COVID-19 (Officials) that day, chaired by Mr Johnson, Professor Whitty stated that:
“the prohibition of mass gatherings was not considered necessary from a scientific standpoint, and that widespread school closures were not yet necessary in the current phase of the outbreak”.203 Professor Whitty confirmed that the UK was “still in the containment phase but actively preparing for delay”.204 He also explained that there would be a “need to move to the Delay phase in the next seven to 14 days”.205 |
| 3.103. | Also on 5 March 2020, SAGE recommended implementation of self-isolation and household isolation within one to two weeks, followed roughly two weeks later by shielding of those aged over 65 and those with underlying medical conditions.206 It reiterated that there was no evidence that banning very large gatherings would reduce transmission.207 |
| 3.104. | SAGE concluded that the UK remained in the containment phase, noting that “there are currently no scientific grounds to move away from containment efforts in the UK”.208 However, earlier on 5 March 2020, Professor Vallance had advised Mr Johnson that SAGE was close to advising a move from the contain phase to the delay phase.209 As outlined above, this move was required even before the Coronavirus: Action Plan was published on 3 March. Professor Neil Ferguson, Mathematical Epidemiologist at Imperial College London, recalled:
“(quite possibly imperfectly) … that Chris Whitty was uncomfortable with the idea that the UK would be the first European country to abandon containment”.210 |
| 3.105. | On 6 March 2020, a Cabinet Secretariat briefing prepared for a later COBR meeting stated that the advice from SAGE was “that our response will soon need to move from contain to delay” and that containment was “now unlikely to be achievable”.211 It also advised on the possibility of an exit wave if stringent restrictions were implemented:
“[V]ery stringent social and behavioural interventions (such as those in China) have the potential to prevent a major epidemic establishing but risks a large epidemic re-establishing when lifted.”212 |
| 3.106. | The same day, the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) discussed how to explain “why facemasks were acceptable for healthcare staff but not the general public”.213 It noted that members of the public were not trained to use face coverings and that it was the use of face coverings alongside other personal protective equipment (PPE) that made face coverings effective at preventing contamination in a healthcare setting.214 |
| 3.107. | Also on 6 March 2020, Dr Rob Orford (Chief Scientific Adviser (Health) for Wales from January 2017) shared the eighth update from the Technical Advisory Cell with Dr (later Sir) Frank Atherton (Chief Medical Officer for Wales from August 2016) and Dr Andrew Goodall (Director General of Health and Social Services in the Welsh Government and Chief Executive of NHS Wales from June 2014 to November 2021), which attached simple modelling for the projected demands on health services in Wales.215 It projected that:
“Adjusting the model assumptions by simple scaling down [of the reasonable worst-case scenario] gives lower demand – but even with a 25% scaling, demand will exceed supply.”216 With interventions, the peak Covid-19 case load in Wales would still require almost 5,000 additional beds and over 1,400 additional intensive care beds.217 |
| 3.108. | In considering when it became clear that the NHS in Wales would be overwhelmed without taking action, Dr Goodall said that there was “definitely a switch from the last week of February into that first week of March”.218 |
| 3.109. | On 9 March 2020, a protocol for the move from ‘contain’ to ‘delay’ was agreed across the four nations on a draft basis, although advice remained that there were no scientific grounds for moving away from containment.219 It stated that the decision to move to the delay phase must be based on scientific advice and “jointly recommended” by the UK Chief Medical Officer (the Chief Medical Officer for England) and the Government Chief Scientific Adviser, “working in concert with the [Chief Medical Officers] of Scotland, Wales and Northern Ireland”.220 |
| 3.110. | On 8 March 2020, a Six Nations rugby match between Scotland and France went ahead in Edinburgh. Dr Calderwood and Health Protection Scotland had recommended the match be allowed to proceed on the basis that “there is no clear scientific evidence that cancelling the event would lessen the risk of exposure to coronavirus”.221 The first recorded death of a person with Covid-19 in Scotland was a French national who had visited Scotland to watch the game.222 It was understood that he had contracted the virus prior to travelling to Scotland.223 When the Scottish Government announced this first death on 13 March, Dr Calderwood described the deceased as being an older person with underlying health conditions who was being treated by Lothian Health Board.224 The Scottish Government did not disclose to the public at the time that he had attended the rugby match in Edinburgh. |
| 3.111. | On 8 March 2020, the Department of Health and Social Care reported that there had been more than 80,000 cases and more than 3,000 deaths in China and almost 6,000 cases and more than 200 deaths in Italy.225 That same day, a number of northern provinces in Italy were placed into an effective lockdown – this was extended to the whole of the country on 9 March.226 |
| 3.112. | In the UK, the total number of Covid-19 cases had increased to 273, including 244 cases in England, 18 in Scotland, 4 in Wales and 7 in Northern Ireland. There had been two deaths.227 |
| 3.113. | Data from systematic NHS surveillance (initiated in late February 2020) became available around 8 March 2020.228 Professor Edmunds told the Inquiry that positive cases were found through this surveillance “almost immediately”.229 According to Professor Edmunds, given the sensitivity of those surveillance systems, the identification of any cases might “indicate a large underlying epidemic”.230 Professor Edmunds explained that the data were, however, “very difficult to analyse” because there were delays of five to seven days between onset of cases and “confirmation and entry onto the database ” – although “some cases were taking up to 3 weeks to be recorded”.231 There were significant caveats to, and uncertainties in, the data available. |
| 3.114. | Mr Cain raised concerns on 8 March 2020 that the Department of Health and Social Care appeared to be overwhelmed and unable – or unwilling – to support the Cabinet Office work on interventions and the coordination of the response.232 |
| 3.115. | Modelling from NHS England on 9 March 2020 indicated that:
“NHS demand will greatly exceed supply before the peak of the virus is reached in a Reasonable Worst Case scenario (RWCS), meaning the NHS will be unable to meet the demands placed on it.”233 It also noted that NHS beds and critical care capacity would still be overwhelmed in the reasonable worst-case scenario, even if self-isolation, household isolation and social distancing for over-65s were implemented.234 |
| 3.116. | The same day, Professor Steven Riley, Professor of Infectious Disease Dynamics at Imperial College London, sent a paper to Professor Medley. It advised that measures akin to lockdown should immediately be implemented to avoid the NHS being overwhelmed.235 In his reply, Professor Medley made the point that the present approach being pursued by the four governments was based on:
“the assumption that herd immunity will develop after one infection … if we need multiple infections to develop immunity … then we are really in trouble”.236 |
| 3.117. | There was a growing recognition in the UK government and devolved administrations that the move from the contain phase to the delay phase was fast approaching. For example, at a COBR meeting for officials on 5 March 2020, chaired by Mr Johnson and attended by an official from the Welsh Government, Professor Whitty noted that the UK “will need to trigger Delay within the next week or fortnight”.237 Mr Gething told the Inquiry that he was informed of the discussion at the meeting and he therefore understood at this point that there would be a “need to move to the Delay phase in the next seven to 14 days”.238 On the same day, Professor Vallance advised Mr Johnson that SAGE was close to advising a move from contain to delay.239 The Scottish Cabinet recognised on 3 March that it was likely that the response would move to the delay phase in the “near future”.240 |
| 3.118. | On the evening of 8 March 2020, Mr Stewart told colleagues at The Executive Office of Northern Ireland: “The UK is approaching (but has not yet reached) the transition point from ‘contain’ to ‘delay’.”241 He explained that a COBR meeting the following day would:
“focus on those measures that will need to be adopted and maintained when that transition point is reached (soon)”.242 (emphasis in original) |
| 3.119. | COBR met on 9 March 2020, again chaired by Mr Johnson. It was attended by the First Minister and deputy First Minister of Northern Ireland and the First Ministers of Scotland and Wales, as well as their health ministers and Chief Medical Officers.243 Sir Christopher Wormald explained that, by the time of this meeting, “it was widely expected … we would move from contain to delay”.244 The purpose of the meeting was therefore to agree which restrictions to slow the spread should remain in development and what the priority should be for work on them.245 Mr Johnson was briefed that he should ask Professors Whitty and Vallance to confirm at the meeting that they still expected to advise on or around 11 March that the triggers for moving from ‘contain’ to ‘delay’ had been met.246 |
| 3.120. | A paper presented at the meeting stated “advice from SAGE is that our response will soon need to move from contain to delay”.247 It also explained that SAGE had considered the effectiveness of these interventions against different objectives, including containing the outbreak so that it did not become an epidemic and slowing the spread (mitigation).248 The paper noted that containing the outbreak through the use of restrictions was “now unlikely to be achievable”.249 It is clear from the fact that SAGE was considering the effectiveness of potential restrictions to achieve different objectives that, even at this point, the UK government had still not made clear to SAGE its objectives for the response. |
| 3.121. | COBR considered “planned interventions to delay the virus’ peak” in three stages:“1. Self isolation of symptomatic individuals. 2. Full house-hold isolation where one individual is symptomatic.3. A series of currently undetermined measures to safeguard the elderly and vulnerable individuals.“250 |
| 3.122. | Professor Vallance explained that these interventions aimed to reduce “the peak of the virus to enable the NHS to cope with demand and to reduce the mortality rate”.251 SAGE had advised that both individual self-isolation (for those with “mild respiratory symptoms”) and household isolation (“for all individuals living in the same household as someone who is ‘symptomatic’”) should be implemented by 13 March 2020 to maximise effectiveness, with a decision on these measures to be made by 11 March.252 COBR recognised that Scotland, Wales and Northern Ireland were not at the same stage as England and that the island of Ireland faced the additional challenge of having two separate jurisdictions with different public messaging.253 |
| 3.123. | Professor Whitty advised COBR that the public should be reminded to self-isolate for serious, influenza-like symptoms and that this was not a change in medical advice. He confirmed that the next step would be for mildly symptomatic people to self-isolate and that this should be communicated within the next 10 days.254 Professor Whitty also said that scientific advice supported early implementation of self-isolation, although household isolation and measures for vulnerable people and the elderly could be triggered later.255 He warned COBR that “the timing of implementation of measures was crucial” because measures might “be in place for months and public compliance or despondence was heavily dependent on timing”.256 |
| 3.124. | No decision was made at the COBR meeting on 9 March 2020 about implementing the three restrictions of self-isolation, household isolation or shielding, although an action was raised for SAGE to “set out the thresholds for triggering each of the three interventions”.257 The delay phase was imminent. COBR should have asked SAGE to identify the trigger points for the implementation of restrictions during the delay phase long before this point. |
| 3.125. | COBR decided to “advise people with serious flu-like symptoms to stay at home today, in line with existing medical advice” and that it should consider at a meeting on 11 March 2020 whether to advise people with mild symptoms to do the same.258 Ms Sturgeon and Mr Drakeford had raised their concerns at the meeting that advising only people with serious influenza-like symptoms to self-isolate – and not those with mild symptoms – did not reflect the restriction outlined in SAGE’s paper for their consideration.259 Mr Johnson stated that the next COBR meeting would discuss self-isolation for people with mild symptoms, household isolation and shielding.260 The issue of whether the implementation of restrictions was timely is analysed in detail in Chapter 4: Realisation and lockdown, in this volume. |
| 3.126. | On 10 March 2020, Mr Drakeford updated the Welsh Cabinet about COBR discussions, stating that the timing of the implementation of restrictions was critical, since if they:
“were used prematurely it would likely lead to the population being less receptive to messages at a time when the spread of the virus was more virulent”.261 |
| 3.127. | The Top Management Group within the Department of Health (Northern Ireland) met on 9 March 2020 but, even at this late stage, was only considering the possibility of invoking Northern Ireland Central Crisis Management Arrangements (known as NICCMA) to involve The Executive Office further. This was to be discussed further with the Chief Medical Officer.262 Further, the Department of Health (Northern Ireland) was still debating whether to advise that these civil contingency arrangements should be initiated in Northern Ireland.263 While the Department of Health (Northern Ireland) did provide updates to officials in other departments, the Executive Committee (through the Minister of Health) and The Executive Office – and provided strategic public health advice – it fundamentally underestimated the scale of Covid-19 and the risk it presented in Northern Ireland and failed to appreciate the need for urgent, ministerially sponsored, whole-of-government action. |
| 3.128. | SAGE met again on 10 March 2020.264 By this date, there were 319 confirmed cases in the UK, but SAGE advised there were likely to be as many as 5,000 to 10,000 cases and transmission was “underway in community and nosocomial (i.e. hospital) settings”.265These estimates were based on approximations by Professors Medley and Ferguson, who had sought to gain an understanding of the degree to which cases in the UK had been underestimated. However, as Professor Ferguson told the Inquiry:
“[I]n retrospect that range was almost certainly a substantial underestimate, given [various data limitations and connected issues] … it is highly likely that many (if not most) COVID-related deaths were missed in the UK prior to 11th March 2020.”266 |
| 3.129. | Professor Ferguson told the Inquiry that, at this meeting, he asked the 10 Downing Street officials present “if they knew what an epidemic with 4000-6000 deaths per day would feel like”.267 He later emailed Dr Warner in 10 Downing Street, stating that he would like Mr Johnson to see graphs in an Imperial College London paper that indicated the NHS would be overwhelmed under the interventions being considered and deaths would still likely peak at 4,000 to 6,000 a day.268 Professor Ferguson told Dr Warner:
“While this got called the reasonable worst case until today, this is my Centre’s best estimate of what might happen. Even allowing for uncertainty, we will still see at least half of those numbers … So long as the PM and Cabinet accept and understand this is what is likely to happen and are still happy to proceed with current plans, then there is a rational basis to that decision which I would say the science supports … But what would be the worst outcome – in my opinion – would be to go for mitigation (the policy package currently being discussed) and for the health, social and political cost to be judged later to be unacceptable – necessitating a policy pivot in the midst of what will already be a national crisis .”269 Professor Ferguson later told the Inquiry that he would not have sent these emails had he been satisfied that his views were being properly reflected in SAGE and communicated to the UK government through Professors Whitty and Vallance.270 |
| 3.130. | The Cheltenham Festival took place from 10 to 13 March 2020.271 On 11 March, a Champions League football match took place in Liverpool.272 SAGE had advised on 10 March that “public gatherings pose a relatively low but not zero public risk … But it acknowledged the importance of advice in this area and agreed to review it.”273 A paper was therefore provided by the London School of Hygiene & Tropical Medicine on 11 March, which concluded the following:
“Banning sporting events has a negligible impact on the epidemic. Reducing all leisure contact, which mainly occurs in pubs/bars, restaurants and cinemas would have a much larger (though still modest) impact on the epidemic.”274 |
| 3.131. | On 10 March 2020, Mr Shafi suggested the NHS England modelling dated 9 March should be included in the papers for the COBR meeting on 12 March and stated that it was “frightening that even if we pull all levers we are still overwhelmed”.275 Even at this stage, decision-makers in the UK government had failed to understand that there was a real risk the reasonable worst-case scenario would materialise and, as a result, the NHS in England would be overwhelmed. This was despite, as outlined above, an NHS England modelling paper being provided to COBR on 4 March, which indicated that, in a severe epidemic where the reasonable worst-case scenario materialised, the NHS would be overwhelmed before the peak was reached, regardless of the interventions put in place.276 |
| 3.132. | Mr Johnson told the Inquiry that, following his review of the daily update contained in his ministerial red box on 10 March 2020, “the potential consequences were becoming ever clearer”.277 The update advised that 8% of those diagnosed with the virus in the Lombardy region of Italy had died, due to its older population.278 Mr Johnson explained that this figure disturbed him, as Britain also had an elderly population.279 There were others with concerns. Mr Gove asked Mr Hancock and Mr Cummings probing questions about aspects of the UK government’s response, including about the provision of PPE, respirators and ventilators.280 As the Inquiry is examining in detail in Module 5: Procurement, the Department of Health and Social Care was working on the issue but, by this stage, it was known that procurement in a global pandemic would be a challenge.281 Mr Gove told the Inquiry that he sent this email as he was concerned the UK government “needed more challenge” to its assessment.282 |
| 3.133. | On 10 March 2020, the Scottish Cabinet discussed Covid-19 at length. Its conclusions suggest that the matter was discussed in far greater detail than on previous occasions and the tone of the record suggests a broader recognition of the gravity of the situation.283 The Cabinet was now considering the closure of schools and the cancellation of mass gatherings for behavioural reasons because it might:
“be a problem with the credibility of a public message advising significant restrictions of personal behaviour while allowing a ‘business as usual’ approach for large events”.284 It noted that the spread of the outbreak in Scotland was not out of proportion with that elsewhere in the UK and that: “[T]here was no current reason to depart from a concerted, UK-wide approach, guided by the evidence provided by the Scientific Advisory Group for Emergencies [SAGE] … the only reason for a departure from a UK-wide approach would be if the evidence suggested that there would be an advantage for the Scottish population in following a different course from the rest of the UK.”285 Its conclusions record the need for a cross-government response.286 The overall objective was said to be “to do everything possible to keep the number of severe cases to a minimum”.287 |
| 3.134. | On 10 March 2020, the Northern Ireland Executive Committee was briefed that there was no government advice to cancel large events but that organisers had called off various large gatherings, including various St Patrick’s Day parades.288 By this point, there were 16 cases of Covid-19 in Northern Ireland and 21 cases in the Republic of Ireland.289 In the meeting, Michelle O’Neill MLA, deputy First Minister of Northern Ireland from January 2020 to February 2022, said: “[Executive] approach needs to kick in – all need to contribute.”290 Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021, was noted to have asked: “Civil Contingencies – have we got plans to handle ?”291 These comments capture the Executive Committee’s belated realisation that responding to the pandemic would require a ministerially sponsored, cross-governmental response. Mr Swann agreed that, at that time, there was no real cross-departmental response to Covid-19 in Northern Ireland.292 |
| 3.135. | In an exchange with Professor Whitty, Professor McBride noted that he needed “to secure an all Ireland approach aligned with the UK”.293 An all-Ireland approach was, within days, to prove unrealistic. |
| 3.136. | On 11 March 2020, with more than 118,000 cases in 114 countries and 4,291 deaths, the World Health Organization declared Covid-19 to be a pandemic.294 It had deep concern over the “alarming levels of spread and severity, and by alarming levels of inaction”. The World Health Organization further stated:
“[W]e have called every day for countries to take urgent and aggressive action. We have rung the alarm bell loud and clear.”295 |
| 3.137. | That morning, Professor Whitty sent an email to Professor David Hunter, Professor of Epidemiology and Medicine at the University of Oxford, concerning the timing of the implementation of restrictions. Professor Whitty explained that “my main concern at the moment is sustainability if we go too early”.296 |
| 3.138. | On 11 March 2020, Mr Cummings sent a message to Mr Gove expressing his frustration that, contrary to assurances, the Cabinet Office did not have a plan for responding to Covid-19 (see Figure 5). |
Figure 5: Exchange of messages between Mr Cummings and Mr Gove on 11 March 2020

Source: Extract from INQ000275436_0003
| 3.139. | Mr Cummings also sent a message to a WhatsApp group of 10 Downing Street and Department of Health and Social Care advisers and officials, Mr Hancock and Professors Vallance and Whitty. He stressed that it was necessary for senior people to understand and discuss with Mr Johnson that “all sensible people can see the trajectory and how social distancing will be needed to flatten curve”.297 Mr Cummings referred to the fact that some were saying the risks of implementing restrictions too late were higher than those of going too soon and that “extremely clear scientific justification” would be needed if the introduction of social distancing was to be delayed for a further week.298 |
| 3.140. | The UK Cabinet met on the morning of 11 March 2020. Mr Johnson explained that: “[E]pidemiologists were clear that the timing of [the] introduction of [further interventions] was key to their effectiveness. Measures would be deployed only when the time was right.”299 Mr Hancock advised the UK Cabinet that: “[T]he key symptoms were a dry cough and a temperature. Without these symptoms, it was highly unlikely that someone was suffering from coronavirus.”300 Mr Hancock’s statement was incorrect. As outlined in Chapter 2: The emergence of Covid-19, in this volume, there was clear evidence (including reports from the Diamond Princess cruise ship) by February 2020 that someone could have Covid-19 and be asymptomatic. |
| 3.141. | The first case of community transmission of Covid-19 was reported in Wales on 11 March 2020.301 That same day, Public Health Wales identified Covid-19 as a potential “major (health) incident”.302 It noted that:
“Objectively the demographic characteristics of the Welsh population and specifically the age profile of the population over 65/75, health and economic status, and dependency responsibilities are such that Wales may experience disproportionate levels of impact from Covid-19.”303 |
| 3.142. | Public Health Wales recommended early implementation of home isolation, household quarantine and cocooning (or shielding) of vulnerable people, commending “urgent attention directed at the elderly population cared for in residential and nursing homes in Wales”.304 The Inquiry is considering the decisions affecting the adult social care sector in Module 6: Care sector. |
| 3.143. | Public Health England was also active at this time. It was still trying to develop an effective test and trace system, and it established the Covid-19 Hospitalisation in England Surveillance System (known as CHESS) to collect data relating to people hospitalised with the virus and provide real-time data on the utilisation of hospitals by these patients.305 |
| 3.144. | SPI-M-O met on 11 March 2020. It discussed the paper dated 9 March from Professor Riley, which set out reasons for the UK not to delay closing schools, to move to working from home and to implement any other possible social distancing, with a suggested initial three-week duration of additional interventions.306 He also suggested that the perceived benefits of slowing the spread of the virus might not be achieved if NHS critical care was overwhelmed and the public voluntarily began to socially distance as a result. He said there was:
“strong evidence with which to abandon mitigation strategies, justified in any way by the possibility of a short epidemic … we suggest that the first step is to adopt stringent fixed-term social distancing”.307 Professor Riley proposed an immediate switch to a suppression strategy of stopping the spread of the virus and discussed the possibility of using adaptive or repeated lockdown policies. It was agreed at the meeting that these scenarios should be modelled.308 This would be the first time that a lockdown, as it became known, had been “seriously considered” as a possible intervention.309 |
| 3.145. | SPI-M-O also produced a consensus statement on the matter of mass gatherings on 11 March 2020. It advised that stopping mass gatherings would only have a low impact on the spread of Covid-19, noting that “the risk to an individual from attending large events is generally no higher than in smaller events”.310 Cancelling mass gatherings could either lead to more epidemiologically risky displacement activities or, by contrast, could send a message to people that would lead them to change their behaviour and potentially slow the spread of the virus. However, it noted that:
“[I]t is not possible to quantify either of these effects. The impact of stopping all leisure activities, including public gatherings such as at bars and restaurants, would be expected to have a much larger effect on the population-level spread of the epidemic.”311 The following day, the Technical Advisory Cell advised that “only a modest reduction in the infection related deaths (2%) is predicted for restricting mass gatherings”.312 However, a Welsh Covid-19 Core Group meeting the same day recorded that “it would be difficult to justify not cancelling events”.313 |
| 3.146. | On the afternoon of 11 March 2020, Mr Hancock chaired a COBR meeting, attended by the First Minister of Northern Ireland, the Deputy First Minister of Scotland and the Director of Local Government in the Welsh Government.314 The purpose of this meeting was to agree a coronavirus bill, as it was intended that the following day COBR would discuss the move from ‘contain’ to ‘delay’ and interventions to slow the spread (despite SAGE having previously advised that a decision on interventions was required by 11 March).315 |
| 3.147. | Professor Whitty advised COBR that cases in the UK were rising, with an estimated 5,000 to 10,000 cases present. If no significant actions were taken to mitigate the upward trajectory, the peak would arrive in 10 to 14 weeks, with cases increasing rapidly from 6 weeks. It was believed that the UK was 4 to 6 weeks behind Italy, which was still some weeks away from its peak.316 Sir Simon Stevens (later Lord Stevens of Birmingham), Chief Executive of NHS England from April 2014 to July 2021, advised COBR that, in the reasonable worst-case scenario, NHS services would be under extreme pressure, but that:
“[I]n the event of a lower infection rate than in Lombardy, lower, but nonetheless high, pressure would still be experienced.”317 Sir Simon Stevens explained that elective surgery would need to be postponed to release 30,000 beds.318 COBR agreed that NHS England should liaise with its counterparts in the devolved administrations on decisions that might be required to surge health and care facilities, including cancellation of elective treatments.319 |
| 3.148. | The content of the emergency coronavirus bill was also agreed by COBR.320 The bill was based on the Pandemic Influenza (Emergency) Bill, which had been prepared in collaboration with the devolved administrations and finalised in 2019.321 Its development had been led by the Department of Health and Social Care, with input from the UK government and devolved administrations at both official and ministerial levels.322 It contained measures for use in the delay phase, to manage the peak of the outbreak, and created public health powers for the Scottish Government and Northern Ireland Executive to implement restrictions (such powers were already available to the UK and Welsh governments under the Public Health (Control of Disease) Act 1984).323 Mr Drakeford told the Inquiry that it was not until 20 March 2020 that there was a “looming reality” that public health powers would be used to respond to the pandemic.324 |
| 3.149. | On 11 March 2020, Professor (later Dame) Jenny Harries (Deputy Chief Medical Officer for England from July 2019 to March 2021) publicly stated that it would be detrimental for people without Covid-19 symptoms to wear a face covering:
“If a healthcare professional hasn’t advised you to wear a face mask, it’s usually quite a bad idea. People tend to leave them on, they contaminate the face mask and then wipe it over something. So it’s really not a good idea and doesn’t help.”325 |
| 3.150. | The Irish government followed the example of other countries such as Italy by announcing a package of measures that were to take effect from 18:00 on 12 March 2020 and remain in place until 29 March. These included the closure of schools, colleges and childcare facilities, the cancellation of all indoor mass gatherings of 100 people and outdoor gatherings of over 500 people, the closure of cultural institutions and the implementation of social distancing in restaurants and cafes. People were also advised to continue to work if they could, but to work from home where possible.326 This took ministers in Northern Ireland by surprise and showed Professor McBride’s hope of securing an all-Ireland approach that aligned with the UK to be unrealistic. Ms O’Neill said that the Irish government:
“took that decision and didn’t tell us. That wasn’t good enough, because that actually led and fed into that confusion and put us all in a very difficult spot.”327 |
| 3.151. | On 12 March 2020, Ms Foster and Ms O’Neill met with Mr Sterling, who advised that there was “no medical/scientific evidence” to support the measures announced by the Irish government.328 A note of the meeting records that Ms O’Neill referred to “one island and two approaches – need to identify which approach is right and which isn’t”.329 |
| 3.152. | The same day, at a further meeting attended by all Northern Ireland Executive ministers and permanent secretaries in Northern Ireland, Ms Foster explained:
“[T]he urgency of this meeting was driven by the statement this morning by the Taoiseach. DFM [deputy First Minister] referred to public confusion. While we continue to follow the science and medical advice, we are now in a difficult position given RoI [Republic of Ireland] approach.”330 Professor McBride advised that there was a risk in creating a peak too early and then inviting an additional peak. Conor Murphy MLA, Minister of Finance from January 2020 to October 2022, pointed to a need to understand why the advice in the Republic of Ireland was different. Ms Foster and Ms O’Neill subsequently took different positions publicly on the issue of school closures.331 The Northern Ireland Office noted that “cracks” were beginning to emerge in the Northern Ireland Executive, with Sinn Féin “wanting to follow Irish government particularly re school closures”.332 The impact of this is explored in greater detail in Chapter 11: Government decision-making, in Volume II. |
| 3.153. | On the morning of 12 March 2020, Ms Sturgeon decided that mass gatherings of more than 500 people should be cancelled from 16 March 2020.333 Although Dr Calderwood’s view was that cancelling mass gatherings, particularly those outdoors, would not have a significant impact on transmission, Ms Sturgeon made the decision for three reasons: (i) mass gatherings carried a risk of potential outbreaks that would be better avoided at this time; (ii) the impact of mass gatherings on the resources of the emergency services; and (iii) the risk that negative public perceptions about mass gatherings continuing might undermine the general public health advice.334 Ms Sturgeon told the Scottish Parliament at noon that day that she was minded to cancel mass gatherings in Scotland, subject to the views of the other three governments at the COBR meeting that afternoon.335 |
The move from ‘contain’ to ‘delay’ and self-isolation advice
| 3.154. | On the morning of 12 March 2020, Mr Cummings messaged Mr Johnson, warning him:
“We got big problems coming. CABOFF [Cabinet Office]is terrifyingly shit, no plans, totally behind the pace … We must announce TODAY – not next week – ‘if feel ill with cold/flu stay home’ … overwhelming danger here is being late and the nhs implodes … not being a week early.”336 |
| 3.155. | On 12 March 2020, SPI-B produced a consensus statement that expressed concern about displacement activities if mass gatherings were cancelled.337 However, it highlighted that the public expected mass gatherings to be banned in the UK – as they had been in other countries – and therefore advised that failing to ban them could risk the public viewing the government’s actions:
“as incompetent or not in the public’s best interests. It may also be taken as signifying that the situation is not expected to be severe for the UK. This could have knock-on implications for public attitudes to other recommendations made by Government.”338 |
| 3.156. | That same day, the UK Chief Medical Officers raised the risk level to the UK from ‘moderate’ to ‘high’.339 Professor Whitty explained that this was in response to the clear increase in transmission.340 |
| 3.157. | By 12 March 2020, containment had already failed.341 The Chief Medical Officers, along with SAGE, should have advised that the four governments move to the delay phase much earlier – around the time the Coronavirus: Action Plan was published at the latest. The evidence indicates that a move was not advised earlier because scientific advisers were unaware of how widely seeded the virus was in the UK and how short the doubling time had become. However, there was also evidence that Professor Whitty did not wish the UK to be the first country to abandon containment and felt it was best to wait until the World Health Organization had accepted that Covid-19 was a pandemic and, therefore, there was an international consensus that containment was not achievable.342 This was the wrong approach, given the extent of the spread of the virus within the UK before the World Health Organization declared Covid-19 to be a pandemic on 11 March. |
| 3.158. | A COBR meeting was convened on the afternoon of 12 March 2020.343 It was chaired by Mr Johnson and attended by Ms Foster and Ms O’Neill, Ms Sturgeon and Mr Drakeford, as well as their health ministers and Chief Medical Officers. Professor Vallance explained that there were an estimated 5,000 to 10,000 cases in the UK and that the UK was approximately four weeks behind Italy.344 A paper prepared for the meeting explained that SAGE had considered a number of “possible social and behavioural interventions to delay the outbreak” (see Table 2).345 Professor Vallance told COBR that the aim of implementing these interventions:
“was not to completely suppress the spread of the disease, not only was this not possible, but it would likely lead to a larger second peak later in the year when the NHS may be under increased pressure. Instead, Government interventions should seek to change the shape of the epicurve, ideally delaying the peak until summer when transmission may be lower (although they noted the scientific basis for this is uncertain) and flattening the peak so as not to completely swamp NHS resources.”346 |
Table 2: Interventions considered by SAGE (presented by the Cabinet Secretariat to COBR on 12 March 2020)
Source: Based on INQ000056209_0003
| 3.159. | The Cabinet Secretariat recommended that COBR agree:
“to implement intervention 1 ([symptomatic] individuals staying at home) now; and interventions 3 and 4 (protection for the most vulnerable groups; and social distancing for the over 70s and those with chronic conditions) in 1–3 weeks’ time”.347 However, even with self-isolation and household isolation being implemented, it was anticipated that, at the peak of the epidemic, demand for NHS beds would outstrip supply by 328,000 beds in England, 37,000 in Scotland and 24,000 in Wales.348 |
| 3.160. | Professor Vallance advised COBR that self-isolation for symptomatic people should be implemented and potentially household isolation.349 He also said that SAGE felt there was a strong argument not to begin household isolation or shielding of vulnerable or elderly people immediately, as:
“[T]here was a risk of starting too early in the epicurve, with people’s resilience subsequently flagging during the peak weeks when it is most important for them to isolate.”350 Professor Vallance also described “a good outcome being that by September 2020 herd immunity would be established”.351 |
| 3.161. | A debate took place at COBR over the timing of interventions. Mr Hancock suggested that the implementation of self-isolation should be delayed until 16 March 2020, due to challenges in providing operational support for NHS 111, the non-emergency NHS helpline.352 |
| 3.162. | Mr Johnson echoed Professor Vallance’s advice and stated that the timing of the implementation of the restrictions was critical, since:
“[T]here were downsides to implementing the interventions too early, but if applied too late the most vulnerable may be exposed to the virus during the peak. The timing of the interventions was therefore key to minimising the number of deaths and it was very important to communicate this to the public. Another objective of the interventions would be to minimise the gap in NHS capacity to respond to the outbreak during the peak weeks.”353 |
| 3.163. | COBR decided that an announcement would be made that day (12 March 2020) advising those with mild Covid-19 symptoms to stay at home for seven days from 13 March, reflecting scientific advice about the duration.354 This was to be advisory rather than legally enforceable since, as Mr Johnson explained, it was thought that advice would be enough and “it would have taken longer to enact the legislation”.355 It was agreed that COBR would revisit whether and when to implement household isolation the following week and that no school closures would be implemented.356 Household isolation and shielding were to be communicated to the public shortly, with an indication that these policies would come in the next few weeks.357 |
| 3.164. | Professor Vallance told COBR that it was still thought possible that delaying the peak would avoid swamping the NHS.358 However, as discussed above, Professors Vallance and Whitty, the Department of Health and Social Care, and 10 Downing Street advisers were aware by this time that NHS modelling indicated a level of deaths and hospitalisations that would, in the absence of stringent interventions, be likely to overwhelm the NHS before the peak was reached in the reasonable worst-case scenario. This was not reflected in the COBR minutes, which stated only that:
“the NHS would not find this crisis easy to deal with and that there was still significant work to be done to increase its capacity to respond”.359 |
| 3.165. | Mr Johnson told the Inquiry that, with hindsight, it was clear from the graphs in the paper presented to COBR that:
“[W]e were at risk of some incoherence. The measures envisaged did not seem to lower the epicurve enough to stop the NHS from being overwhelmed.”360 |
| 3.166. | The decision to advise people with mild Covid-19 symptoms to self-isolate was the first intervention to be implemented as part of the delay phase of the Coronavirus: Action Plan. In the Inquiry’s view, this intervention was too little, too late. |
| 3.167. | COBR also discussed the issue of mass gatherings and decided to keep its policy regarding mass gatherings under review.361 The Scottish Government explained that it was minded to advise against gatherings of more than 500 people to ensure emergency workers could prioritise the Covid-19 response.362 Following the COBR meeting, Ms Sturgeon publicly announced that all gatherings over 500 people in Scotland would be cancelled from 16 March 2020.363 |
| 3.168. | Mr Johnson told the Inquiry that the move from ‘contain’ to ‘delay’ was agreed at this COBR meeting by all four nations.364 While this was not explicitly recorded in the minutes of the meeting, it was implicit in the decision taken by the UK government and devolved administrations to start implementing restrictions to slow the spread of the virus – beginning with self-isolation advice.365 A Northern Ireland Office Situation Report (SitRep) produced on the evening of 12 March 2020 stated that “COBR (M) today took the decision to move from Contain to Delay” and a UK government press release indicated that the decision had been taken that day.366 |
| 3.169. | After the COBR meeting, Mr Johnson and Mr Hancock met with Sir Simon Stevens to discuss “how the NHS would best manage in this situation”.367 Sir Simon Stevens explained that NHS England planned to “free up 30k beds” by “stopping non-urgent operations” and “being more assertive on long stays”.368 NHS England slides were presented to Mr Johnson outlining the potential impact of Covid-19 on the NHS. Mr Shafi explained that these slides demonstrated:
“[I]n a reasonable worst-case scenario with over 80% infected and if no restrictions, with no mitigation, we would need 800,000 beds versus total capacity of 100,000 and the ability to free up 30,000. Even if … measures … were introduced, 200,000 beds would be required … in a more benign scenario with only 20% of the country infected, implementing all the measures … would still lead to a total demand of 100,000 beds at peak.”369 Mr Shafi told the Inquiry that the discussion between Mr Johnson and Sir Simon Stevens focused on how the NHS would best manage this situation and “the conversation did not turn to what the implication of this analysis was” for the government’s plan of slowing the spread.370 |
| 3.170. | The self-isolation advice that COBR had agreed to implement was announced on the evening of 12 March 2020 by the UK government at a 10 Downing Street press conference.371 Mr Johnson explained that delaying the implementation of further restrictions was thought to be necessary: “We have to deploy these at the right time to maximise their effect.”372 |
| 3.171. | Mr Johnson informed the public that the delay phase would now commence and that, from 13 March 2020, people with coronavirus symptoms would be advised to self-isolate at home for at least seven days.373 He explained:
“[W]e have a clear plan that we are now working through. We’re now getting on to the next phase in that plan because this is now not just an attempt to contain the disease as far as possible, but to delay its spread and thereby minimise the suffering … From tomorrow, if you have coronavirus symptoms, however mild, either a new continuous cough or a high temperature, then you should stay at home for at least seven days to protect others and help slow the spread of the disease.”374 Mr Johnson explained that it was likely in the coming weeks that it would be necessary to go further and implement household isolation, so that “if someone in a household has those symptoms, we will be asking everyone in that household to stay at home”.375 Household isolation was ultimately introduced on 16 March 2020. |
| 3.172. | Professor David Halpern, Chief Executive of the Behavioural Insights Team (formerly known as the ‘Nudge Unit’) from 2014, sent an email to Mr Hancock, Sir Christopher Wormald, Professors Vallance and Whitty, and others, expressing his concern at the limitations of SAGE modelling.376 He recommended that there should be concrete advice on general social distancing. Professor Halpern told the Inquiry that he was “puzzled as to why SAGE was not recommending stronger action”.377 |
| 3.173. | Professor Edmunds was also alarmed by the lack of urgency. On 12 March 2020, Sir Jeremy Farrar, Director of the Wellcome Trust from October 2013 to February 2023, asked Professors Edmunds and Ferguson whether they were “comfortable with the plans UKG [UK government] have got in place, the pace of actions and the changes they are making”.378 Professor Edmunds said that he was not:
“1. The data are crap and hopelessly out of date, so we have little situational awareness. The daily figures are a joke and the guestimate of 5–10,000 cases is probably too low. 2. The measures just announced will do very little. Not quite sure just how many cases will escape, but I suspect a fair few. 3. We will have to do a lot more to manage this epidemic. The current plans will overwhelm the NHS almost straight away. We need much more stringent control measures if we want to slow it down. Not necessarily now, but soon. Very soon. 4. There is an obsession with not getting an autumn / winter epidemic later this year. This seems to be the tail wagging the dog. We are going to get a massive epidemic in the summer with hundreds of thousands of deaths.“379 |
The end of community testing and tracing contacts
| 3.174. | Testing is a vital tool in responding to a pandemic, yet the UK government and devolved administrations were forced to abandon community testing at an early stage of the Covid-19 pandemic. At COBR on 12 March 2020, Professor Whitty stated:
“[O]nce the policy of seven day self-isolation was in place the plan would be to stop all testing of people entering into self-isolation and to stop all contact tracing from other geographical areas.”380 |
| 3.175. | That day, the UK government announced that it would stop community testing and contact tracing in order to prioritise testing capacity for healthcare settings.381 Mr Hancock confirmed to the Inquiry that “the problem at this point was that we didn’t have enough tests for community testing”.382 Neither did the devolved administrations. It takes time to increase test and trace capacity. The Inquiry is exploring the approach to testing, tracing and isolation in Module 7: Test, trace and isolate. |
| 3.176. | A similar decision was confirmed in Wales on 13 March 2020.383 Dr Tracey Cooper, Chief Executive of Public Health Wales from June 2014, said that, by 12 or 13 March, Public Health Wales and colleagues across the UK “didn’t have the capacity to cope with all of the contact tracing”.384 By mid-March, the Welsh Government had a lack of testing capacity and confirmed in a public statement on 21 March that “Public Health Wales now has capacity for over 800 tests per day”.385 Dr Goodall confirmed that:
“[I]n hindsight, if testing capacity had been available, I believe that despite the extraordinary ask it would have represented, maintaining a universal contact tracing system may have more positively affected outcomes over the subsequent weeks of the pandemic.”386 |
| 3.177. | In Northern Ireland, testing also ended on 12 March 2020, although this was not the subject of a positive decision nor of any analysis specific to Northern Ireland by the Northern Ireland Executive Committee.387 Professor McBride told the Inquiry that testing capacity at the time was insufficient to identify all cases that needed to be contact traced and that available tests needed to be prioritised for clinical care and settings with vulnerable people. He explained that this:
“in turn impacted the effectiveness of contact tracing, as only a limited proportion of cases in the community were being picked up through testing”.388 Mr Swann explained that, in Northern Ireland: “The decision to pause testing and contact tracing at this stage in mid-March was integrally linked to the decisions to move to the delay phase and to introduce population wide lockdown measures.”389 Mr Pengelly told the Inquiry that the decision to cease testing and tracing in Northern Ireland was: “an issue that flowed from the COBR decision to move nationally from the contain to the delay phase, because there was – the UK-wide plan had been agreed, I think at COBR, a week before, and it included that – it included the point that when we move into the delay phase, the benefits of contact tracing were redundant, it would be stood down”.390 |
| 3.178. | The decision to stop testing was also seen as consistent with the delay phase of the Covid-19 response by Professor Harries. She told colleagues on 13 March 2020 that the decision to stop testing was “a planned change in approach as part of the move from containment to delay”.391 It was seen as unnecessary to continue to test, trace and isolate during the delay phase. The Scottish Government also considered that it was not the best use of its resources to continue to test and trace once containment was no longer possible.392 |
| 3.179. | However, just a few days later, Dr Tedros Adhanom Ghebreyesus, Director-General of the World Health Organization from July 2017, stated: “[W]e have a simple message to all countries – test, test, test.”393 |
| 3.180. | At a 10 Downing Street press conference on 26 March 2020, Professor Harries explained that the World Health Organization guidance was:
“addressing all countries across the world with entirely different health infrastructures and particularly public health infrastructures, we have an extremely well developed public health system in this country and in fact our public health teams actually train others abroad … so the point there is that they are addressing every country including low and middle income countries so encouraging all countries to test of some type”.394 Professor Harries added that, as the UK had moved to the delay phase, testing and contact tracing in the community was now “not an appropriate intervention” – although this would continue in high-risk settings such as care homes.395 In her evidence to the Inquiry, Professor Harries accepted that the World Health Organization advice applied equally to the UK and explained she had intended to communicate that test and trace in the community was no longer an “appropriate intervention” when “the peak of the pandemic rises so quickly that it becomes unmanageable”.396 She confirmed that the decision to stop community testing was based on a need to prioritise the limited number of tests available for use in healthcare settings.397 While Professor Harries did not intend to mislead the public about the reason that test and trace had ended in the community, her statement that it was no longer an “appropriate intervention” had the potential to do so and was therefore unhelpful. Her statement gave rise to a risk that the public might have believed there was a principled reason that test and trace in the community had ended, rather than because there was insufficient testing capacity. |
| 3.181. | The Inquiry is satisfied that the decisions to stop test and trace across the UK reflected a lack of test and trace capacity. The limited remaining capacity was prioritised for hospitals and other healthcare settings. There was inadequate capacity because pandemic planning had focused solely on pandemic influenza, which spreads too quickly for test and trace procedures to be effective. Covid-19 has a longer generation time of six to seven days, which would have made test and trace procedures more viable had greater capacity existed.398 |
| 3.182. | The consequences were dire. Community testing did not recommence in the UK until 18 May 2020.399 Until scientific advisers began to receive data from CHESS from 16 March, the UK government and devolved administrations were left without any effective means of monitoring the spread of Covid-19 in the community.400 However, as outlined in Chapter 4: Realisation and lockdown, in this volume, it was not until late March that CHESS was able to provide a more complete data picture.401 As a result, neither scientific advisers nor decision-makers had robust data on how many infections there were in the community. These data were essential to understanding how quickly NHS capacity might be overwhelmed. |
The situation on 12 March 2020
| 3.183. | The situation by 12 March 2020 was little short of calamitous. The Coronavirus: Action Plan , which had taken three weeks to produce, was significantly out of date at the point of its publication. Containment had failed. Community testing had ceased and the UK government and devolved administrations had no real understanding of the spread of the virus. Any opportunity to get on top of the virus had been lost. |
| 3.184. | Mr Johnson told the Inquiry that “it was clear” by 12 March 2020 “that the UK was going to be badly hit by coronavirus”.402 At the press conference that day, Mr Johnson warned the public:
“[T]he number of cases will rise sharply and indeed the true number of cases is higher – perhaps much higher – than the numbers of cases we have so far confirmed with tests. I’ve got to be clear, we’ve all got to be clear, that this is the worst public health crisis for a generation. Some people compare it to seasonal flu. Alas, that is not right. Owing to the lack of immunity, this disease is more dangerous. And it’s going to spread further and I must level with you, level with the British public, many more families are going to lose loved ones before their time .”403 |
- INQ000223394_0001
- INQ000223394_0001
- ‘CMO for England announces 12 new cases of novel coronavirus: 01 March 2020’, Department of Health and Social
Care, 1 March 2020 (https://www.gov.uk/government/news/cmo-for-england-announces-12-new-cases-of-novel-coronavirus-01-march-2020;
INQ000237298) - ‘Coronavirus (COVID-19) confirmed in Scotland’, Scottish Government, 1 March 2020 (https://www.gov.scot/news/coronavirus-covid-19; INQ000591896)
- ‘Health Secretary sets out government “battle plan” for COVID-19’, Department of Health and Social Care, 1 March
2020 (https://www.gov.uk/government/news/health-secretary-sets-out-government-battle-plan-for-covid-19;
INQ000237297_0003) - ‘Health Secretary sets out government “battle plan” for COVID-19’, Department of Health and Social Care, 1 March
2020 (https://www.gov.uk/government/news/health-secretary-sets-out-government-battle-plan-for-covid-19;
INQ000237297_0004) - ‘Health Secretary sets out government “battle plan” for COVID-19’, Department of Health and Social Care, 1 March
2020 (https://www.gov.uk/government/news/health-secretary-sets-out-government-battle-plan-for-covid-19;
INQ000237297_0003) - INQ000249526_0045 para 141
- INQ000116811_0044-0046 paras 161-168
- INQ000116811_0046 para 168
- INQ000116811_0047 para 169
- INQ000116811_0047 para 169
- INQ000116811_0060 para 222
- INQ000116811_0046-0047 paras 168-169
- Graham Medley 12 October 2023 131/22-132/16
- INQ000061517_0005; INQ000106129_0003
- INQ000151506
- INQ000249526_0045 para 140; INQ000116811_0046 para 168
- INQ000116811_0046-0047 paras 168-169
- INQ000116811_0046 para 168
- INQ000228664; INQ000151506; INQ000233672
- INQ000273841_0015 para 29
- Edward Udny-Lister 7 November 2023 148/23-24
- INQ000065694
- INQ000065694_0003-0004
- Robin Swann 13 May 2024 113/1-18
- Robin Swann 13 May 2024 107/6-17
- INQ000255836_0025 para 111; INQ000056217
- INQ000144792_0033 para 72
- INQ000056217_0005 para 2
- INQ000056217_0005 para 3
- INQ000056217_0005-0007 paras 5-13, decision 2; see also INQ000215035_0024 para 95; Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000391237_0041 para 167
- Mark Drakeford 13 March 2024 72/22-25
- INQ000233559
- INQ000233559_0003
- INQ000591923_0001
- INQ000591923_0001
- INQ000048787. The Covid-19 Core Group met weekly to share information until 14 September 2020. See INQ000371209_0014-0015 para 42.
- INQ000147277_0001
- INQ000103691_0002
- INQ000102697_0005
- INQ000339033_0078 para 210
- INQ000273984_0030 para 132
- Incident Management Team Report Conference Outbreak – March 2020, Public Health Scotland, 5 October 2021, p6 (https://publichealthscotland.scot/media/9575/incident-management-team-report-conference-outbreak-march-2020-oct21-english.pdf;
INQ000147544) - Incident Management Team Report Conference Outbreak – March 2020, Public Health Scotland, 5 October 2021, p27
(https://publichealthscotland.scot/media/9575/incident-management-team-report-conference-outbreak-march-2020-oct21-english.pdf;
INQ000147544) - Incident Management Team Report Conference Outbreak – March 2020, Public Health Scotland, 5 October 2021, p31
(https://publichealthscotland.scot/media/9575/incident-management-team-report-conference-outbreak-march-2020-oct21-english.pdf;
INQ000147544) - INQ000225995_0001; Elizabeth Lloyd 25 January 2024 59/12-24; INQ000273978_0089 para 356; INQ000339033_0078-0079 para 211
- INQ000227479_0001
- INQ000052319
- INQ000119430_0001 para 1
- INQ000119430_0001 para 1; INQ000310090_0002 para 16
- INQ000119430_0001 paras 4-5
- ‘The effect of social distance measures on deaths and peak demand for hospital services in England’, London School of Hygiene & Tropical Medicine, 12 June 2020 [considered at SAGE 3 March 2020] (https://www.gov.uk/government/publications/the-effect-of-social-distance-measures-on-deaths-and-peak-demand-for-hospital-services-in-england-3-march-2020; INQ000212223)
- INQ000474255_0057 para 147; see also INQ000048089_0001-0002
- INQ000052319_0002 para 1
- INQ000056158_0001 para 3
- INQ000056158_0001 para 5
- INQ000056158_0003 para 14
- INQ000119719_0002 paras 4, 6
- INQ000119719_0002 para 7
- INQ000129014_0002
- INQ000129014_0001-0002
- INQ000119430_0001 paras 8-9
- ‘The effect of social distance measures on deaths and peak demand for hospital services in England’, London School of Hygiene & Tropical Medicine, 12 June 2020 [considered at SAGE 3 March 2020], p2 (https://www.gov.uk/government/publications/the-effect-of-social-distance-measures-on-deaths-and-peak-demand-for-hospital-services-in-england-3-march-2020; INQ000212223)
- ‘The effect of social distance measures on deaths and peak demand for hospital services in England’, London School of Hygiene & Tropical Medicine, 12 June 2020 [considered at SAGE 3 March 2020], p2 (https://www.gov.uk/government/publications/the-effect-of-social-distance-measures-on-deaths-and-peak-demand-for-hospital-services-in-england-3-march-2020; INQ000212223)
- INQ000232901_0004 para 19
- ‘Testing expansion’, Scottish Government, 1 May 2020 (https://www.gov.scot/news/testing-expansion; INQ000357884_0003); INQ000273984_0064 para 280
- INQ000189140; INQ000137447_0001
- INQ000232901_0004 para 15
- INQ000056139_0004
- INQ000056139_0004
- INQ000056139_0004
- INQ000056139_0004
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 March 2020’, Prime Minister’s Office and Boris Johnson, 3 March 2020 (https://www.gov.uk/government/speeches/pm-statement-at-coronavirus-press-conference-3-march-2020; INQ000086761_0002)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 March 2020’, Prime Minister’s Office and Boris Johnson, 3 March 2020 (https://www.gov.uk/government/speeches/pm-statement-at-coronavirus-press-conference-3-march-2020; INQ000086761_0003)
- INQ000231042_0009
- INQ000196743_0002
- Boris Johnson 6 December 2023 102/3-10
- INQ000093223_0006
- INQ000048313_0068. The reference to ‘swine flu’ was the 2009 to 2010 H1N1 influenza pandemic.
- INQ000320806_0005; Mark Drakeford 13 March 2024 68/5-13
- INQ000255778_0001
- INQ000255778_0001
- Quentin Sandifer 6 March 2024 54/24-55/3
- Mark Drakeford 13 March 2024 68/5-8
- INQ000273747_0009 para 28; INQ000216456_0002 para 1.1
- INQ000227479_0001
- For example, the discussion of Covid-19 at the previous Cabinet meeting on 25 February 2020 had taken place
under “any other business” (INQ000238705_0009 para 44). - INQ000232901_0006 para 20
- INQ000145786_0004 para 5
- INQ000145786_0006 para 13
- INQ000145786_0004 para 8
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380); INQ000106107; Matt Hancock 30 November 2023 111/17-18
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p10, para 3.9 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000251645_0077-0078 para 7.43; Christopher Whitty 21 November 2023 124/5-7; INQ000255836_0024 para 104; INQ000146569
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, pp6, 13, paras 2.9, 4.13 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- John Edmunds 19 October 2023 46/23-47/8
- For a detailed explanation of the scientific concept of population immunity, see INQ000252450_0016-0018 paras 2.33-2.38; INQ000238826_0073 para 233; INQ000251645_0106-0108 paras 7.144-7.149.
- INQ000251645_0108 para 7.148
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, pp10, 18, paras 3.9, 4.45 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000238826_0073, 0079 paras 233, 244; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0004-0005, 0008); INQ000056221_0005 para 2; INQ000056217_0005 para 2; INQ000255836_0040 para 168; INQ000252711_0006 para 25; INQ000215035_0011 para 43
- INQ000255836_0039 para 165
- INQ000056219_0007 para 8; see also INQ000056221_0005 para 2
- INQ000056221_0005 para 2
- INQ000056221_0005 para 2
- INQ000548398
- ‘The government’s herd immunity plan is callous and dangerous’, The Guardian, 15 March 2020 (https://www.theguardian.com/world/2020/mar/15/the-governments-herd-immunity-plan-is-callous-and-dangerous; INQ000625218)
- INQ000548398
- INQ000255836_0040 para 170; INQ000232194_0089 para 370; INQ000251645_0083, 0104 paras 7.63, 7.135; INQ000238826_0048, 0062 paras 144, 193
- Dominic Cummings 31 October 2023 192/11-193/3; INQ000237819_0008-0009 para 21; INQ000269182_0030 para 103; see also INQ000279901
- Mark Sedwill 8 November 2023 76/14-19. This is akin to population segmentation strategies subsequently proposed by some scientists, for example in the Great Barrington Declaration published in October 2020. This is discussed further in Chapter 6: The second wave, in this volume.
- INQ000255836_0043 para 178
- INQ000255836_0043 para 178
- Mark Sedwill 8 November 2023 75/16-24
- Mark Sedwill 8 November 2023 81/12-17
- INQ000269182_0029 para 99
- Imran Shaf i 30 October 2023 143/8-15, 144/8-10
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, para 2.21 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, para 2.12 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708); see also Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 4 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, p28 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, pp36-37 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- Christopher Wormald 2 November 2023 108/10-11
- Imran Shaf i 30 October 2023 143/8-15, 144/8-10
- INQ000048399_0005
- Mark Sedwill 8 November 2023 55/18-21
- INQ000252711_0006 para 26
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.42 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000119430_0001 para 9; ‘The effect of social distance measures on deaths and peak demand for hospital services in England’,
London School of Hygiene & Tropical Medicine, 12 June 2020 [considered at SAGE 3 March 2020], p2 (https://www.gov.uk/government/publications/the-effect-of-social-distance-measures-on-deaths-and-peak-demand-for-hospital-services-in-england-3-march-2020; INQ000212223_0002); INQ000151558_0003; INQ000056221_0005 para 2; INQ000064580_0002-0003; INQ000048399_0003; INQ000236391_0002 para 24 - Christopher Whitty 21 November 2023 212/10-25, 213/1-3, 214/21-25
- Lee Cain 31 October 2023 23/3-6; see also INQ000273872_0034
- INQ000056221_0005 para 2
- INQ000238826_0074 para 236; INQ000280628_0053 para 99; Boris Johnson 6 December 2023 110/15-20; INQ000048399_0003; INQ000102697_0019-0020
- INQ000056221_0005 para 2
- ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0002)
- INQ000064580_0003; INQ000231021_0002
- INQ000238826_0074 para 236
- INQ000273841_0031 para 59; Edward Udny-Lister 7 November 2023 160/25-161/1-2; INQ000251645_0110 para 7.159
- INQ000251645_0110 para 7.159
- INQ000273841_0031 para 59
- Edward Udny-Lister 7 November 2023 160/25-161/1-2
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, pp10, 15, 18, paras 3.9, 4.26, 4.42 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380); INQ000056221_0005 para 2; Boris Johnson 6 December 2023 110/13-15; ‘UK Prime Minister Boris Johnson holds a press conference on
coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0003); INQ000232901_0004 para 16 - Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.46 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380); INQ000056221_0005 para 2; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0002)
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p15, para 4.26 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.44 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.45 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, pp14, 18, paras 4.25, 4.45 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000056217_0005 para 3
- Matt Hancock 30 November 2023 138/1-2
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.44 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000056217_0005 para 3
- Christopher Whitty 22 November 2023 26/20-23; INQ000255836_0022 paras 88-89; INQ000056219_0005 para 6; ‘Watch again: Boris Johnson says government is moving towards “delay phase” of coronavirus’, YouTube, 9 March 2020 (https://www.youtube.com/watch?v=Yc1alOEjDVA; INQ000223088_0004-0005); INQ000273807_0057-0058 para 7.65; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0002-0004)
- INQ000056219_0005 para 6; ‘Watch again: Boris Johnson says government is moving towards “delay phase” of coronavirus’, YouTube, 9 March 2020 (https://www.youtube.com/watch?v=Yc1alOEjDVA; INQ000223088_0004-0005); INQ000273807_0057-0058 para 7.65
- ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0003-0004)
- INQ000146571_0001
- INQ000236391_0003 paras 29-30; INQ000146572_0001
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p17, para 4.36 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, p27, para 3.13 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708)
- INQ000106107; Matt Hancock 30 November 2023 111/17-18
- INQ000251645_0083 para 7.62
- INQ000056217_0005 para 5
- INQ000238826_0059 para 178; Christopher Whitty 21 November 2023 199/16-20; Neil Ferguson 17 October 2023 121/8-10
- Michael McBride 10 May 2024 48/11-22; INQ000421704_0127, 0245 paras 283, 539
- INQ000298975_0004; ‘Written Statement: Coronavirus (COVID-19) Action Plan’, Vaughan Gething, Minister for Health and Social Services, Welsh Government, 3 March 2020 (https://www.gov.wales/written-statement-coronavirus-covid-19-action-plan; INQ000066062_0001); INQ000273747_0009 para 27; see also Michael Gove 28 November 2023 53/2-5
- INQ000273747_0009 para 27
- INQ000238822_0002-0004 paras 12-15
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3
March 2020, p11, para 4.5 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380) - UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011, p15 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf; INQ000022708); see also Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 4 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- Christopher Whitty 21 November 2023 198/20-23; see also Frank Atherton 4 March 2024 35/24-25; Vaughan
Gething 11 March 2024 77/12-17 - Patrick Vallance 20 November 2023 52/14-16
- Report 8: 11th June 2020 – COVID-19 Genomics UK (COG-UK) Consortium, COVID-19 Genomics UK (COG-UK) Consortium, 12 June 2020 (https://webarchive.nationalarchives.gov.uk/ukgwa/20201203114610/https://www.cogconsortium.uk/news_item/report-8-11th-june-2020-covid-19-genomics-uk-cog-uk-consortium; INQ000230987); INQ000238826_0195 para 594
- INQ000252711_0007 para 30; Lee Cain 31 October 2023 16/10-12
- INQ000269182_0018 para 62
- INQ000269182_0018 para 62; INQ000195879
- INQ000273841_0016 para 30
- INQ000279883_0002
- ‘Public information campaign focuses on handwashing’, Department of Health and Social Care, 4 March 2020 (https://www.gov.uk/government/news/public-information-campaign-focuses-on-handwashing; INQ000618208)
- INQ000056218_0001-0003
- INQ000056158_0003 para 3
- INQ000056158
- INQ000056158_0003 para 14
- INQ000056218
- INQ000056158_0003 para 6
- INQ000056158_0003 para 7
- INQ000056218_0008 para 17
- INQ000056218_0009 para 19
- INQ000056218_0008 para 18
- INQ000056218_0011 para 10
- INQ000425601
- INQ000352956_0001-0010; INQ000352955_0001-0013; INQ000352957_0001-0008
- INQ000258367_0002
- INQ000309229_0003
- INQ000309229_0003
- INQ000103631_0001 para 1; INQ000421704_0125 para 279
- INQ000218494_0002
- INQ000398439_0001 para 4
- INQ000216456_0004 para 3.4
- INQ000216456_0004 para 3.5
- INQ000216456_0004 para 5.2
- INQ000281647_0001
- ‘CMO for England announces first death of patient with COVID-19’, Department of Health and Social Care, 5 March 2020 (https://www.gov.uk/government/news/cmo-for-england-announces-first-death-of-patient-with-covid-19; INQ000237343)
- ‘CMO for England announces 25 new cases of coronavirus (COVID-19): 5 March 2020’, Department of Health and Social Care, 5 March 2020 (https://www.gov.uk/government/news/cmo-for-england-announces-25-new-cases-of-coronavirus-covid-19-5-march-2020; INQ000237341)
- INQ000183959_0003
- INQ000216492_0002
- INQ000391237_0045 para 180
- INQ000106152_0002 paras 2-3
- INQ000119719_0002 para 7; INQ000106152_0002 para 14
- INQ000106152_0002 paras 1, 6
- INQ000047950_0001
- INQ000249526_0061-0062 para 200
- INQ000056179_0001-0002
- INQ000151558_0003
- INQ000087540_0004 para 2.6
- INQ000087540_0004 paras 2.7-2.9
- INQ000252311; INQ000252096; INQ000252095. Dr Orford’s updates to the Chief Medical Officer for Wales became labelled as Technical Advisory Cell updates from 2 March 2020. See INQ000390618_0032, 0039 paras 92, 115. The cell was established during the pandemic to provide coordination of scientific and technical advice to support Welsh Government decision-makers during emergencies – see Chapter 9: Scientific and technical advice, in Volume II.
- INQ000252311_0001 point 4
- INQ000252311_0008
- Andrew Goodall 5 March 2024 57/13-21
- INQ000255779; INQ000049539
- INQ000049539_0001 para 3.a
- INQ000292536_0002 para 14
- INQ000339033_0077 para 207
- INQ000292579_0001-0002
- ‘First death of patient from Coronavirus (COVID-19)’, Scottish Government, 13 March 2020 (https://www.gov.scot/news/first-death-of-patient-from-coronavirus-covid-19; INQ000357783_0002)
- INQ000049540_0003
- ‘Coronavirus: Northern Italy quarantines 16 million people’, BBC News, 8 March 2020 (https://www.bbc.co.uk/news/world-middle-east-51787238;
INQ000591899); ‘Coronavirus: Italy extends emergency measures nationwide’, BBC News, 10 March 2020 (https://www.bbc.co.uk/news/world-europe-51810673; INQ000573840) - INQ000049540_0008
- INQ000273553_0045-0047 para 8.13. S-COVER was a respiratory intensive care network under which, from 29 February 2020, 11 pilot trusts were asked to submit samples from adult patients admitted to intensive care with an acute community-acquired respiratory infection (see INQ000251906_0168 para 724). (This was later replaced by the COVID-19 Hospitalisation in England Surveillance System, known as CHESS.) In addition, the Royal College of General Practitioners’ sentinel surveillance system tested a random sample of patients attending GP practices for acute respiratory illness (see INQ000273553_0045-0047 para 8.13). This was added to Public Health England’s First Few Hundred or FF100 datasets.
- INQ000273553_0045-0047 para 8.13
- INQ000273553_0045-0047 para 8.13
- INQ000273553_0045-0047 para 8.13
- INQ000273841_0030 para 56; INQ000285993
- INQ000146571_0001
- INQ000146571_0001
- Steven Riley 17 October 2023 28/11-30/14; INQ000269365
- INQ000269365_0001
- This was not recorded in the minutes of the meeting (INQ000183959_0003), but was set out in a note taken by the Welsh Government at the meeting (INQ000216492_0001).
- INQ000391237_0045 para 180
- INQ000047950_0001
- INQ000232901_0004 para 15
- INQ000255049_0001
- INQ000255049_0001
- INQ000056219
- INQ000280628_0049 para 92
- INQ000056190_0001
- INQ000056190_0003
- INQ000056179_0001; INQ000056178_0002
- INQ000056179_0002
- INQ000056179_0002
- INQ000056219_0005 paras 4-5
- INQ000056219_0005 para 4
- INQ000056179_0001. This included high-level analysis of the likely societal and economic impacts of Covid-19 and interventions that had been collated by the Cabinet Office (as discussed above).
- INQ000056219_0005-0006 para 7
- INQ000056219_0007 para 8
- INQ000056219_0005-0006 paras 6, 8
- INQ000056219_0005 para 6; see also INQ000056221_0005 para 4
- INQ000056219_0010
- INQ000056219_0010; INQ000056179_0005; see also ‘Watch again: Boris Johnson says government is moving towards “delay phase” of coronavirus’, YouTube, 9 March 2020 (https://www.youtube.com/watch?v=Yc1alOEjDVA; INQ000223088_0014)
- INQ000216493; INQ000273747_0011-0012 para 33
- INQ000056219_0007 para 9
- INQ000129909_0002 para 2.1
- INQ000433481_0002 action 1
- Richard Pengelly 7 May 2024 55/5-60/5
- INQ000109125
- INQ000109125_0002 paras 5-6; INQ000249526_0083 para 255
- INQ000249526_0084-0085 para 262
- INQ000249526_0063 para 206
- INQ000196055; INQ000149009
- INQ000196055_0002
- Neil Ferguson 17 October 2023 191/21-192/2
- ‘Cheltenham Festival 2020: Race schedule and BBC radio coverage times’, BBC Sport, 4 March 2020 (https://www.bbc.co.uk/sport/horse-racing/51592290;
INQ000591894) - ‘Champions League: Atletico score three as Liverpool knocked out – reaction’, BBC Sport, 11 March 2020 (https://www.bbc.co.uk/sport/live/football/51468477; INQ000591893)
- INQ000109125_0004 para 37
- INQ000151575_0003
- INQ000146572_0001
- INQ000056158
- INQ000255836_0031 para 130
- INQ000183880_0002; INQ000255836_0029 para 129
- INQ000255836_0031 para 130
- INQ000263380
- INQ000536350_0014-0015 paras 65-70
- INQ000259848_0018-0019 para 31
- INQ000238706_0003 para 10
- INQ000238706_0003 para 10
- INQ000238706_0003 para 9
- INQ000238706_0004 para 15(a)
- INQ000238706_0004 para 15(d)
- INQ000425540_0004
- INQ000065695_0001
- INQ000065695_0002
- INQ000065695_0002-0003
- Robin Swann 13 May 2024 121/2-24
- INQ000282777_0003
- ‘WHO Director-General’s opening remarks at the media briefing on COVID-19 – 16 March 2020’, World Health Organization, 16 March 2020 (https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefingon-covid-19—16-march-2020; INQ000237407)
- ‘WHO Director-General’s opening remarks at the media briefing on COVID-19 – 20 March 2020’, World Health Organization, 20 March 2020 (https://www.who.int/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—20-march-2020; INQ000052458_0001)
- INQ000048039_0001
- INQ000102697_0017
- INQ000102697_0017
- INQ000056132_0006
- INQ000056132_0004
- INQ000273747_0013 para 35
- INQ000147246_0002 para 1; INQ000267867_0014 para 56
- INQ000147246_0005 para 2
- INQ000147246_0006
- INQ000119666; INQ000251906_0169-0179 paras 727-730
- INQ000269367; see also INQ000269365; INQ000233674_0001 para 5
- INQ000269367_0004
- INQ000233674_0001 para 6
- INQ000273553_0059 para 9.8
- INQ000195883_0001
- INQ000195883_0001
- INQ000271613_0002
- INQ000215171 para 9
- INQ000056220_0001-0003, 0007 para 12
- INQ000056192_0001, 0006
- INQ000056220_0005 para 1
- INQ000056220_0008 para 15
- INQ000056220_0008 para 15
- INQ000056220_0009 para 10
- INQ000056220_0007 para 12
- INQ000263372_0015 para 44
- INQ000056208_0001-0002 para 6; INQ000056180_0003
- INQ000056208_0003-0004 para 17; see Coronavirus Act 2020, sections 48, 49 and Schedules 18, 19 (https://www.legislation.gov.uk/ukpga/2020/7/contents); Public Health (Control of Disease) Act 1984, section 45C (https://www.legislation.gov.uk/ukpga/1984/22/contents)
- Mark Drakeford 13 March 2024 38/20-40/20
- ‘PM and Deputy CMO on Coronavirus’, Facebook, 11 March 2020 (https://www.facebook.com/borisjohnson/videos/pm-and-deputy-cmo-on-coronavirus/227850301597915; INQ000548399)
- INQ000083097_0002
- Michelle O’Neill 14 May 2024 90/8-11
- INQ000232525_0001
- INQ000232525_0002
- INQ000289859_0001
- INQ000083098_0002
- INQ000083098_0003
- INQ000339033_0010 para 23
- INQ000339033_0072-0074 paras 194-197
- INQ000339033_0010 para 23
- INQ000048313_0022-0023
- INQ000214048_0002
- INQ000214048_0001
- ‘COVID-19: Government announces moving out of contain phase and into delay’, Department of Health and Social Care, 12 March 2020
(https://www.gov.uk/government/news/covid-19-government-announces-moving-out-of-contain-phase-and-into-delay; INQ000052485_0002) - INQ000251645_0091 para 7.94
- INQ000061522_0003 para 5
- Christopher Whitty 21 November 2023 207/4-208/4; INQ000236382_0002; Neil Ferguson 17 October 2023 158/6-160/1
- INQ000056221
- INQ000056221_0005 para 1
- INQ000056209_0001
- INQ000056221_0005 para 2
- INQ000056209_0002
- INQ000056209_0006. No figures were provided for Northern Ireland.
- INQ000056221_0005 para 3
- INQ000056221_0005 para 4
- INQ000056221_0005 para 2; see also INQ000273747_0014 para 37; INQ000280628_0053 para 99
- INQ000056221_0007 para 10
- INQ000056221_0007 para 8
- INQ000056221_0008 para 14
- INQ000255836_0036 para 149
- INQ000056221_0010 paras 3, 6
- INQ000056221_0008 para 15; INQ000255836_0037 para 154; INQ000412903_0026 para 67
- INQ000056221_0005 para 2
- INQ000056221_0006
- INQ000255836_0036 para 150
- INQ000056221_0010
- INQ000056221_0006
- ‘First Minister announces large events to be cancelled’, Scottish Government, 12 March 2020 (https://www.gov.scot/news/first-minister-announces-large-events-to-be-cancelled; INQ000249326)
- INQ000255836_0037 para 154; INQ000056221; INQ000421704_0040 para 94; INQ000391237_0048-0049 para 196; INQ000339033_0070 para 188
- ‘COVID-19: Government announces moving out of contain phase and into delay’, Department of Health and Social Care, 12 March 2020 (https://www.gov.uk/government/news/covid-19-government-announces-moving-out-of-contain-phase-and-into-delay; INQ000052485)
- INQ000083097_0002; ‘COVID-19: Government announces moving out of contain phase and into delay’, Department of Health and Social Care, 12 March 2020 (https://www.gov.uk/government/news/covid-19-government-announces-moving-out-of-contain-phase-and-into-delay; INQ000052485)
- INQ000215035_0014 para 56; INQ000146636_0054
- INQ000146639_0001
- INQ000215035_0014 para 56
- INQ000215035_0014 para 56
- ‘COVID-19: Government announces moving out of contain phase and into delay’, Department of Health and Social Care, 12 March 2020 (https://www.gov.uk/government/news/covid-19-government-announces-moving-out-of-contain-phase-and-into-delay; INQ000052485); INQ000255836_0038 para 159; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0001)
- ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0001)
- ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0001); ‘Prime Minister’s statement on coronavirus (COVID-19): 12 March 2020’, Prime Minister’s Office and Boris Johnson, 12 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-12-march-2020; INQ000086751_0002-0003); INQ000255836_0038 para 159
- ‘Prime Minister’s statement on coronavirus (COVID-19): 12 March 2020’, Prime Minister’s Office and Boris Johnson, 12 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-12-march-2020; INQ000086751_0002-0003)
- ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0001)
- INQ000129046
- INQ000188738_0015 para 70
- INQ000212037_0002
- INQ000212037_0001
- INQ000056221_0007-0008 para 12
- INQ000109142_0004 para 33; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0003)
- Matt Hancock 30 November 2023 152/2-3
- INQ000267867_0012 para 50; INQ000147243_0001-0002
- Tracey Cooper 5 March 2024 187/18-20
- ‘Written Statement: Coronavirus (COVID-19) – update’, Vaughan Gething, Minister for Health and Social Services, Welsh Government, 21 March 2020 (https://www.gov.wales/written-statement-coronavirus-covid-19-update; INQ000509418)
- INQ000396878_0085 para 332
- Arlene Foster 15 May 2024 69/4-7; INQ000452486_0016 para 50; Richard Pengelly 7 May 2024 91/8-11
- INQ000421704_0137-0138 para 298; see also INQ000426790_0001; INQ000065689_0031
- INQ000412903_0027-0028 para 72
- Richard Pengelly 7 May 2024 89/19-25
- INQ000151587_0001
- INQ000273984_0029 para 124
- ‘WHO head: “Our key message is: test, test, test!”’, BBC News, 16 March 2020 (https://www.bbc.co.uk/news/av/world-51916707; INQ000625219); INQ000625220
- INQ000273807_0145 para 10.18; INQ000587693_0002
- INQ000273807_0145-0146 para 10.18; INQ000587693_0002
- Jenny Harries 28 November 2023 246/11-15
- INQ000273807_0146 paras 10.19-10.20; Jenny Harries 28 November 2023 244/8-15; see also INQ000236391_0003 para 33
- INQ000051883_0002 para 11
- ‘Everyone in the United Kingdom with symptoms now eligible for coronavirus tests’, Department of Health and Social Care, 18 May 2020 (https://www.gov.uk/government/news/everyone-in-the-united-kingdom-with-symptoms-now-eligible-for-coronavirustests; INQ000497453); INQ000232194_0097-0098 para 401
- INQ000249526_0081 para 250
- INQ000249526_0081 para 253
- INQ000255836_0038 para 158
- ‘Prime Minister’s statement on coronavirus (COVID-19): 12 March 2020’, Prime Minister’s Office and Boris
Johnson, 12 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-12-march-2020; INQ000086751_0002); ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0001); INQ000255836_0038 paras 158-159
Chapter 4: Realisation and lockdown (13 to 23 March 2020)
Introduction
| 4.1. | The decision to announce a mandatory lockdown across the UK on 23 March 2020 was one of the gravest decisions that any government in the UK has had to make. Such intensive and widespread measures had not been adopted in Western Europe for more than a century.1 Similar decisions had already been taken across the world, including in Wuhan, China on 23 January 2020, in Italy on 9 March following regional measures across Lombardy and 14 northern provinces on 8 March, in France on 17 March and in large swathes of other parts of Europe.2 More than 100 countries had instituted a full or partial lockdown by the end of March.3 |
| 4.2. | Prior to mid-March 2020, it was considered “inconceivable” that such a step would be taken in the UK.4 This chapter examines the events that led to the UK government and devolved administrations finding themselves with no option but to contemplate the previously inconceivable. |
Public health data and NHS capacity at 13 March 2020
| 4.3. | By 13 March 2020, the UK government and the devolved administrations had moved to the ‘delay’ phase of their responses. They had stopped community testing and implemented the first restriction – the advice to self-isolate – with the objective of flattening the peak of infections to reduce the pressure on their healthcare systems. Time was quickly running out to prevent NHS capacity in England being overwhelmed. This would become apparent to decision-makers and their advisers in the following days. Professor Neil Ferguson, Mathematical Epidemiologist at Imperial College London, described 13 March 2020 as “pivotal in determining policy over the next 10 days”.5 |
| 4.4. | As noted in Chapter 3: The first 12 days of March 2020, in this volume, papers provided to COBR on 4 and 12 March made clear that, in the reasonable worst-case scenario, the NHS would be overwhelmed before the peak of the virus was reached.6 |
| 4.5. | Boris Johnson MP (Prime Minister from July 2019 to September 2022) and Matt Hancock MP (Secretary of State for Health and Social Care from July 2018 to June 2021) had also been told by NHS England on 12 March 2020 that, in the reasonable worst-case scenario and if no restrictions were put in place, it would “need 800,000 beds”. This considerably exceeded the “total capacity of 100,000 and the ability to free up 30,000″.7 Even if restrictions were introduced, 200,000 beds would be required and there would be a demand of 100,000 beds at peak.8 The same applied to the devolved administrations, with demand vastly outstripping the number of beds available.9 |
| 4.6. | NHS England had been placed on a Level 4 Major Incident emergency footing (on 30 January 2020) and discussions were taking place about discharge of patients and cancellation of elective treatments to increase NHS capacity. On 13 March 2020, Sir Simon Stevens (later Lord Stevens of Birmingham), Chief Executive of NHS England from April 2014 to July 2021, telephoned Mr Hancock. He proposed postponing all non-urgent operations from 15 April 2020 to free up 30,000 beds and that:
“frail, elderly patients who did not need urgent treatment would need to be discharged, either to their home or care homes”.10 |
| 4.7. | However, up-to-date data on NHS England capacity were still not readily available to decision-makers in mid-March 2020. Mr Johnson told the Inquiry that he:
“could not believe that in the first few weeks the NHS did not even know how many beds there were in the whole organisation”.11 |
| 4.8. | Dominic Cummings, Adviser to the Prime Minister from July 2019 to November 2020, described the data system for NHS updates to Mr Johnson as “me dragging the whiteboard in and scribbling tables” as Sir Simon Stevens spoke. Mr Cummings said that there were not “any real time data”.12 |
| 4.9. | According to Lord Stevens, statistics on bed availability were published from 2000.13 However, NHS England bed availability was recorded as statistics on a weekly basis, rather than as real-time data.14 Lord Stevens recognised that, before the second half of March 2020, “it was not possible automatically to ‘pipe’ real time information on patient case mix and capacity” due to the nature of records and systems available. He attributed this to NHS England proposals to invest in more modern systems being “repeatedly rejected or scaled back” and noted that the lack of immediate access to data therefore “should not have come as a surprise to ministers”.15 Data from the new NHS Covid Situation Report (SitRep) system became available on 16 March.16 Professor Ferguson described this as a system “for monitoring COVID-19 related healthcare demand”.17 From this point, NHS England began to provide data on bed occupancy and availability, the number of ventilated beds available and occupied, hospital capacity, staffing numbers and deaths.18 |
| 4.10. | The devolved administrations also faced problems with real-time NHS data. Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, considered that there was generally a better understanding of hospital capacity in Scotland than in England, due to Scotland’s well-developed electronic health data system.19 However, Professor Andrew Morris (Professor of Medicine at the University of Edinburgh and Chair of the Scottish Government Covid-19 Advisory Group) noted that, at the start of the pandemic, Scotland was still “in the foothills” of being able to use healthcare data in a sufficiently agile and real-time way for rapid analysis generation of insights to inform decision-making, including difficulties with access to primary care data.20 |
| 4.11. | On 5 March 2020, Dr Andrew Goodall (Director General of Health and Social Services in the Welsh Government and Chief Executive of NHS Wales from June 2014 to November 2021) wrote to all Chief Executives of local health boards in Wales. He asked hospitals to review their critical care and high dependency capacity and consider how this could be increased.21 On 13 March, Vaughan Gething MS, Minister for Health and Social Services in the Welsh Government from May 2016 to May 2021, announced a “framework of actions, within which local health and social care providers can make decisions“.22 The framework “switched off” large parts of the health service in Wales, including allowing the suspension of non-urgent work.23 In an update to the Permanent Secretary to the Welsh Government on 13 May, Dr Goodall confirmed that, as a result of modelling for NHS Wales by mid-March, which projected a necessity for 900 critical care and an additional 10,000 system-wide beds at the point of peak demand (which was anticipated to be over the next three to four weeks), “critical care beds were more than doubled from a normal level of 156 beds to over 400“.24 By 3 April 2020, there were 353 critical care beds.25 However, by 20 March, the Technical Advisory Cell (which coordinated scientific and technical advice to the Welsh Government) confirmed:
“[T]here has not been a complete set of accurate data from all Health Boards that describes both ICU [intensive care unit] or Hospitalisations from COVID-19.”26 This meant that: “TAC [the Technical Advisory Cell] is currently not being provided with the data it needs to effectively provide timely and accurate advice.”27 When these data were initially collated, it was “done by phone using an Excel Spreadsheet“.28 |
| 4.12. | Professor Sir Michael McBride, Chief Medical Officer for Northern Ireland from September 2006, observed that, at the outset of the pandemic, there was:
“more limited ICU capacity in NI [Northern Ireland] than in some other parts of the UK and Europe per head of the population. On 1 March 2020 there were 88 critical care beds in NI.”29 |
| 4.13. | The Department of Health (Northern Ireland) announced on 13 March 2020 that health service activity would have to be significantly curtailed as resources needed to be diverted to care for Covid-19 patients. Affected services included non-urgent outpatient appointments, day cases and inpatient and diagnostic work.30 The process of scaling back provision was phased in over days and weeks.31 As this announcement was made prior to the Northern Ireland Executive Committee’s meeting on 16 March, there can have been no advance scrutiny or examination of the decision to curtail health services by it. It was not until the end of April 2020 that reliable data on hospital admissions in Northern Ireland became available.32 The delay in these data becoming available was the result of Northern Ireland “relying largely on [a] paper-based records system“.33 |
| 4.14. | During a pandemic, real-time and accurate knowledge of data relating to NHS bed capacity and patient case mix (the mix of adult, paediatric and neonatal general and acute beds), bed occupancy and admissions is vital to understanding whether interventions may be required to prevent hospitals being overrun. Each of the four governments faced its own lack of real-time health data in mid-March 2020, which reflected a lack of planning by the UK government, Scottish Government, Welsh Government and the Department of Health (Northern Ireland). |
13 March 2020: New data and a dawning realisation
Figure 6: Daily confirmed cases from 2 March to 23 March 2020 across the UK
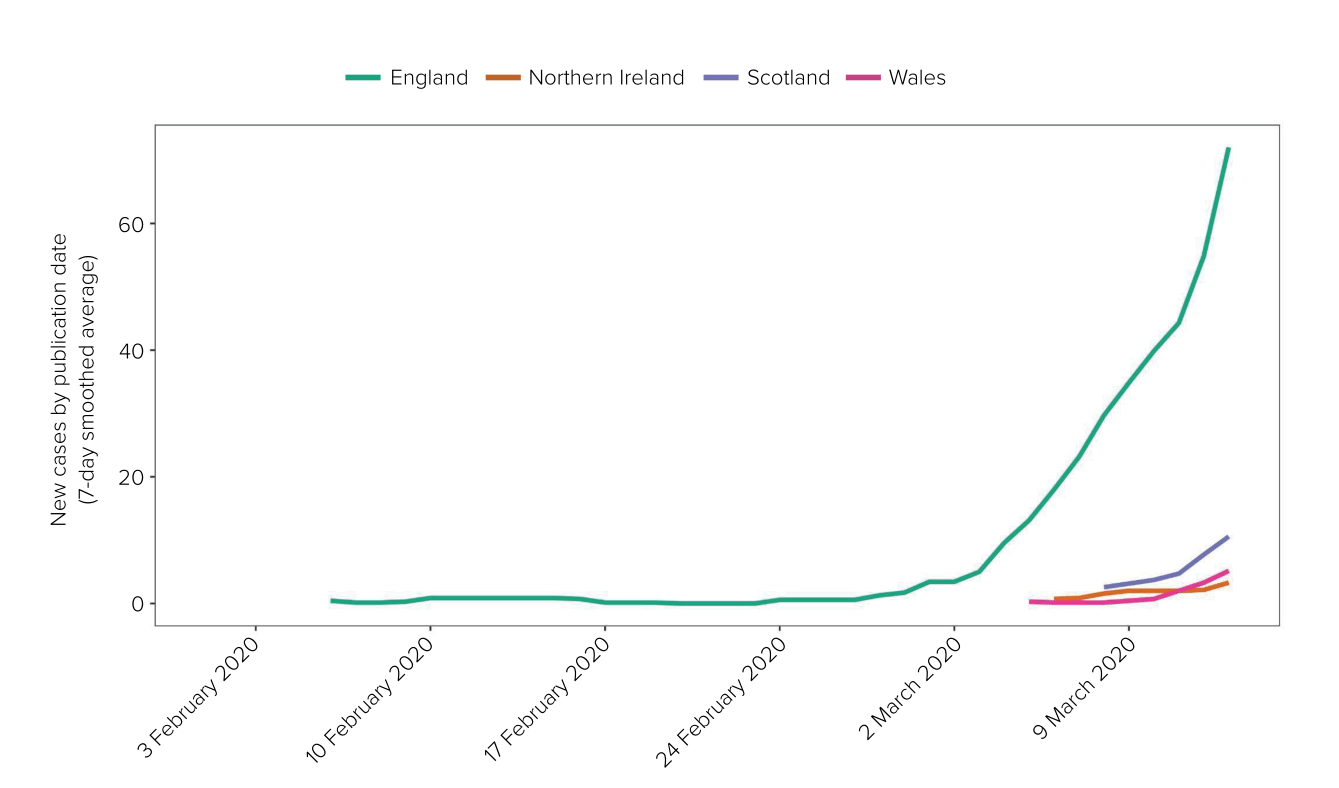
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 4.15. | On 13 March 2020, the Scientific Advisory Group for Emergencies (SAGE) stated:
“Owing to a 5-7 day lag in data provision for modelling, SAGE now believes there are more cases in the UK than SAGE previously expected at this point.”34 |
| 4.16. | Data on the spread of the virus had been commissioned in late February 2020.35 By mid-March 2020, some of these data had become available but the data received were “very difficult to analyse“.36 Professor John Edmunds, Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine and a participant in the Scientific Pandemic Infections Group on Modelling (SPI-M), told the Inquiry:
“[T]he delays between onset in cases to confirmation and entry onto the database were long, at about 5-7 days, but with a very long tail so that some cases were taking up to 3 weeks to be recorded … new cases registered on a given day were actually reflecting infections that might have occurred two weeks earlier … we were estimating that there were hundreds or perhaps thousands of cases occurring every day.”37 Professor Edmunds explained: “[The] data revealed that there were significant delays to confirmation and reporting of cases and that the scale of the epidemic was far larger than was being reported. Both of these had serious implications for the accuracy of the information being portrayed to decision-makers and the public (and even other SAGE members).“38 |
| 4.17. | The SAGE meeting of 13 March 2020 was “sometimes tense and heated“, in part because “unease came to a head about the logistical, political and ethical feasibility of a mitigation strategy which would overwhelm NHS capacity“.39 Professor Ferguson asked NHS England representatives:
“whether there was any way the NHS could cope with the numbers of hospitalisations being envisaged under any of the mitigation scenarios previously reviewed by SAGE, even allowing for surging general bed and ICU capacity. This question got a very clear ‘No’ in response, which was the first time NHSE [NHS England] had stated this at any SAGE meeting.”40 |
| 4.18. | As Professor McBride explained, “We realised we were further into the pandemic than we knew … That caused significant concern.“41 Professor Vallance told the Inquiry that this information “unambiguously showed that the pandemic was far more widespread and far bigger and moving faster than we had anticipated“, which was “extremely worrying“. He explained that, in light of this, “it was my view that we were in a position now where we had to move quickly” and introduce “much more stringent measures“.42 |
| 4.19. | Professor Dame Angela McLean (Chief Scientific Adviser to the Ministry of Defence from 2019 to 2023 and Government Chief Scientific Adviser from April 2023) described the analysis which showed that “ICU capacity was way below that which would be required if there was a wave of infections” as a “real wake-up call“.43 |
| 4.20. | This realisation came too late. It was almost two months after Covid-19 had emerged, and 10 days after NHS England modelling had been presented to SAGE, which established that:
“under a RWC [reasonable worst-case] scenario, the NHS would be unable to meet all demands placed on it, with demand on beds being likely to overtake supply well before the peak was reached“.44 |
| 4.21. | In a discussion on what could be done to limit the spread, most likely in response to the comments that had been made in the preceding days by Professor (later Sir) Christopher Whitty, (Chief Medical Officer for England from October 2019), and Professor Vallance about the risk of ‘behavioural fatigue’, SAGE emphasised:
“[D]ifficulty maintaining behaviours should not … be taken as a reason to delay implementation where that is indicated epidemiologically.”45 |
| 4.22. | However, SAGE recorded that there was a real concern that the restrictions proposed – self-isolation, household isolation and social distancing – would not reduce NHS demand enough and that they might need to be coupled with more intensive actions to enable the NHS to cope.46 It therefore requested that the Scientific Pandemic Infections Group on Modelling, Operational sub-group (SPI-M-O) “investigate what kinds of interventions might be sporadically or continuously implemented to enable the NHS to meet demand“.47 SAGE reiterated that measures that sought to completely suppress the spread of Covid-19 would cause a second peak.48 On the morning of 13 March 2020, Professor Vallance had publicly voiced similar concerns about the use of stringent measures, explaining in a media interview:
“[I]f you suppress something very, very hard. When you release those measures, it bounces back and it bounces back at the wrong time.”49 |
| 4.23. | SAGE’s advice on mass gatherings also began to shift at this meeting as organisers continued to take matters into their own hands and cancel events. It advised:
“Supporting social distancing measures that are taking place anyway (e.g. sporting events, working from home) may be useful and reinforce the notion that all measures the UK implements need to be taken seriously. Not doing so potentially undermines the other actions and trust.”50 |
| 4.24. | During the SAGE meeting, Professor David Halpern, Chief Executive of the Behavioural Insights Team (formerly known as the ‘Nudge Unit’) from 2014, wrote in his notebook “WE ARE NOT READY“. Dr Ben Warner, Special Adviser to the Prime Minister from December 2019 to May 2021, “leaned over, crossed out ‘NOT READY’ and wrote ‘Fucked!’.”51 Professor Halpern’s impression, which he relayed to Mr Hancock later that day, was that “the penny had dropped at that meeting for several people in the room” and that “we really needed to do something about suppression and locking down“.52 |
| 4.25. | Despite the ‘penny dropping’ and the ‘wake-up call’, SAGE concluded that “the UK remains on broadly the same epidemic trajectory and time to peak“.53 It stated in the first version of the minutes that “household isolation and social distancing of the elderly and vulnerable should be implemented soon“.54 On receipt of the minutes, Sir Jeremy Farrar (Director of the Wellcome Trust from October 2013 to February 2023 and a participant in SAGE) expressed concern that this language did not “convey the need for urgency that was palpable at the meeting“.55 An amended version of the minutes was subsequently produced on 16 March 2020, which advised that those measures should instead be implemented “as soon as practical (i.e. they can be done well and equitably)“.56 |
| 4.26. | Mr Hancock explained that, after the meeting, Professor Whitty informed him of SAGE’s view that household isolation and shielding should “come in sooner rather than later” and that greater restrictions could be needed “to make sure case numbers stay within NHS capacity and they were examining options“.57 |
| 4.27. | Mr Hancock told the Inquiry that he had spoken to Mr Johnson and reinforced his view that “we needed to lock down immediately“.58 Mr Johnson said that he did not recall any such discussion.59 Mr Hancock, in the event, was unsure whether he had called or emailed Mr Johnson. The Inquiry was not provided with any contemporaneous material to demonstrate that Mr Hancock had communicated such concerns to Mr Johnson on that day. Given the extraordinary significance of a communication in which the Secretary of State for Health purportedly informed the Prime Minister that an immediate lockdown was required, the fact that lockdown was not yet widely being considered as an option and the absence of any corroborative confirmation, it is likely that Mr Hancock’s recollection was mistaken. |
| 4.28. | Immediately after the SAGE meeting of 13 March 2020, Professor Ferguson spoke to Dr Warner and Imran Shafi (Private Secretary to the Prime Minister for public services from March 2018 to March 2021). Mr Shafi said that he had raised “concerns about our overall approach … arguing that we needed to go further with our measures“.60 Following the meeting, Professor Ferguson emailed Sir Jeremy Farrar and Professor Edmunds:
“I think the message got across. I still think part of the issue is Chris [Whitty] hoping it won’t be as bad as we say. I was amazed that Chris and Patrick [Vallance] haven’t appeared to have previously asked the question … as to whether the NHS could cope with what the govt [government] policy would likely produce.”61 |
| 4.29. | That evening, a number of advisers and officials from 10 Downing Street, led by Mr Cummings, gathered to discuss SAGE’s findings.62 Dr Warner used NHS modelling data and a paper from Professor Ferguson to support his conclusion that the UK “needed to change strategy from mitigation to suppression“.63 Dr Warner and Mr Cummings used a whiteboard to illustrate the problems with the current strategy and to explain the need for the UK government to implement stringent restrictions shortly.64 The whiteboard (see Figure 7) explained that the difference between the mitigation approach to the response currently being pursued by the UK government and that outlined on the whiteboard was that the new approach required “> [more] aggressive [action] next week“.65 It further explained that “[we] [m]ust avoid NHS collapse … [t]o stop NHS collapse, we will probably have to ‘lockdown’” and that this would mean that “e/o [everyone] stays home, pubs etc close“.66 |
Figure 7: Notes on a whiteboard during the meeting at 10 Downing Street on 13 March 2020
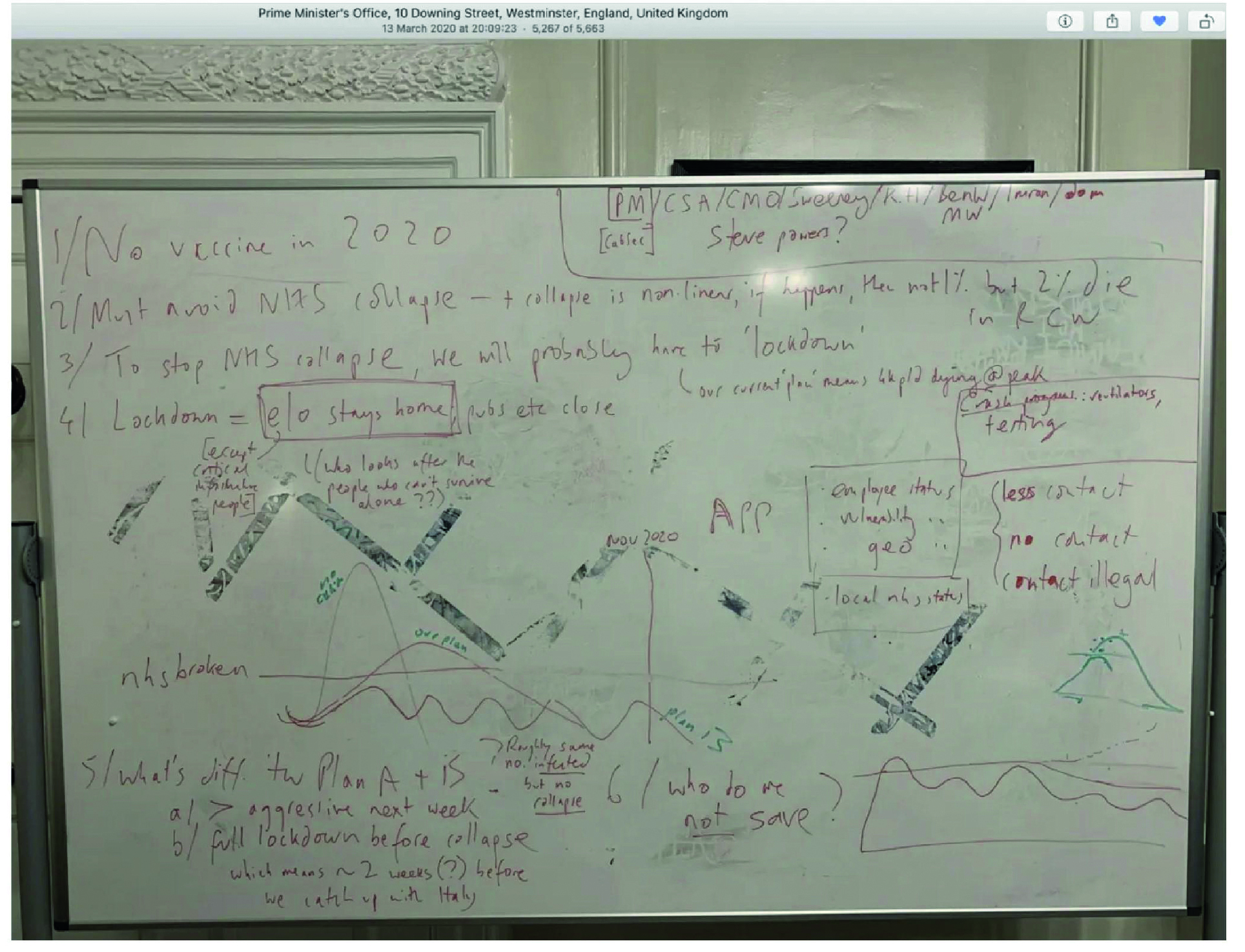
Source: INQ000273872_0045
| 4.30. | Mr Cummings told the Inquiry that it was clear that if the UK government continued to pursue its initial mitigation plan:
“not only would there be thousands of deaths but NHS projections were clear that there would effectively be no NHS at all for anything for a period“.67 The advisers agreed that Mr Johnson must be advised to “change course and introduce a national lockdown as a matter of urgency“.68 |
| 4.31. | Helen MacNamara, Deputy Cabinet Secretary from January 2019 to February 2021, described a “sense of foreboding” in 10 Downing Street on 13 March 2020.69 She had heard that the SAGE meeting had concluded that case numbers were rising faster than thought and was concerned that there was not sufficient urgency.70 She became aware – including through discussions with Mark Sweeney, Director General of Domestic and Economic Affairs in the Cabinet Secretariat from November 2019 to September 2022, who was coordinating with the Department of Health – that there were gaps in the policy for interventions. Mr Sweeney told Ms MacNamara:
“I have been told for years that there is a whole plan for this. There is no plan. We are in huge trouble.”71 |
| 4.32. | Ms MacNamara went into 10 Downing Street that evening and encountered Mr Cummings and others at their meeting. She gave a blunt assessment of the situation:
“We are absolutely fucked. I think this country is heading for a disaster.”72 |
| 4.33. | That evening, Mr Cummings sent a WhatsApp message to a group which included Mr Johnson, Mr Hancock, and Professors Whitty and Vallance, stating:
“[W]e must talk on Monday through the full plan up to lockdown if necessary in time to stop Italy style collapse. If we are 2-4 weeks behind Italy we may have to be more aggressive faster.”73 Professor Vallance replied: “Yes.“74 |
| 4.34. | Professor McBride told the Inquiry that, around 13 March 2020, it was “increasingly apparent” that there were:
“huge pressures on the health service, and particularly in London, and the health service and intensive care beds were about to be overwhelmed“.75 He explained that the Chief Medical Officers for the four nations of the UK met that day to discuss the SAGE update and that “[m]inisters were and should have been fully aware of the way in which things were ramping up“.76 |
| 4.35. | A briefing prepared by the Department of Health (Northern Ireland) on 13 March 2020, in advance of Northern Ireland Executive Committee and COBR meetings on 16 March, referred to the current high consequence infectious disease capacity in the UK having been exceeded. It noted the establishment of a planning sub-group to ensure an appropriate level of preparedness across the health and social care sector.77 The briefing did not provide any detail of the ability of health services in Northern Ireland to cope, nor any detail of concerns that those services could be overwhelmed. |
The weekend of 14 and 15 March 2020
| 4.36. | In the early morning of Saturday 14 March 2020, a discussion took place on WhatsApp between Mr Johnson and Professor Vallance about the plan for responding to Covid-19. Mr Johnson expressed concern about the “terrifying … numbers of infections required for herd immunity to work if that is part of the strategy“.78 Professor Vallance advised Mr Johnson:
“The primary reason for flattening the peak rather than trying to completely [suppress] it is the problem of a severe second wave of outbreak later if we suppress really hard now. Herd immunity is not the strategy, but is a consequence – as more people get infected (as they will), we will start to develop immunity and that will be part of bringing transmission down and bringing it to a halt.”79 |
| 4.37. | Shortly after this exchange, at about 08:00, Professor Vallance sent an email to colleagues which said, “I want to push for faster action.“80 Professor Vallance told the Inquiry that he wanted to push for restrictions to be introduced earlier and that “they may need to be more extensive if the government’s objective of safeguarding the NHS were to be achieved“.81 Professor Edmunds agreed and Professor Ferguson commented that “the policies will need to be more intense” and “go on for longer“.82 Later in the day, Professor Ferguson was asked to prepare a slide deck for Professor Vallance that illustrated the potential healthcare demand resulting from mitigation measures (restrictions to slow the spread) versus suppression measures (restrictions to stop the spread) in a simple manner.83 |
| 4.38. | That morning, Mr Johnson met with Mr Hancock, Professors Vallance and Whitty and several senior officials including Sir Christopher Wormald (Permanent Secretary to the Department of Health and Social Care from May 2016 to December 2024). Professors Whitty and Vallance informed decision-makers of SAGE’s advice from the previous day that the country was now further along the epidemic curve than had previously been understood.84 Mr Hancock explained that Professor Vallance:
“told everyone that while we had thought we were four weeks behind Italy on the epidemic curve, it was now thought that the UK was two weeks behind, which meant there was no time to lose … The data pointed to our reasonable worst-case scenario of over 500,000 deaths becoming a reality unless the Government stepped in hard and fast.”85 Professors Vallance and Whitty indicated that SAGE had advised: “[T]he right time to implement measures in our plan might be sooner than previously envisaged given the latest analysis.”86 |
| 4.39. | Professor Whitty told the Inquiry that, at this meeting, it was made “clear to core decision makers that action was needed at speed, faster than had been previously anticipated“.87 Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021 and Minister for the Cabinet Office from February 2020 to September 2021, explained that this meeting was “a turning point, where we really began to shift gears to a more robust response“.88 |
| 4.40. | Advice was to be provided by SAGE on a package of measures, to be discussed with Mr Johnson the following day, including “how we could implement further social distancing based on the epidemiology, with options ranging up to full lockdown“.89 This was the first time that SAGE had been formally commissioned to consider a lockdown strategy. It was a marked departure from the initial plan set out in the Coronavirus: Action Plan published on 3 March.90 Restrictions to stop the spread of the virus were now under serious consideration in the UK government. |
| 4.41. | Notes from the meeting record that the possibility of a London lockdown in the near future was discussed.91 Mr Gove was recorded as saying “Go now!“92 |
| 4.42. | Immediately after that meeting, Mr Johnson held a small group discussion with members of the 10 Downing Street Private Office, including Mr Cummings, Dr Warner, Mr Shafi, Lee Cain (Director of Communications at 10 Downing Street from July 2019 to November 2020) and Stuart Glassborow (Deputy Principal Private Secretary to the Prime Minister from May 2019 to May 2022).93 |
| 4.43. | Dr Warner explained that he told Mr Johnson:
“[W]ith the current plan, we would quickly overload the NHS. Once the NHS was broken, it would not be able to treat those with Covid, and therefore those with survivable Covid would die. In addition, people would not be able to get treatment for regular conditions such as heart attacks. This meant that the number of deaths that would occur would be significantly higher than just the infection fatality rate from Covid.”94 Dr Warner used a whiteboard to brief Mr Johnson to this effect (see Figure 8). |
Figure 8: Notes on a whiteboard during the meeting at 10 Downing Street on 14 March 2020
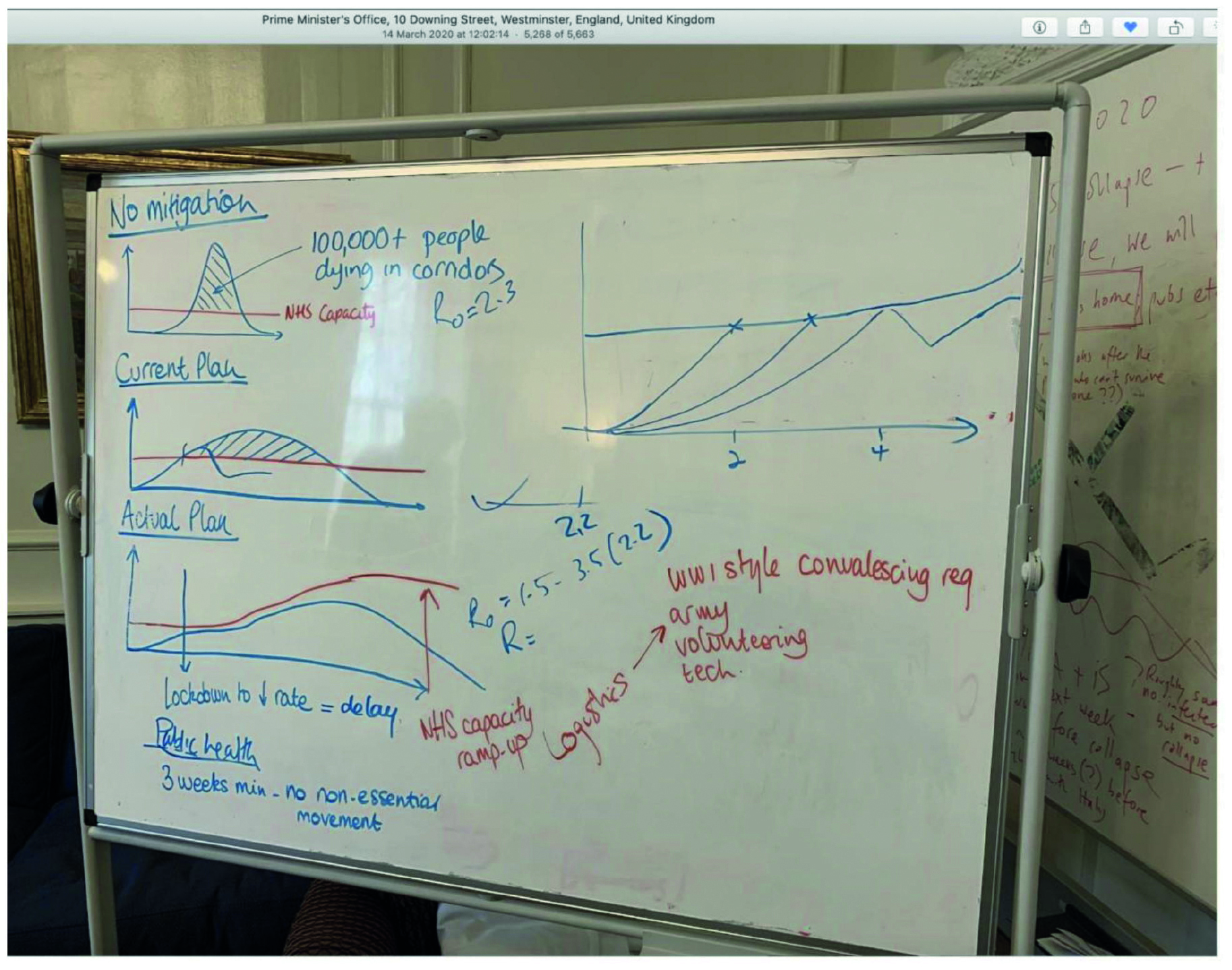
Source: INQ000196057
| 4.44. | Mr Johnson told the Inquiry: “It was absolutely clear by the Saturday that we had to act. We were out of time.“95 According to Mr Cain:
“[T]he collective agreement in the room was that a full lockdown was the only strategy which could suppress the spread of Covid-19, save the NHS from collapse, and ultimately buy the Government more time, and that ‘flattening the curve’ could only really work as an interim measure until full lockdown could be achieved.”96 |
| 4.45. | Mr Shafi told the Inquiry that Mr Johnson:
“agreed that he wanted to look at more aggressive measures, but did not decide in this smaller meeting on whether to implement them. He asked for the CMO [Chief Medical Officer] and CSA [Chief Scientific Adviser] – who were not present during this discussion – to validate the argument for firmer action presented in the room.”97 |
| 4.46. | Mr Cummings told the Inquiry that Mr Johnson “asked reasonable questions including ‘why aren’t Hancock, Whitty, Vallance telling me this?’“.98 |
| 4.47. | Mr Johnson said that, prior to the morning of Saturday 14 March 2020:
“[N]either SAGE, nor our scientific advisers had said that we were on the brink of a total lockdown. They may have begun to think it was possible, given the data we could all see. But they did not spell it out, or certainly not explicitly, as far as I can remember.”99 However, he explained that, at the meeting that morning, “the picture changed, or certainly my assumptions changed“, and “it was clear that on current trends we might very soon be obliged to lock down the whole country“.100 This would be “an immense undertaking and could not be done overnight“.101 |
| 4.48. | On the afternoon of Saturday 14 March 2020, Mr Cummings exchanged WhatsApp messages with Mr Johnson about flaws in the advice previously presented to him and failures within the Cabinet Office and the Department of Health and Social Care to appreciate the urgency of the situation (see Figure 9). |
Figure 9: Message from Mr Cummings to Mr Johnson on 14 March 2020
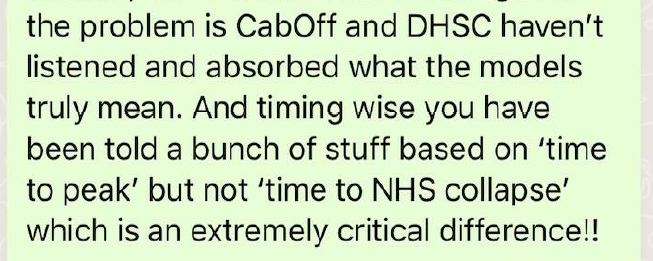
Source: INQ000048313_0007
| 4.49. | Later that evening, Mr Cummings suggested in a WhatsApp group with Mr Johnson, Mr Hancock, Professors Whitty and Vallance and Mr Cain that, on Monday 16 March 2020, the public should be told that the UK government would do what was required to prevent the collapse of the NHS, “including extreme social distancing / lockdown“.102 This consisted of “social distancing, work from home, oldies shouldn’t go to weddings etc, closing pubs and nightclubs etc“.103 He stated that this:
“means doing a bunch of stuff roughly 2-3 weeks (i think??) before we think the crunch point is cos there is a time lag on the effects and the cases already in the system feeding through to ICUs“.104 Professors Whitty and Vallance broadly agreed.105 Professor Vallance explained that the new modelling of further restrictions would be provided on 15 or 16 March for decision-makers to consider.106 |
| 4.50. | The discussion on WhatsApp about the UK government’s approach continued into the evening of 14 March 2020. Mr Hancock noted that the UK government’s initial response was “predicated, explicitly, on the inevitability of global spread” and questioned whether that was, in fact, inevitable. Professor Vallance suggested that they should “discuss tomorrow live“.107 |
| 4.51. | The implications of SAGE’s advice on 13 March 2020 were also considered in Wales on 14 March. Dr Rob Orford, Chief Scientific Adviser (Health) for Wales from January 2017, informed Dr (later Sir) Frank Atherton, Chief Medical Officer for Wales from August 2016, and Dr Goodall about the discussions at SAGE regarding NHS capacity. He queried if it was possible to determine whether the three sets of control measures would “reduce demand sufficiently for the re-aligned system to cope” in Wales.108 This was significant:
“not just for ensuring the NHS is not overwhelmed but also as it might mean a change in the current population level approach towards more restrictive measures, which has a knock-on impact on herd immunity, potentially longer periods of measures and a more difficult winter“.109 Officials within the Welsh Government then went on to consider venues that could be used for step-down care, isolation facilities and “nightingale type wards“. Dr Orford responded, stating “we need to throw the kitchen sink at it“.110 |
| 4.52. | Some mass gatherings continued to go ahead. Two Stereophonics concerts went ahead in Cardiff on 14 and 15 March 2020. However, a Six Nations rugby match between Wales and Scotland, due to take place on 14 March, was called off by the Welsh Rugby Union the day before.111 The Welsh Government had powers under the Public Health (Control of Disease) Act 1984 to prohibit such gatherings.112 Public Health Wales had recommended, on 13 March, cancelling the match due to concerns about the number of people who would be travelling and “the impact of crowding in pubs and other venues“.113 Mark Drakeford MS, First Minister of Wales from December 2018 to March 2024, said that the Welsh Government did not advise against it going ahead because the scientific advice did not justify interference and there was not an agreed four-nations approach.114 |
| 4.53. | At about 00:30 on 15 March 2020, Professor Graham Medley (Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine and Co-Chair of SPI-M-O from January 2020 to February 2022) warned Professors Whitty and Vallance that his latest review of the data suggested:
“[T]ransmission is growing faster than all expectation … we are days away from facing NHS overall load in 3 weeks.”115 However, he noted that this could be attributed to a problem with the data. Professor Vallance replied and stated that he had “primed the politicians yesterday that this all looks closer than it did“.116 |
| 4.54. | Shortly before 04:00 on 15 March 2020, in an email marked ‘Urgent’ sent to Professors Whitty and Vallance, Professor Ferguson explained that the “minimum policy” required to avoid NHS England surge capacity being overwhelmed would involve:
“closing schools and universities, home isolation of cases, and large-scale intensive social distancing – reducing all contacts outside the home and work by 75%+, preferably reducing work contacts by some extent”.117 He explained that this policy was: “basically suppressing transmission, so population immunity will build up slowly. In the absence of a vaccine, we’ll still be doing it in over a year’s time.”118 Professor Ferguson also forwarded the email to Dr Warner, commenting: “Even if we reduced the epidemic by or more, it would still look very bad at the peak. What has changed is that NHSE has been more definitive at saying they are a long, long way away from coping with such levels of demand.”119 |
| 4.55. | Professor Ferguson told the Inquiry that this was the moment at which it became “clearly apparent that exceeding NHS capacity was a government red line” and that these were the policies that needed to be implemented in order to achieve this.120 |
| 4.56. | Professor Edmunds also advised Professors Whitty and Vallance via email:
“[W]e need a precautionary approach to our social distance policy. If the data are unreliable, then we need to step up our social distance measures much more rapidly than we might otherwise have thought necessary. I think we should immediately introduce HH [household] quarantine, banning of all social contacts (bars, restaurants, cinemas etc, in particular) and cocooning for the old and high risk groups. We might also want to flag up school closure.”121 |
| 4.57. | Professor Vallance told the Inquiry that, by this point, it was his “clear view that more extensive NPIs [non-pharmaceutical interventions] would have to be introduced” to safeguard the NHS in England “as early as possible, meaning within the coming week at the latest“.122 |
| 4.58. | At 09:37 on 15 March 2020, Professor Vallance emailed Professor Whitty and outlined that the two aims of the response were now:
“1. To ensure that the curve of the epidemic is flattened to a degree that allows the NHS to cope 2. Protect lives through appropriate shielding of the elderly and vulnerable.”123 To achieve this, household isolation, shielding and enhanced social distancing should be implemented “as soon as it is practical to do so“.124 |
| 4.59. | At about 10:30, Professor Vallance advised Mr Johnson they would need to “move to the stricter quarantine and social distancing“.125 A short time later, Mr Johnson responded: “Seeing what happened in Italy we simply have NO TIME.”126 |
| 4.60. | At 12:18, Mr Cummings informed Mr Johnson that Professor Vallance agreed that more stringent measures were now needed (see Figure 10). |
Figure 10: Message from Mr Cummings to Mr Johnson on 15 March 2020
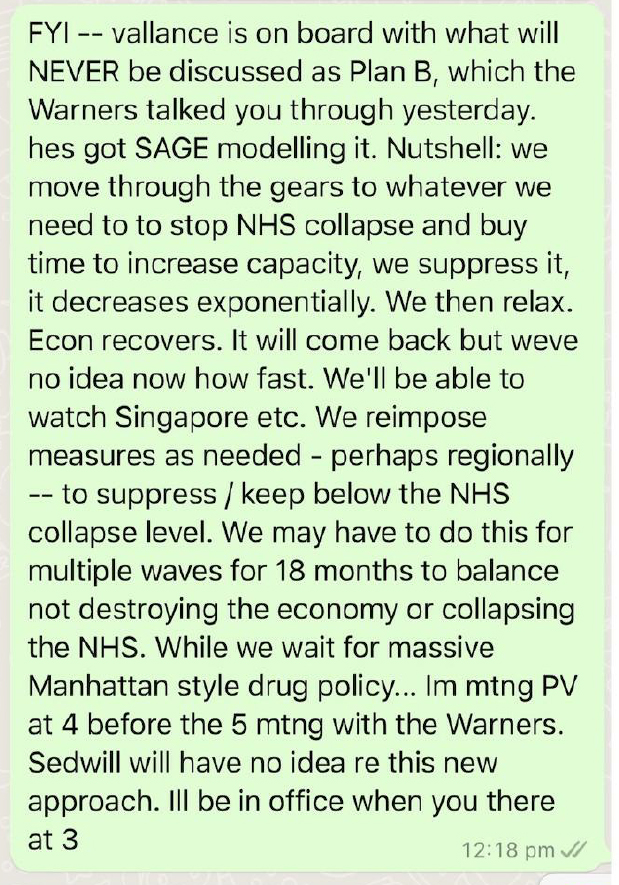
Source: INQ000048313_0008
| 4.61. | At about 13:00, Professor Ferguson emailed Professors Whitty and Vallance regarding a paper that his team was preparing to publish the following day. He explained:
“[W]e will conclude that suppression is the only feasible strategy given how much hospital demand is likely to be exceeded.”127 |
| 4.62. | Professor Edmunds and Sir Jeremy Farrar also emailed during the afternoon urging the implementation of stringent restrictions.128 |
| 4.63. | It appeared that there was some reluctance within the Cabinet Office and Department of Health and Social Care to adopt the new approach advised by scientific advisers.129 On the afternoon of 15 March 2020, a ‘pre-meet’ in preparation for a ministerial meeting with Mr Johnson was described by Ms MacNamara as “scratchy“.130 She explained that, by this, she meant that:
“it felt like we really were in slightly different places in terms of a group of us in the centre who had got much further on how bad this would be quite quickly, and a … concern from DHSC [the Department of Health and Social Care] who knew as well if not better than we did that the planning wasn’t there to support this“.131 Ms MacNamara recalled that the Department of Health and Social Care’s view was: “to wait until the latest possible moment to tell people they had to stay at home whereas – based on the previous 24 hours – the Cabinet Office view was to follow the CMO’s advice and lock down in 10 days at the latest and earlier if possible with every day helping to stem the tide“.132 |
| 4.64. | A meeting chaired by Mr Johnson took place at 17:00 to discuss a further package of restrictions to be approved by COBR the following day.133 It was attended by Mr Hancock, Professors Whitty and Vallance, Sir Mark Sedwill (later Lord Sedwill), Cabinet Secretary and Head of the Civil Service from October 2018 to September 2020, and Mr Cummings as well as other advisers and civil servants. A SAGE paper was presented at the meeting which advised that approximately 5% of Covid-19 cases would require hospitalisation and, of those, 30% would need ventilation.134 These figures were now “NHS central case planning assumptions” as they were no longer a distant or unlikely possibility, but reality.135 The UK government’s Covid-19 Dashboard (published for the first time on 15 March 2020, although it did not contain any data on hospitalisation rates or occupied intensive care beds) was also presented.136 It made clear that, if the restrictions that had been under consideration to date were implemented, surge critical care bed capacity in the NHS would still be overwhelmed “by 8-fold”, and that remaining within NHS capacity would “require more intensive social distancing”.137 |
| 4.65. | At the meeting, Mr Cummings argued: “[W]e should accelerate everything and go further and accept the risks of suppression and future waves to buy time.“138 Professor Vallance suggested the need for “an urgent lockdown at this meeting“.139 He told the Inquiry he was later informed that Sir Christopher Wormald and Sir Mark Sedwill were “incandescent” with him for raising this in the meeting.140 Sir Christopher Wormald told the Inquiry he did not recollect this and that the meetings in 10 Downing Street were “tense but business like”.141 Slides were presented at the 15 March 2020 meeting that advised implementing various restrictions and outlined their potential impact.142 |
Figure 11: Notes on a whiteboard during a ministerial meeting on 15 March 2020
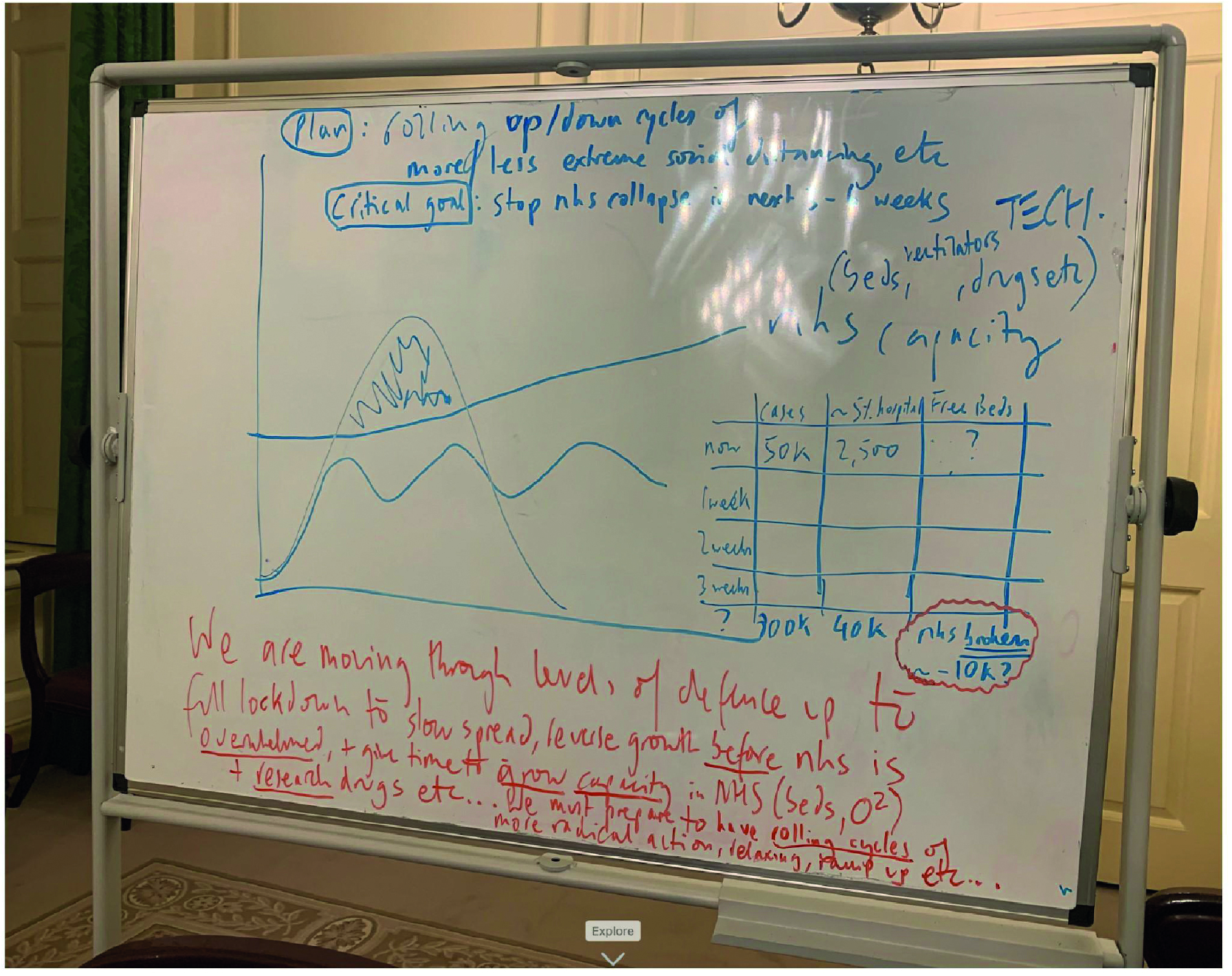
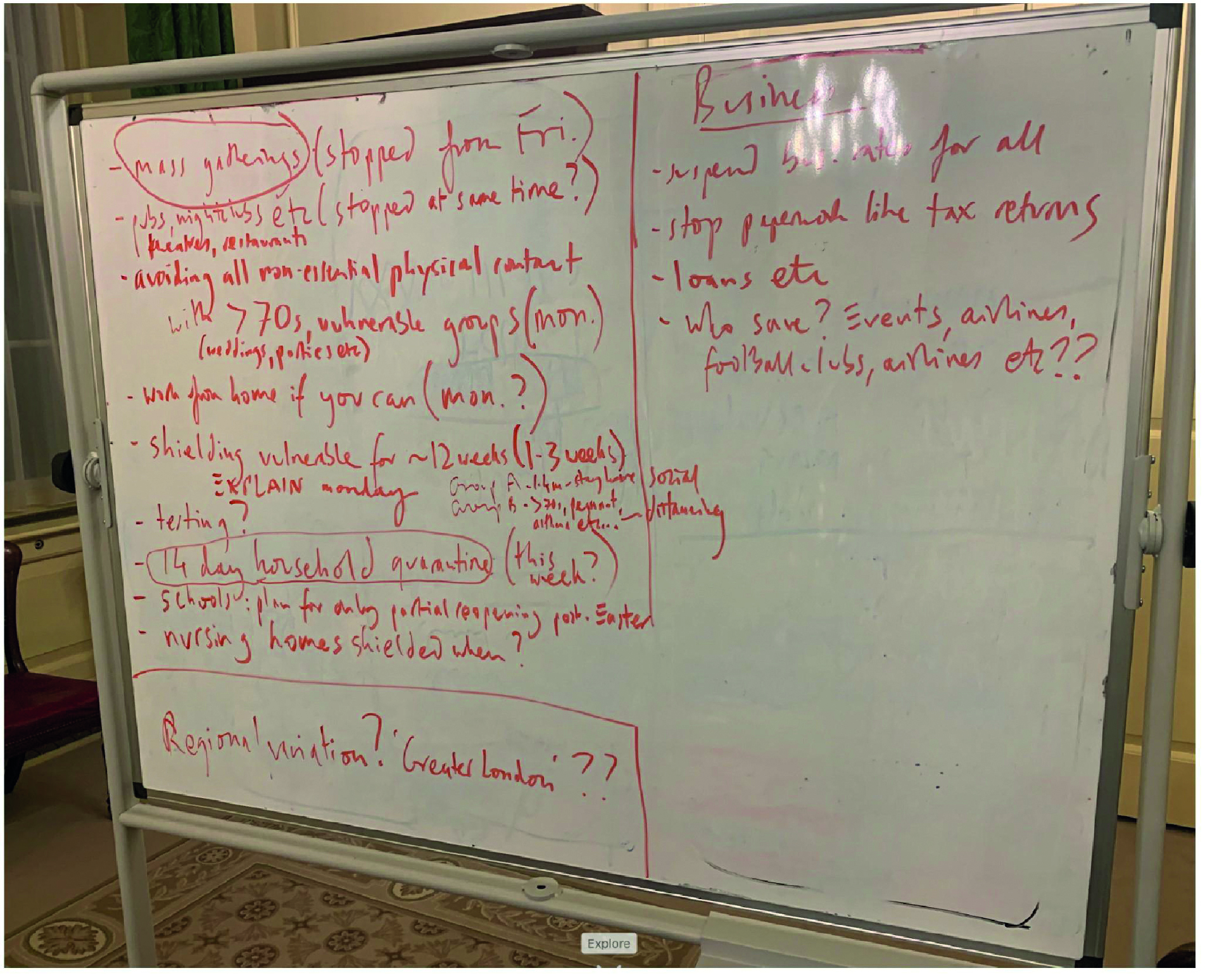
Source: INQ000273872_0052-0053
| 4.66. | Mr Johnson agreed to take a package of proposed measures to COBR the following day. These included immediate introduction of household isolation and advice that members of the public should socially distance, although this would be voluntary. Those aged over 70, pregnant women and people with particular health conditions would be advised to follow this advice more rigorously. The proposed measures also included the introduction of shielding for about 1.4 million clinically vulnerable people within a week.143 Although SAGE had noted on 13 March 2020 that not cancelling mass gatherings “potentially undermines the other actions and trust”, it was also agreed to advise but not mandate a cancellation of mass gatherings and to direct that no public services support would be provided to any such events.144 |
| 4.67. | In Scotland, on 14 March 2020, Nicola Sturgeon MSP (First Minister of Scotland from November 2014 to March 2023) was said to be “uneasy” about the UK government’s approach on the basis that it appeared to be out of step with other countries and the World Health Organization.145 She asked to discuss with Dr Catherine Calderwood (Chief Medical Officer for Scotland from April 2015 to April 2020) and others the “aggressive containment approach that many other countries appear to be taking versus the UK manage it / flatten curve approach“. She was concerned that the public was “already so far ahead of SAGE approach” in its behaviour and queried whether this “must surely change all the assumptions” on which the scientific advice to wait to implement restrictions was based. She questioned whether, in light of this, further restrictions should now be implemented, including social distancing for everyone and shielding for the elderly and vulnerable. |
| 4.68. | On 15 March 2020, there was a meeting of senior officials of the Scottish Government Resilience Room to discuss the advice that would be tendered to Scottish ministers in preparation for the COBR meeting the following day.146 Dr Calderwood noted that some measures might be in place for a significant length of time and, as such, it was important not to implement any restrictions too soon.147 She also made “very clear” that the scientific evidence did not justify any school closures.148 |
The situation on 15 March 2020
| 4.69. | By the weekend of 14 and 15 March 2020, it had become apparent within the UK government that stringent measures were necessary. The NHS in England would not be able to provide care for the large number of people infected with Covid-19 who were likely to need hospital treatment, in particular those requiring intensive care. |
| 4.70. | Professor Vallance in particular played a key role in bringing about the change of direction over that weekend. He told the Inquiry:
“[I]t became very clear that much more stringent measures would be needed … and they needed to be introduced quickly. I made my views known about that, that that was the view of the SAGE committee and the modellers, and it was my view that we were in a position now where we had to move quickly. That decision, I believe, was understood.”149 Professor Vallance explained that, at the meeting on 15 March 2020, he was: “unambiguous … that much more stringent measures would be needed now … I also suggested on that day that London was so far ahead that it would be necessary to possibly lock down London.”150 He said: “[O]n that weekend an in principle decision was taken that lockdown would be required. It then took several more days to work that into a full mandatory process.”151 |
| 4.71. | As it was, the delays in NHS data and modelling, the realisation that the reasonable worst-case scenario was likely to materialise and the emergence of new data indicating a higher level of cases combined to create the perfect storm. Nothing less than stringent restrictions to reduce the reproduction number (R) below 1 would now suffice to prevent the NHS in England being overwhelmed. The devolved nations were also facing a trajectory of increasing cases, the natural consequence of which would be similar unsustainable pressures on their NHS systems. The governments of the UK had left themselves no option other than to immediately implement stringent restrictions to stop the spread of the virus. |
16 March 2020: An ‘advisory’ lockdown
| 4.72. | On 16 March 2020, the Northern Ireland Executive Committee met to consider a paper concerning the phased activation of the Northern Ireland Central Crisis Management Arrangements (referred to as NICCMA). This was the first point at which consideration was given to initiating cross-government civil contingency arrangements and it was agreed that the activation point had been reached.152 The Executive Committee also discussed planning, though at a rudimentary level, concluding that Executive departments “can prepare own plans but have to join up“.153 |
| 4.73. | New UK government decision-making structures came into effect on 16 March 2020.154 These included:
|
| 4.74. | A meeting chaired by Mr Johnson on the morning of 16 March 2020 discussed the need to plan for a lockdown in London, due to a sharp rise in cases in the city.157 Professor Vallance told the Inquiry that, at this meeting, he argued:
“[A] lockdown for at least London would be required if the government’s stated policy of protecting the NHS and the vulnerable was to be achieved.”158 |
| 4.75. | The Covid-19 Dashboard published on 16 March 2020 did not contain data on hospitalisation. It stated:
“Data was collected on 16 March but is believed to be inaccurate. Processes are being improved and accurate data is promised from 17 March.”159 These data on hospitalisation would not be provided in the UK government’s Covid-19 Dashboard until 20 March.160 However, on 16 March, data from the new NHS Covid SitRep system became available.161 These set out the total daily numbers of patients who had been admitted to hospital or diagnosed with Covid-19, as well as data relating to bed occupancy and ventilator use. As a result, decision-makers in the UK government did not have an up-to-date understanding of NHS resources or the NHS’s surge capacity until mid-March 2020. Data from the COVID-19 Hospitalisation in England Surveillance System (CHESS) concerning hospitalisation and intensive care unit cases also became available on 16 March. However, it was not until late March that CHESS was able to provide a more complete picture of these data.162 |
| 4.76. | SAGE met at 13:00 on 16 March 2020.163 It recognised that the objective of implementing restrictions was now:
“to avoid critical cases exceeding NHS intensive care and other respiratory support bed capacity. The figures for capacity are now clear but intensive care bed capacity will increase by 20% or more.”164 |
| 4.77. | As a result of the emergence of new infection data on 13 March 2020 and data on NHS critical care capacity, SAGE’s advice “changed regarding the speed of the implementation of additional interventions“.165 At its meeting on 16 March, SAGE recommended that:
“additional social distancing measures be introduced as soon as possible … to be accompanied by a significant increase in testing and the availability of near real-time data flows to understand their impacts“.166 SAGE explained: “[A]ntibody testing is particularly vital to address the central unknown question of the ratio of asymptomatic to symptomatic cases.”167 Public Health England stated: “[T]esting is being scaled up over the coming weeks to 10,000 per day – focused on intensive care units, hospital admissions and key workers.”168 |
| 4.78. | At this meeting, SAGE considered Imperial College London’s Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand, which advised that suppression was now “the preferred policy option“.169 The report concluded that restrictions designed only to slow the spread of Covid-19, such as self-isolation, household isolation and social distancing of the elderly and others at most risk of severe diseases (shielding), would be likely to lead to “emergency surge capacity limits of the UK … healthcare systems … being exceeded many times over” and about “250,000 deaths” in Great Britain.170 However, it noted that implementing stringent restrictions designed to stop the spread of the virus would be challenging as they would need to be maintained until a vaccine was available to avoid an exit wave. This could be in 18 months or longer.171 |
| 4.79. | Professor Vallance told the Inquiry that this report confirmed his view that:
“more extensive NPIs would have to be introduced earlier in order to meet the government’s policy objectives“.172 |
| 4.80. | A SPI-M-O paper considered at the SAGE meeting advised that social distancing by the general public, school closures, self-isolation, household isolation and shielding should be “followed as soon as practical“.173 SAGE explained that it could not be certain that the measures agreed by the UK government the previous day would be sufficient “to push demand for critical care below NHS capacity but they may get very close under the [reasonable worst-case] scenario“.174 It emphasised, however, that “[c]ompliance with the measures by the public” would be “key” for the restrictions to have the intended effect and it would take “two to three weeks before the impacts of measures are observed (this needs to be monitored carefully)“.175 |
| 4.81. | School closures were not part of the package of restrictions considered for immediate implementation. SAGE explained that, while closing schools was one of the less effective measures in reducing the peak, “it may nevertheless become necessary” to do so in future “in order to push demand for critical care below NHS capacity“.176 Further modelling of school closures was therefore commissioned from SPI-M-O and this would be considered by SAGE at its next meeting.177 SAGE also raised an action point for the Department of Health and Social Care, NHS England and Public Health England:
“to urgently work with NHSX and GO-Science on a data strategy, ensuring there is access to real time data to track the UK epidemic“.178 |
| 4.82. | Professor Ferguson described this SAGE meeting as “a significant pivot towards advising rapid introduction of more intensive” interventions, driven by two factors:
Professor Whitty similarly told the Inquiry that SAGE’s advice from 16 March 2020 was “extremely clear: that without action we were going to be in very deep trouble“.180 |
| 4.83. | Mr Johnson chaired the COBR meeting convened at 15:15 on 16 March 2020 to approve the package of further interventions to slow the spread of the virus that had been agreed at the UK government meeting he had chaired the previous day.181 It was attended by leaders from the devolved administrations as well as, for the first time, Sadiq Khan (later Sir Sadiq Khan), Mayor of London from May 2016. Professor Whitty advised that the UK:
“was now at the cusp of a fast upward swing of the infection curve. On the basis of the NHS capacity model, further action should be taken.”182 |
| 4.84. | A commonly recognised information picture (CRIP) presented to COBR advised the implementation of a package that had been worked up the previous day. The package consisted of household isolation and ‘soft’ social distancing for the whole population (through encouraging people to work from home and limit their social mixing), particularly for those aged over 70, those with long-term medical conditions and pregnant women.183 It also advised that shielding for the most vulnerable be implemented in England within the next week and that public services support should no longer be provided for mass gatherings, which would be advised not to go ahead.184 It advised “no change recommended for now” in respect of school closures.185 COBR approved the recommended package.186 |
| 4.85. | That evening, at a 10 Downing Street press conference, Mr Johnson told the public:
“[W]e need to go further, because according to SAGE, it looks as though we’re now approaching the fast growth part of the upward curve. And without drastic action, cases could double every 5 or 6 days.”187 He announced the package of restrictions approved at COBR earlier that day, including:
|
| 4.86. | Mr Johnson emphasised that social distancing was “particularly important” for people aged over 70, pregnant women and those with some health conditions.189 He stated that shielding for those with “the most serious health conditions” would be implemented in “a few days time“.190 He said that the reason these restrictions were being implemented now was because:
“the right moment, as we’ve always said, is to do it when it is most effective, when we think it can make the biggest difference to slowing the spread of the disease, reducing the number of victims, reducing the number of fatalities“.191 |
| 4.87. | People in London – which was said to now be “a few weeks ahead” – were asked to “pay special attention” to the guidance about social distancing.192 Mr Johnson also explained that, from 17 March 2020, mass gatherings would no longer be supported by the emergency services in England.193 He stated:
“[I]t is far more now than just washing your hands – though clearly washing your hands remains important.”194 |
| 4.88. | Similar announcements were made across the UK that day. Ms Sturgeon advised people to avoid crowded areas and gatherings, including hospitality settings, and to avoid public transport as much as possible.195 Working from home was recommended wherever possible. In Northern Ireland, The Executive Office announced the package of measures.196 In Wales, Mr Drakeford announced these new restrictions on 17 March 2020, following the announcement of the first death in Wales due to Covid-19 on 16 March.197 |
| 4.89. | Professor Whitty told the Inquiry that he advised the UK government that SAGE was “strongly in favour” of this package of restrictions.198 He explained that they represented:
“a very major policy shift and a substantial move away from the personal philosophy of the Prime Minister … It was also a major departure from the assumed policy of the previous planning for an influenza pandemic.”199 He noted that the restrictions announced on 16 March 2020 were the “start of the Government’s efforts to make a strong push for a reduction in social interactions“, rather than those subsequently announced on 23 March.200 |
| 4.90. | Mass gatherings should have been stopped before this point. Professor Vallance told the Inquiry that, on reflection, mass gatherings:
“should have been stopped earlier together with instructions about smaller indoor meetings and gatherings in pubs and clubs“.201 Professor Sir Jonathan Van-Tam, Deputy Chief Medical Officer for England from October 2017 to March 2022, agreed that the continuation of mass gatherings was “unhelpful“.202 Professor Whitty said that, with hindsight, he would approach the issue of mass gatherings differently.203 He stated that scientific advice on mass gatherings missed the important point that allowing these gatherings to go ahead “signalled to the general public that the government couldn’t be that worried” and gave an impression of “normality at a time that what you’re trying to signal is anything but normality“.204 He also observed that scientific advice “likely underestimated the risk involved in travel to and from venues and in getting into the venue itself“.205 Professor McBride, who told the Inquiry that his advice to the Minister of Health in Northern Ireland had been aligned with SAGE’s recommendations, made similar observations.206 |
| 4.91. | Mr Johnson conceded in hindsight that, while he followed scientific advice on mass gatherings, the UK government perhaps ought to have cancelled them “as a symbol of the government’s earnestness“.207 Ms Sturgeon noted that the rugby match of 8 March 2020 had taken place the weekend before that announcement was made and noted: “[I]f I have a regret it is not that I took the decision too early, it’s that we took it too late.“208 Reflecting on the Welsh Government’s decision not to intervene in relation to the Scotland versus Wales Six Nations match originally scheduled for 14 March 2020, Mr Gething told the Inquiry: “[I]n all of the awkward choices we made that is definitely one that jars and I recognise that.“209 |
| 4.92. | While scientific advice was clear that mass gatherings would not make a significant contribution to the spread of Covid-19, this advice did not sufficiently take into account the epidemiological risks of travel to and from events, which, for the majority of people, would be on (usually crowded) public transport. Nor did it sufficiently take into account the risks associated with groups socialising indoors before or after the event or watching the event on television in pubs.210 Further, it underestimated the importance of the message to the public to avoid unnecessary social contact. In any event, given the spread of the virus and that its containment had effectively been lost, it was wrong for the four governments not to prevent mass gatherings going ahead in March 2020 when Covid-19 was already circulating in the community. This sent the wrong message of normality at a critical point in the pandemic response. |
| 4.93. | On the evening of 16 March 2020, 10 Downing Street officials and advisers discussed the lack of centrally held plans in the UK government.211 Two days earlier, Munira Mirza (Director at the 10 Downing Street Policy Unit from July 2019 to February 2022) had emailed Clare Brunton (Private Secretary at 10 Downing Street), asking whether the Civil Contingencies Secretariat had a detailed civil contingencies plan for the response, as well as the NHS plan.212 On 16 March, Ms Brunton told Ms Mirza, Dr Warner, Mr Cummings and other 10 Downing Street officials:
“Apparently departments hold their own detailed civil contingencies plans, as well as their business continuity plans. We do not have these centrally. The NHS also hold their own plans. CCS [the Civil Contingencies Secretariat] are working with DHSC to get appropriate sight of this.”213 In response, Dr Warner asked whether this meant “that the department of health haven’t seen the NHS plans yet?“214 |
| 4.94. | Ms MacNamara told the Inquiry that she was still not sure whether the plans did exist somewhere, but, if they did, they “didn’t exist in a way that was usable” by the Cabinet Office to coordinate the response.215 Mr Cummings described this as “shocking“:
“This was another terrible sign fundamental things were broken: how could CCS not have departmental pandemic plans by 16/3?“216 (emphasis in original) The Inquiry agrees with Mr Cummings: it is astonishing that bodies like the Civil Contingencies Secretariat and the Cabinet Office, which were charged with coordinating the response, still did not have sight of departmental civil contingency plans by the time the UK government had been advised to implement stringent restrictions. |
17 March 2020
| 4.95. | On the morning of 17 March 2020, Mr Cummings informed Mr Johnson that further restrictions might be necessary to avoid the collapse of the NHS in England:
“We may have to close schools and order full curfew in London within days I think or else Italy collapse.”217 |
| 4.96. | At 10:30, Mr Johnson informed the UK Cabinet of the restrictions that he had announced the previous day.218 He also explained that people occupying beds in hospitals who would otherwise be in social care should be supported to leave hospital to free up capacity.219 That same day, Sir Simon Stevens instructed NHS England to “urgently discharge all hospital inpatients who are medically fit to leave” in order to free up 30,000 or more beds.220 Sir Simon Stevens also advised that trusts should assume that they would need to postpone all non-urgent elective operations from 15 April 2020 for at least three months.221 |
| 4.97. | Steps were also being taken to increase NHS capacity in Scotland on 17 March 2020. NHS Scotland was placed on an emergency footing in order to double intensive care unit capacity and increase NHS bed capacity from 13,000 to 16,000.222 Non-urgent elective operations would also be suspended and steps taken to increase NHS staff capacity.223 |
| 4.98. | The Scottish Cabinet also met that day. It agreed that managing the response to the virus should now be the Scottish Government’s central objective.224 Ms Sturgeon told the Scottish Cabinet:
“[F]ar more stringent steps would now be required in order to suppress (as far as possible) the spread of the virus, to protect and allow time for the scaling up of the capacity of the NHS, and – ultimately – to save as many lives as possible.”225 She also explained that the measures announced the previous day “were not necessarily the end point“.226 |
| 4.99. | Dr Calderwood explained that Scotland was “probably only days behind England in the spread of infection” and that if the clear messaging about limiting social contact proved ineffective “action would be taken to move to compulsory measures“.227 She informed the Scottish Cabinet that the significant increase in cases in London was “one of the major factors” that had led to the decision to put in place further restrictions on 16 March 2020.228 She explained that “a ‘zoned’ response in different parts of the UK had been assessed as unsafe, given the risk of confusion over mixed messages“.229 |
| 4.100. | Dr Calderwood noted that a reduction in social contact by 75% “could have a significant impact on the outbreak and contribute to keeping the ‘peak’ level within the capacity of the NHS“.230 Dr Calderwood advised that:
“[d]istancing measures would need to last for at least three to four months to be effective, and it would be vital to maintain public trust by being open with people about this from the outset, rather than suggesting that things would improve in a matter of weeks – which they would not“.231 |
| 4.101. | In Northern Ireland, in an email to David Sterling (later Sir David Sterling), Head of the Northern Ireland Civil Service and Permanent Secretary to The Executive Office from June 2017 to August 2020, and other senior civil servants, Karen Pearson (Director of Covid-19 Strategy and Recovery, Civil Contingencies and Programme for Government at The Executive Office from March 2020) mapped out a potential executive strategy and action plan.232 Ms Pearson explained that her:
“thinking was that co-ordinated effort across Departments, in a way which assisted Executive decision-making and monitoring would be essential“.233 |
Dashboard 04: 17 March 2020
Estimated population infected: 30,000–40,000 (awaiting SAGE confirmation)
Total confirmed cases UK: 1,950 (1,557 in England, 195 in Scotland, 136 in Wales and 62 in Northern Ireland)
Deaths: 74 (71 in England, 2 in Scotland, 1 in Wales and 0 in Northern Ireland)
Number of tests carried out: 41,953
Source: INQ000055918_0003
18 March 2020: Closing schools and London lockdown
| 4.102. | The Welsh Government had been working on the assumption on 17 March 2020 that the “best thing to do would be to keep schools open“. However, Mr Drakeford and Kirsty Williams MS (Minister for Education in the Welsh Government from May 2016 to May 2021) jointly decided on the morning of 18 March that schools in Wales should be advised to close from 20 March.234 Schools would be repurposed to support “those most in need, including people involved in the immediate response to the coronavirus outbreak“.235 Dr Orford advised the Covid-19 Core Group that morning that the NHS was “four to five weeks away from maximum capacity“.236 |
| 4.103. | Mr Cummings sent a message to Mr Johnson that morning stating:
“All schools nationwide closed from Friday [ie 20 March]. Announced today. Minimum. I think London lockdown from Saturday.”237 |
| 4.104. | Mr Cummings also messaged Professor Vallance that morning and said that the “soft” advisory social distancing restrictions that had been introduced on 16 March 2020 were “causing a lot of confusion” among the public.238 Professor Vallance agreed:
“We need to have the effect on behaviour and if we are not then we need to go harder and make it clear we mean it.”239 |
| 4.105. | School closures in England were discussed at the Covid-19 Strategy Ministerial Group meeting at 09:15, ahead of further advice from SAGE that day.240 According to Sir Gavin Williamson MP, Secretary of State for Education from July 2019 to September 2021, his recommendation to Mr Johnson was that schools should close on 3 April 2020 for the Easter holiday and thereafter should be open only for vulnerable children.241 However, the minutes of the meeting recorded him saying that schools should close in England on 20 March 2020, before being repurposed to provide childcare to key workers and to children in need or at risk.242 Mr Johnson told the Inquiry that he recognised at this point that school closures were “now inevitable“.243 In Module 8: Children and young people, the Inquiry is examining in further detail the sequence of decision-making about the closure of schools. |
| 4.106. | At the meeting, they also considered a paper entitled ‘”Lockdown” in London’ which discussed options for imposing strict measures to curb the spread of Covid-19.244 The most recent data showed a 30% increase in overnight cases and deaths.245 Although the data lagged behind slightly, the trend was considered likely to be accurate and there would be a two-week lag before the measures already taken would have an impact.246 As a result, the impact of those measures in reducing R – and therefore whether they were sufficient to bring cases within NHS capacity in England – would not be known for two weeks. |
| 4.107. | It was agreed that restrictions for London would be discussed at the Covid-19 Strategy Ministerial Group meeting the following morning and COBR would take a decision on school closures later that afternoon.247 |
| 4.108. | The Scottish Government had been considering the closure of schools during the previous week. At the Scottish Cabinet meeting held on 17 March 2020, it was noted:
“[The] epidemiological evidence did not suggest that this measure would slow the transmission of COVID-19 down to a great extent (and might in fact cause some additional infections – for example by increasing children’s exposure to grandparents over 70).“248 |
| 4.109. | The Scottish Cabinet agreed that:
“[t]he advantages and drawbacks of closing schools and other educational establishments should be considered further over coming days in light of emerging evidence across the UK“.249 However, Ms Sturgeon and John Swinney MSP (Deputy First Minister of Scotland from November 2014 to March 2023) discussed school closures after the Cabinet meeting on 17 March 2020 and again on 18 March.250 Mr Swinney explained that, on the evening of 17 March, he had received advice that it was “likely that SAGE on 18 March would conclude that the epidemiological case was in place for the closure of schools“.251 There was declining school attendance.252 Ms Sturgeon noted that concerned parents were now “voting with their feet” by not sending their children to school.253 |
| 4.110. | On 18 March 2020, Ms Sturgeon and Mr Swinney decided schools should be closed in Scotland. The Scottish Cabinet was not consulted. Mr Swinney explained that there was no time to undertake any equality impact assessment about the closure of schools.254 He accepted that the Scottish Government did not consider alternatives to school closures at the time because of the “severity” of the situation.255 At about 14:00 that afternoon, before SAGE had met to agree its advice on school closures, Ms Sturgeon announced that “schools will close to pupils at the end of this week” and she could not promise that “they will reopen before the summer holidays“.256 |
| 4.111. | SAGE met later that afternoon, after decisions had already been taken to close schools in Scotland and Wales, to consider the modelling it had commissioned from SPI-M-O on 16 March 2020 on school closures.257 SPI-M-O had produced its ‘Consensus view on the impact of school closures on Covid-19’ the previous day. It stated that there was “a great deal of uncertainty around the extent to which children have a role in the transmission of SARS-CoV-2“.258 However:
“accounting for the policies announced on 16th March, and in the absence of school closures, NHS critical care capacity is likely or highly likely to be breached in the short to medium term … It is almost certain that school closures will not make the epidemic worse, and that they would reduce both the epidemic peak and expected number of cases. Our best assessment is that they would reduce the reproduction number by between 10% and 20% … School closures would need to last several months to maintain the effect seen.”259 SAGE therefore advised: “[A]vailable evidence now supports implementing school closures on a national level as soon as practicable to prevent NHS intensive care capacity being exceeded.”260 |
| 4.112. | SAGE also explained that the restrictions that had been implemented on 16 March 2020 should have a significant effect if compliance rates were good, but if they were not, then additional restrictions would be needed.261 However, reliable data on their impact would not be available for two to three weeks, which would be too long to inform decision-making as additional interventions to prevent NHS capacity being exceeded could be needed before then.262 It was known, therefore, only 2 days after the advisory lockdown was announced, that it would take up to 21 days for its impact to be properly assessed. SAGE also discussed the possibility of implementing further restrictions for London, given it “may be 1-2 weeks ahead of the rest of the country“.263 |
| 4.113. | Mr Cummings sent Mr Johnson a message at 15:42 from the SAGE meeting, stating:
“Am sitting in SAGE – not only they saying close all schools now but also London lockdown asap with some exceptions – but pubs etc closed by order of gvt by Fri pm … MAY BE ONLY WAY TO STOP LONDON NHS COLLAPSE IN 15 DAYS.”264 Professor Vallance said that this advice was driven by SAGE’s “concerns about the rapid doubling time and number of infections“.265 With a short doubling time, as Professor Whitty explained, “epidemics can expand from small numbers to very large numbers extremely rapidly“.266 Over a 30-day period, a doubling time of 3 days would generate 16 times as many cases as a doubling time of 5 days and almost 50 times as many cases as a doubling time of 7 days. Professor Whitty told the Inquiry: “Initially, SAGE had thought it would be possible to achieve control of Covid-19 (meaning R below 1) without school closures, but as the data on force of transmission emerged the collective view of SAGE changed.”267 |
| 4.114. | A COBR meeting was convened at 16:00 to consider SAGE’s advice on schools.268 At this meeting, Professor Vallance explained that London was approximately two to three weeks away from intensive care units being full and that, even if social distancing restrictions were increased, London remained at risk of exceeding this capacity.269 He told COBR that the advisory social distancing restrictions that had been put in place on 16 March 2020 had not led to “changes … at the rate needed” and that:
“the UK would be in a vulnerable position if it watched and waited for a further two weeks before implementing any additional social distancing measures. In order of the most to least effective, the following additional measures could be considered: closure of schools and colleges, closure of leisure facilities, closure of indoor workplaces and closure of non-essential retail.”270 Professor Vallance stated that modelling suggested school closures could potentially reduce Covid-19 cases by 10% to 15% and below the threshold for breaching intensive care unit capacity.271 |
| 4.115. | COBR agreed to “bring forward the Easter holidays for all schools in England, simultaneously with Northern Ireland and in line with Scotland and Wales” and that a “minimal school service” would be made available for the children of key workers and for vulnerable children.272 It also agreed that exams in England scheduled for May and June 2020 were to be cancelled.273 The UK government announced that day, 18 March 2020, that all schools, colleges and early years units in England would be closed from 20 March “until further notice“, although they would remain open for children of key workers and for vulnerable children.274 |
| 4.116. | The closure of schools had not been seriously contemplated in Northern Ireland prior to 12 March 2020, when the Republic of Ireland announced a package of measures that included the closure of schools, colleges and childcare facilities.275 The following day, Michelle O’Neill MLA, deputy First Minister of Northern Ireland from January 2020 to February 2022, called for the immediate closure of schools.276 At the Northern Ireland Executive Committee on 16 March, two separate votes on the issue divided along political lines.277 The Executive Committee ultimately decided to close schools as and when Professor McBride advised it.278 When it then became apparent that the UK government would close schools, according to Sir David Sterling, Professor McBride advised that “we should follow suit“.279 At the time, the Northern Ireland Office noted “cracks beginning to emerge in NIE [Northern Ireland Executive], with SF [Sinn Féin] wanting to follow Irish government particularly re school closures“.280 |
| 4.117. | Some witnesses questioned whether SPI-M-O models might have overestimated the impact of schools on the transmission of Covid-19.281 Professor Whitty told the Inquiry: “[T]here was so much uncertainty that school closures were the prudent approach.“282 According to Sir Gavin Williamson, the initial decision to close schools in England (as announced on 18 March 2020), was borne out of “quite a discombobulating sea change over a 24-hour period“, in which the focus shifted from keeping schools open to closing schools for most children.283 However, no government in the UK was adequately prepared for the sudden and enormous task of educating most children in their homes or for meeting the challenges and risks this presented. None had envisaged or prepared for the potential, complex ramifications of school closures on children’s lives. In Module 8: Children and young people, the Inquiry is considering the merits of the decisions to close schools to most children and the justification for this momentous step, as well as the range of impacts affecting children across society. |
Dashboard 05: 18 March 2020
Estimated population infected: 65,000–75,000 (awaiting SAGE confirmation)
Total confirmed cases UK: 2,626 (2,182 in England, 227 in Scotland, 149 in Wales and 68 in Northern Ireland)
Deaths: 103 (99 in England, 2 in Scotland, 2 in Wales and 0 in Northern Ireland)
Number of tests carried out: 46,842
Source: INQ000056058_0003
19 and 20 March: Additional restrictions
| 4.118. | On the evening of 18 March 2020, the situation in England remained on a knife edge. As Dr Warner pointed out to Professor Vallance and Cabinet Office officials that evening:
“[B]y the time the data shows we haven’t implemented strict enough measures it will be too late to stop an Italy like situation.”284 |
| 4.119. | Sir Simon Stevens and Mr Johnson met on 18 March 2020 to discuss NHS England resilience.285 The following day, COVID-19 Hospital Discharge Service Requirements was published in England, which stated that “hospitals must discharge all patients as soon as they are clinically safe to do so” and that this was “expected to free up at least 15,000 beds by … 27th March“.286 It explained that patients being discharged whose needs were too great to return home would be discharged to a care home.287 |
| 4.120. | The Coronavirus Bill had its first reading in the House of Commons on 19 March 2020.288 |
| 4.121. | Work continued in the UK government on a support pack for people who would be required to shield. At a meeting of the Covid-19 Strategy Ministerial Group on the morning of 19 March 2020, it was agreed that the Department of Health and Social Care and Professor Whitty should “finalise urgently today the categories of ‘clinically high risk’ people” who would be asked to shield.289 Mr Johnson confirmed that a decision on shielding should be delayed until the following day.290 |
| 4.122. | The meeting also discussed the possibility of further restrictions in London.291 Professor Vallance explained that “at the current rate of growth current ICU capacity would be reached in two to three weeks’ time“:
“[However,] the impact of measures on health outcomes would not be seen for two to three weeks. There was therefore an exact congruence between the point when the ICU capacity would be reached and when the government would know the effect of the current measures. A decision could not, therefore, be delayed.”292 Professor Vallance advised that, while school closures would help reduce R to 1, a “25% reduction in workplaces and a 75% reduction in face to face contact was needed to support that reduction“.293 Nonetheless, he explained: “[T]here was a lack of data on whether the UK was close to the 75% reduction … The data was inadequate, and unlikely to improve. If there was a perceived lack of compliance then the government would need to increase measures, in order of importance this would mean closing: leisure … non-essential retail; and workplaces.”294 |
| 4.123. | Mr Johnson acknowledged there was “an ongoing failure of compliance” and “the government must act that day“.295 He asked for a list to be drawn up of non-essential shops for closure and said a decision should be taken on whether this would apply only in London or across the UK.296 |
| 4.124. | Mr Johnson met Mr Khan later that day at about 13:30.297 It was agreed that they would “jointly announce at 5pm today that we would be saying that entertainment/hospitality and non-essential retail ‘must’ close from Friday [20 March] for two weeks” in London.298 |
| 4.125. | Mr Johnson, Rishi Sunak MP (Chancellor of the Exchequer from February 2020 to July 2022), Professor Whitty, officials and advisers met at about 15:00 to discuss the further restrictions that had been considered that morning.299 Mr Cummings sent Mr Cain a WhatsApp message from this meeting stating: “Get in here he’s melting down. Rishi says bond markets may not fund our debt.“300 Following this discussion, Mr Johnson decided not to proceed with London-specific measures at that time.301 |
| 4.126. | Mr Khan told the Inquiry that the joint press conference was cancelled at short notice with a view to further discussions taking place at COBR the following day, in light of concerns about the impact on financial markets.302 |
| 4.127. | An email that evening from a private secretary to the Prime Minister noted that the decision on London measures would be taken the following day and Mr Johnson “remained minded” to take these steps, but was keen for the announcement to be “made alongside further measures to support the economy, business and employees“.303 The Inquiry notes that the decision as to whether London should be locked down was considered more carefully and at greater length than the decision of 18 March 2020 to close schools. |
| 4.128. | At the 10 Downing Street press conference on 19 March 2020, Mr Johnson said that “we can turn the tide within the next 12 weeks” if there was collective action.304 Professor Whitty told the Inquiry that he thought that “this statement was very optimistic if it was taken to mean the path of the pandemic as a whole rather than a single wave“.305 |
| 4.129. | That same day, the Department of Health (Northern Ireland) published the Health and Social Care (NI) Summary Covid-19 Plan for the Period Mid-March to Mid-April 2020.306 The plan summarised the key actions to be taken by Health and Social Care (Northern Ireland) to ensure that there was sufficient capacity within the system to meet the expected increase in demand from patients contracting Covid-19 during this period. By this time, it had been identified that the normal capacity of 88 critical care beds in Northern Ireland “could be rapidly increased by a further 38 beds” by repurposing other facilities and opening additional beds.307 Capacity had been identified in designated wards in hospitals in Northern Ireland to treat roughly 280 adult inpatients with Covid-19.308 In anticipation of numbers increasing thereafter, Health and Social Care (Northern Ireland) trusts began to assess steps that could be needed to convert additional wards into areas to treat patients diagnosed with Covid-19.309 |
| 4.130. | On 19 March 2020, the Northern Ireland Executive Committee considered, for the first time, the application of the reasonable worst-case scenario to Northern Ireland. Setting out what this might mean in terms of the numbers of people who might die (without the application of interventions), Robin Swann MLA (Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024) told his Executive colleagues that the estimate was of 9,500 deaths – with 32,000 new cases per day – and commented that these were “scary numbers“.310 While the Department of Health (Northern Ireland) had previously set out the principles underlying the reasonable worst-case scenario, this had not been translated into Northern Ireland-specific figures.311 Mr Swann told the Inquiry that he could not explain:
“why it wasn’t in a previous briefing as to an exact number that was there. We worked out the reasonable worst-case scenarios and other scenarios were put out and presented as well, but I think it was at that point that that clarification of that … number that really brought things into a very sharp focus.”312 However, he had checked and the calculation had not been done prior to 19 March.313 Irrespective of who was best placed to perform this basic calculation, that it was not performed at all prior to 19 March demonstrates how very late it was that Northern Ireland ministers grasped the gravity of the situation they faced. |
Dashboard 06: 19 March 2020
Estimated population infected: 13,500
Total confirmed cases UK: 3,269 (2,756 in England, 266 in Scotland, 170 in Wales and 77 in Northern Ireland)
Deaths: 144 (135 in England, 6 in Scotland, 2 in Wales and 1 in Northern Ireland)
Number of tests carried out: 46,842
Source: INQ000055920_0002
| 4.131. | On 20 March 2020, SPI-M-O provided a consensus statement that concluded that doubling time based on intensive care cases was three to five days.314 This was significantly shorter than the five to seven days that SAGE had estimated on 18 March.315 It estimated that R was higher than had previously been thought and could be higher than 3.316 SPI-M-O advised that, if additional measures were not put in place, intensive care unit capacity would be likely to also be breached outside London.317 |
| 4.132. | That day, the Covid-19 Strategy Ministerial Group again considered whether further restrictions should be applied to London only or across the UK.318 Mr Johnson said that a decision needed to be made that day “to strengthen advice on social distancing” and on whether:
“measures to close pubs, bars and restaurants needed to be applied to the whole of the UK or London only … [and] what premises needed to close, including whether to close other shops“.319 Mr Johnson described his “instinct” during this discussion as being: “that it made no sense to impose measures on London alone. The capital is integrally connected with the rest of the South East, and for epidemiological purposes it seemed highly unlikely, to me, that it could be insulated from the rest of the Home Counties.”320 |
| 4.133. | Mr Johnson instructed the Cabinet Secretariat to provide him with final advice on further restrictions to reduce social gatherings and whether these restrictions should be applied in London or more broadly, so that he could take a decision on this shortly.321 He explained that they should prepare to convene COBR (should he decide to ask for businesses to close) and that they should consider inviting the devolved administrations and the Mayor of London, depending on the geographical extent of further restrictions.322 Shielding was again discussed, but it was decided that no shielding announcement should take place until a call centre and support package was in place, which should be achieved as soon as possible.323 Mr Johnson also asked Mr Hancock to lead work on the preparation of a “three month battle plan to tackle the virus” covering testing, technology, data gathering and interventions to be presented to him on 22 March 2020.324 |
| 4.134. | Mr Gove chaired the meeting of COBR convened at 16:00 on 20 March 2020.325 Mr Johnson told the Inquiry that he did not attend this meeting as he was about to do the press conference agreed earlier.326 Prior to the COBR meeting, there was consideration as to whether the devolved administrations should be invited.327 Ultimately, it was attended (via video conference) by Ms Sturgeon and Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021, as well as by Mr Drakeford (whose name is not recorded in the minutes).328 Professor Whitty explained that, as SAGE advised on 18 March 2020, the timescale for ascertaining evidence of the effectiveness of the restrictions previously implemented was approximately two to three weeks, although this was also the period within which the effects of the current outbreak would be felt significantly in intensive care units across the UK.329 |
| 4.135. | COBR considered a paper containing advice on further restrictions.330 It explained that, while it was “too early to judge compliance properly” with the restrictions already in place, early data were mixed, which meant that further measures might be necessary to increase compliance.331 The closure of certain businesses was proposed, including those the public had been advised on 16 March 2020 to avoid.332 Either businesses could be asked to close or this could be required by law.333 The aim was to reduce social distancing by the “75 per cent” necessary to bring demand within the capacity of intensive care units.334 The paper advised that the new restrictions should apply across the UK.335 |
| 4.136. | Professor Vallance explained that the objective of restrictions remained:
“to achieve a 75% reduction in household contacts, but it was now considered necessary to expand the range of interventions to achieve it“.336 Mr Johnson stated that these further restrictions: “were needed because there had not been full compliance with the previously announced advice … these enhanced measures would serve to enforce [social distancing]”.337 |
| 4.137. | COBR agreed that the businesses the public had been advised to avoid on 16 March 2020, including pubs, restaurants, cafes, cinemas, theatres and certain other places of leisure, would be required to close across the UK that night.338 It did so without the benefit of data on the impact on R of the advisory restrictions it had implemented on 16 March. Mr Gove explained that COBR could not wait to see compliance data as “the virus was spreading exponentially and the risk was that the NHS would be overwhelmed“.339 Decision-makers in the UK government, by waiting so long to implement the initial, more limited restrictions, had left themselves no time to allow for a two to three week period for the data concerning the impact of those measures to emerge. They had forced their own hand and the devolved administrations followed suit. |
| 4.138. | On the evening of 20 March 2020, Mr Johnson announced the immediate closure of pubs, cafes, restaurants and other places of leisure in England.340 Similar announcements about the closure of these businesses were made in Scotland, Wales and Northern Ireland.341 Laws requiring their closure, made under public health legislation, came into force the following day in England and Wales.342 These closures remained advisory in Northern Ireland and Scotland as the Coronavirus Bill, which created legal powers for use in those nations, had not yet been passed.343 Events had outpaced the Bill. |
| 4.139. | The intention of the restrictions implemented so far was to limit social contact, particularly among people aged over 70 or at particular risk from the virus. However, when Mr Johnson announced these further restrictions at the press conference, he immediately undermined the public health message of protecting those aged over 70 and the most vulnerable by stating that he hoped “to get to see” his mother that weekend for Mother’s Day.344 If, by his comments, Mr Johnson meant that he would see his mother remotely, he failed to say so at the press conference, leaving the impression that he would be seeing her in person. |
Dashboard 07: 20 March 2020
Estimated population infected: 177,000
Total confirmed cases UK: 3,983 (3,384 in England, 322 in Scotland, 191 in Wales and 86 in Northern Ireland)
Deaths: 177 (167 in England, 6 in Scotland, 3 in Wales and 1 in Northern Ireland)
Number of tests carried out: 55,092
Source: INQ000056076_0002
(The estimate of population infected reflected a change of estimate method to number of
deaths x 1,000.)
The weekend of 21 and 22 March 2020
| 4.140. | Over the weekend of 21 and 22 March 2020, concerns escalated about the sufficiency of existing measures to avoid the collapse of the NHS in England. The virus was spreading exponentially. The NHS Covid SitRep for 21 March indicated that there were 2,428 Covid-19 patients in hospitals across England.345 As Professor Ferguson explained:
“This 700-fold increase in hospitalised cases in over just two weeks partly reflects the approximately 4 doublings (16-fold) increase in the size of the epidemic, but also indicates the degree to which hospitalised cases were under-ascertained (i.e. missed) prior to full establishment of the NHS COVID Sitrep system.”346 |
| 4.141. | On 20 March 2020, England had 3,384 confirmed cases of Covid-19, while Scotland had 322, Wales had 191 and Northern Ireland had 86.347 |
| 4.142. | At the Covid-19 Strategy Ministerial Group meeting on 21 March 2020, Mr Johnson said that the UK was heading for an “Italy-style situation” unless the country could turn around the current situation. He suggested that the public “did not yet grasp this from the Government’s messaging“.348 He explained that he wanted to discuss whether the restrictions implemented the previous day were sufficient in light of data being presented or “whether prohibitions needed to be put in place that day“.349 |
| 4.143. | Professor Whitty advised:
“[T]here was some risk of ITUs [intensive treatment units] being overtopped if the Government did not do more, but there were also risks associated with further action.”350 |
| 4.144. | Sir Simon Stevens advised that the NHS was aiming to increase bed capacity.351 Professor Vallance explained that measures to increase NHS England capacity should mean it would not be overwhelmed.352 The worst-case scenario was that intensive care capacity in London would be overwhelmed in 9 days’ time, but the projection was that this would happen in 15 days’ time.353 |
| 4.145. | Mr Johnson concluded that “the situation remained dire and was getting worse“.354 It was agreed that a further discussion on bed capacity would take place at the Covid-19 Strategy Ministerial Group meeting on 23 March 2020.355 |
| 4.146. | Concerns about public compliance with social distancing continued over the weekend. Mr Shafi observed that 21 March 2020 was Snowdonia National Park’s “busiest visitor day in living memory“.356 Similarly, on 22 March, Eluned Morgan MS (Baroness Morgan of Ely), Minister for International Relations and the Welsh Language from December 2018 to October 2020, noted to Mr Drakeford that the Welsh seaside town of Tenby was “full of visitors” and “the Daily Mail is recommending the Welsh wilderness as a place to escape“.357 |
| 4.147. | In an email to Professors Vallance and Whitty sent on the evening of 21 March 2020, Professor Ferguson said he was “unconvinced we’re really seeing a 75% drop in contacts outside the household, at least this weekend“.358 He advised that it could be necessary to “consider some degree of enforcement of ‘stay at home’ recommendations“.359 |
| 4.148. | On 22 March 2020, a Covid-19 Strategy Ministerial Group meeting took place at 15:00. The Covid-19 Dashboard, updated at 14:00, was presented at this meeting. That day, for the first time, the Dashboard contained data on intensive care unit capacity in England (but not in Scotland, Wales or Northern Ireland).360 It outlined that occupancy had reached 80% of capacity in Greater London. It explained that “social distancing is happening but very likely not enough to prevent the virus growing“.361 Mr Hancock told the Inquiry that the data about intensive care unit capacity:
“demonstrated the need to rapidly enforce social distancing, which further supported the need for a legal lockdown rather than the advisory approach that had previously been taken“.362 Professor Whitty advised the meeting: “[I]t was unclear how people had responded to social distancing measures so far … 45% of people had changed their behaviour and … this needed to increase to 75% to be effective.”363 Mr Johnson stated that it was clear that “dramatic action to flatten the infection curve” was needed.364 It was agreed that messaging would be worked up for 24 March which emphasised that “people should not leave their homes unless absolutely necessary“.365 |
| 4.149. | A further meeting of the Covid-19 Strategy Ministerial Group was held at 17:30. A paper drafted by Professor Whitty presented at the meeting explained that, in addition to direct deaths from Covid-19, excess mortality would arise from Covid-19 in a number of ways:
|
| 4.150. | At the meeting, Mr Johnson was provided with a draft version of the Department of Health and Social Care’s COVID-19 Response – health & social care 3 month battleplan to tackle the virus and protect life.367 This estimated that between 12,500 and 15,000 hospital beds across England could be freed by postponing non-urgent elective operations and that, potentially, 15,000 acute beds could also be freed up.368 It was agreed that the Department of Health and Social Care should clarify that non-elective surgery would stop in England in mid-April 2020.369 |
The lockdown decision: 23 March 2020
Dashboard 10: 22 March 2020
Estimated population infected: 281,000 (calculated using SAGE assumption that actual infections = 1,000 x deaths)
Total confirmed cases UK: 5,683 (4,792 in England, 416 in Scotland, 347 in Wales and 128 in Northern Ireland)
Deaths: 281 (257 in England, 10 in Scotland, 12 in Wales and 2 in Northern Ireland)
Number of tests carried out: 78,340
Source: INQ000056000_0002-0003
Figure 12: Daily confirmed cases from 1 to 23 March 2020 across the UK
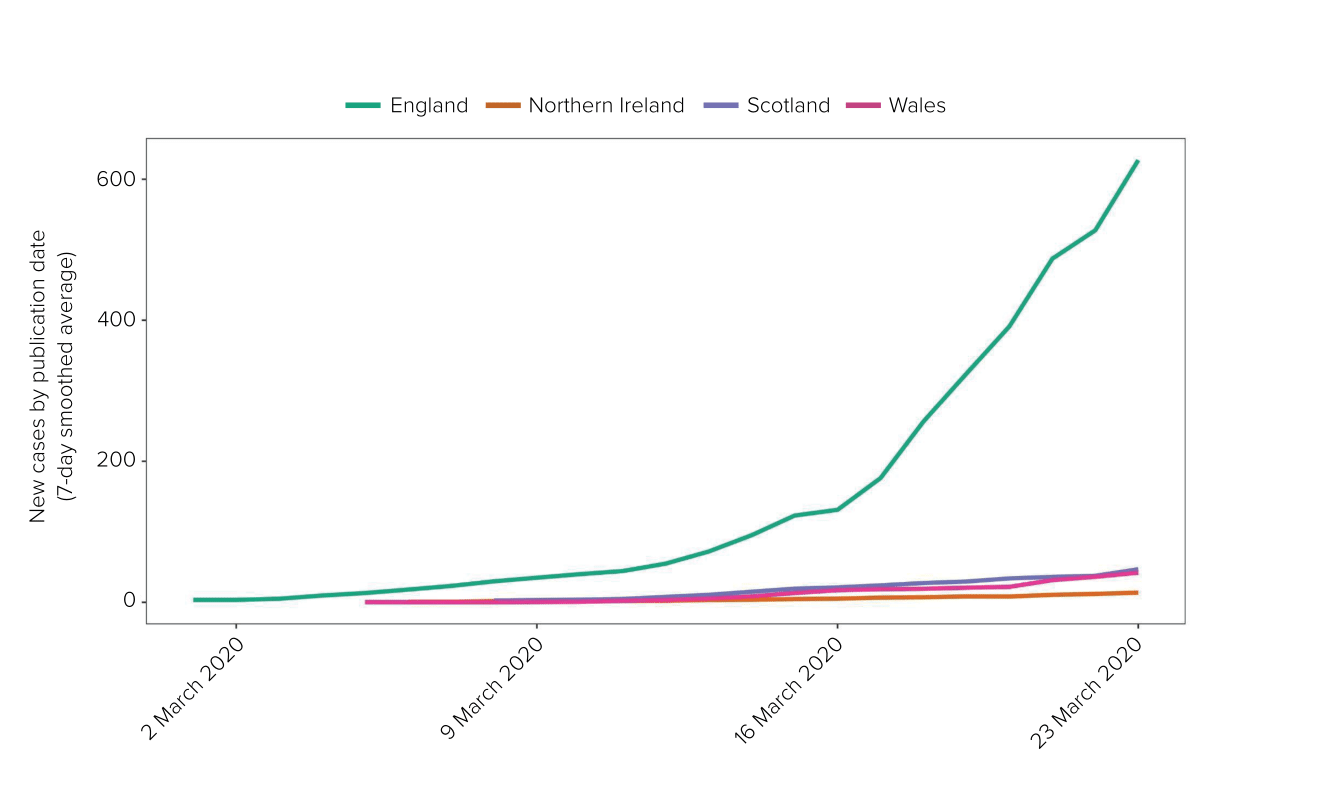
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 4.151. | SAGE met on 23 March 2020. It considered two urgent papers produced by the Scientific Pandemic Insights Group on Behaviours (known as SPI-B) the previous day. The first analysed the current level of adherence among the population to the advisory restrictions in place. It concluded: “[T]here appears to be room for social distancing to be increased still further.“370 The second outlined options for improving adherence further.371 |
| 4.152. | SAGE also discussed a SPI-M-O consensus statement on the Covid-19 outbreak in the UK as at 20 March 2020.372 The statement advised that modelling now suggested that the doubling time of cases in intensive care units “is short, ranging from 3 to 5 days“.373 Intensive care capacity would be exceeded in London “by the end of the month, even if additional measures are put in place today“.374 It explained that the rest of the UK was “1-2 weeks behind London” and, in the absence of additional measures “being put into place in the next few days, it is likely that we will breach ICU capacity in other regions“.375 It stated:
“Any measures enacted would take 2-3 weeks to have an impact on ICU admissions; school closures will take 1-2 weeks longer.”376 |
| 4.153. | SAGE concluded that the epidemic growth rate was faster than previously anticipated, with the doubling time estimated to be three to four days.377 High rates of compliance with social distancing measures would be needed to reduce R below 1 and to bring cases within NHS capacity.378 However, SAGE highlighted that there was uncertainty about whether there was the necessary compliance with social distancing needed to bring the epidemic within NHS capacity and that public polling over the weekend indicated there was room for improvement on compliance rates.379 |
| 4.154. | On 23 March 2020, the Technical Advisory Cell in Wales also recommended consideration of “an immediate ‘lockdown and release’ approach“.380 On 22 March, following a meeting with Mr Drakeford and Mr Gething, officials in Wales had been tasked to “prepare first cut [of a lockdown plan] so that we are ready either to respond to [the UK government] or move separately“.381 |
| 4.155. | A Covid-19 Strategy Ministerial Group meeting was held at 09:15 on 23 March 2020, chaired by Mr Johnson and attended by Mr Sunak, Mr Hancock, Mr Gove, Professor Whitty, Sir Simon Stevens and others.382 Sir Simon Stevens explained that intensive care ratios in London had been increased from 1:1 to 1:8 and that it might not be sustainable for the NHS in London to continue to operate under this strain.383 He said:
“It was important not to be falsely reassured by the fact that hospitals were coping at the time. The NHS was doing well, but the numbers of those needing critical care would follow an exponential path. It was likely that the NHS would be overburdened.”384 Professor Whitty advised: “[E]mergency brake measures were needed now to get control of the immediate situation, but it was likely that the measures already in place would be sufficient in the longer term.”385 Mr Johnson concluded that the UK government’s advisory restrictions “did not seem to be working, and a stronger approach was needed“.386 He stated that the government should, that day, instruct people to stay at home unless they were in a specified occupation or could not work from home.387 People should only leave home to shop for necessities and to attend medical appointments, and social gatherings of any kind should be stopped.388 This should be reinforced with fines.389 Mr Johnson explained that this announcement was: “within the scope of the original plan to introduce more distancing as and when required, and so should not be couched as a big step change. Actions were being forced by the pace of events.”390 |
| 4.156. | At 09:45, a second Covid-19 Strategy Ministerial Group meeting was held.391 Two papers on further restrictions were considered.392 One paper stated:
“Social distancing is happening, but it is uncertain whether there is a sufficient level of compliance to prevent infections growing exponentially … In light of this uncertainty about the level of social distancing, and hence whether current measures are sufficient to push the reproduction number below 1 and therefore contain the spread, the Government may wish to take further steps to increase social distancing.”393 The other paper explained that decision-makers needed to decide that day whether, to drive R below 1, the existing social distancing advice should now be enforced by law and the public told to stay at home.394 It was decided that the public should be informed to stay at home unless shopping for necessities, attending a medical appointment, daily exercise, or if it was not possible for them to work from home.395 Non-essential retail should also be closed. It was agreed that Mr Johnson would announce this that evening.396 Mr Johnson told the Inquiry that he “no longer had the luxury of waiting … it was over“.397 |
| 4.157. | At about 11:30 on 23 March 2020, Professor Van-Tam emailed Professors Whitty and Vallance and explained that participants in SPI-M-O were “seriously alarmed” and “of one mind that extra measures [were] needed right now – right across the country not just London“. He stated that, even with extra measures, intensive care capacity in London would be “overrun“, but the measures “might just avoid overrunning in the rest of England, but only just“.398 Professor Whitty assured him that “ministers are fully seized of the need to act“.399 |
| 4.158. | At 17:00 on 23 March 2020, Mr Johnson chaired a COBR meeting by video link.400 The First Ministers of Scotland and Wales, as well as the First Minister and deputy First Minister of Northern Ireland, were present.401 A paper was presented which recommended COBR agree to:
These measures were to be mandatory and enforced by law. COBR was advised that the restrictions should be announced that night, with clear guidance published immediately after the announcement, and that arrangements for enforcement should be clarified and come into force later that week.403 |
| 4.159. | Professor Vallance explained:
“[T]he current rate of infection by a single person was 2.6-2.8 and this doubled in Intensive Care Units. The rate was doubling every three to five days which was similar to Italy, Germany and Spain.”404 Mr Johnson noted that “measures needed to be taken as social distancing was not being adhered to at present“.405 While some activities had reduced (eg ‘high street’ by 28%, travel by 60% and socialising by 52%): “[P]ark attendance had gone up by 200 per cent and queues in shops had increased. There were regional differences and showed lower compliance rates in some areas outside London.”406 |
| 4.160. | COBR agreed that Mr Johnson and the devolved administrations would announce the recommended restrictions that evening with immediate effect.407 Mr Johnson noted that, given the sensitivities of the discussion, it should remain confidential until the announcements were made that evening.408 The decision to impose a mandatory lockdown was not approved by the UK Cabinet, which, as outlined in Chapter 5: Exit from lockdown, in this volume, did not meet to discuss this decision until the day after it had been announced publicly.409 |
| 4.161. | That evening, Mr Johnson made a televised address. He told everyone: “You must stay at home.“410 All non-essential retail in England was closed with immediate effect. Social and religious events, including weddings and baptisms, were prohibited. Public gatherings of more than two people were banned.411 The First Ministers of Scotland and Wales made parallel announcements.412 The lockdown was not announced in Northern Ireland until the following day.413 |
Dashboard 11: 23 March 2020
Estimated population infected: 281,000 (calculated using SAGE assumption that actual infections = 1,000 x deaths)
Total confirmed cases UK: 6,650 (5,585 in England, 499 in Scotland, 418 in Wales and 148 in Northern Ireland)
Deaths: 335 (303 in England, 14 in Scotland, 16 in Wales and 2 in Northern Ireland)
Number of tests carried out: 83,945
Source: INQ000120846_0002-0003
| 4.162. | The lockdown was given legal effect in England, Wales and Scotland on 26 March, and in Northern Ireland on 28 March 2020.414 |
| 4.163. | Mr Drakeford told the Inquiry that it was “likely that the Chief Medical Officer for Wales conveyed the view … in advance of the COBR meeting, as he was with me at that point“, that a lockdown was necessary by this point. He believed this was also the view of the rest of the Welsh Cabinet.415 Ms Sturgeon noted that the scientific advice and modelling meant a lockdown at this time was the only option “realistically open to decision-makers“.416 |
| 4.164. | Sir David Sterling described the decision as:
“effectively a fait accompli. The Executive was not involved in any meaningful way in the UKG [UK government] decision-making process. In those early days I do not recall the CMO ever suggesting the [Northern Ireland] Executive should follow a different path and I also have no recollection that ministers ever seriously questioned the UKG’s decisions.”417 He also acknowledged that “Northern Ireland could not have moved into a lockdown before the UK did“.418 The Executive Committee had not been advised that a lockdown was necessary in Northern Ireland prior to 23 March 2020, nor had it had any detailed discussion about the prospect of a lockdown or scrutinised any departmental plans for this eventuality.419 Nonetheless, Professor McBride told the Inquiry that he considered that the situation was extremely serious and required a significant additional response.420 Both Ms O’Neill and Baroness Foster readily agreed with the proposition that Northern Ireland was “woefully unprepared” for going into a lockdown.421 NICCMA had only come into effect on 18 March 2020 and, by this point, government departments had not instituted detailed cross-government planning in preparation for a lockdown.422 |
Decision-making leading to the lockdown decision
| 4.165. | The lockdown decision of 23 March 2020 was as difficult a decision as any UK government or devolved administration has ever had to make. The highly polarised views in the public domain on the merits of the lockdown decision are testament to the complexity and unprecedented nature of the decision and the intensely difficult balance that had to be struck by the UK government and devolved administrations. |
| 4.166. | Each government was entitled to decide how to attempt to weigh the public health benefits of a lockdown against the social, economic and educational harm that would ensue. However, their task was made a great deal harder by inadequate planning, inadequate data and the absence of a coherent strategy. |
Flawed planning
| 4.167. | The decision to impose a UK-wide lockdown was remarkable for the failure on the part of the four governments to anticipate and plan effectively for the possible need for a mandatory lockdown or to engage in any kind of anticipatory debate over the merits and consequences of such a restriction. As Professor Mark Woolhouse (Professor of Infectious Disease Epidemiology at the University of Edinburgh) observed, the imposition of a lockdown “was not part of the UK’s pandemic preparedness planning at all“.423 He was “particularly concerned there was no concerted effort to come up with policy options that would have kept us out of lockdown“.424 Professor Vallance explained that lockdown “was always possible, in theory, in the UK but had never really been considered in any detail before the Covid-19 pandemic“.425 |
| 4.168. | The initial plan to respond to Covid-19 by slowing the spread of the disease, as articulated in the Coronavirus: Action Plan and pursued by the four governments until 16 March 2020, was inherently flawed. |
| 4.169. | That plan was partly based on the mitigation plan set out in the UK Influenza Pandemic Preparedness Strategy 2011 (the 2011 Strategy).426 As the Inquiry concluded in the Module 1 Report, a major flaw in the 2011 Strategy was the assumption made that widespread infection could not be prevented and the role of government was limited to taking measures to slow the spread of the disease, pending the discovery of therapeutics or vaccines.427 As such, it envisaged the use of a limited set of restrictions to slow, rather than stop, the spread. |
| 4.170. | However, the assumption in the 2011 Strategy that the spread of an influenza pandemic could not be stopped was based on influenza’s short generation time of one to two days. In this scenario, the capacity of test and trace services would likely be overwhelmed, particularly as case numbers continued to grow and infected people would likely have already passed on the virus by the time they were tested and isolated. Covid-19, however, was a different illness, slower moving but more deadly, and, unlike pandemic influenza, it was often transmitted by people without symptoms. By 3 February 2020, its generation time was estimated to be longer than influenza at six to seven days on average.428 |
| 4.171. | Despite the epidemiological differences between pandemic influenza and Covid-19, the plan for the delay phase of the Covid-19 response continued to be predicated on slowing rather than preventing the spread of the virus.429 |
| 4.172. | SAGE had advised on 28 January 2020 that “pandemic influenza infection control guidance should be used as a base case and adapted“.430 Professor Anthony Costello, Professor of Global Health and Sustainable Development at University College London, told the Inquiry that, from this point:
“[T]he UK advisory die was cast. The UK medical and scientific group of experts saw it as a flu epidemic. In their view there was nothing the UK could do to stop it, only manage its progress to protect the NHS.”431 As such, Professor Costello explained: “[T]heir strategic and management decisions would draw upon a blinkered plan for the wrong virus: influenza, not a coronavirus.”432 |
| 4.173. | Decision-makers should have taken into account epidemiological differences between influenza and Covid-19 and considered whether, in light of these, a response to Covid-19 limited to slowing the spread of the virus was appropriate. |
| 4.174. | To the limited extent that decision-makers considered prior to mid-March whether stopping the spread through the use of restrictions would be feasible, they were advised by scientists that this would lead to an exit wave of infections later in the year when restrictions were lifted.433 It was assumed that putting stringent restrictions in place – in the absence of effective treatments for the virus or a vaccine – would inevitably postpone the wave of infections until a time later in the year when the NHS would already be under strain from seasonal illnesses. This is why the initial plan anticipated building up immunity in the population through a single wave of infection in the spring and summer of 2020, as a potential means of bringing the pandemic to an end if, ultimately, a vaccine did not become available. |
| 4.175. | Yet there could have been an alternative. As Professor Halpern told the Inquiry:
“The world – and more specifically Asian countries – had found another strategy: to build sophisticated test and trace systems strong enough to suppress the virus, at least for long enough to enable treatment and vaccines to be developed.”434 |
| 4.176. | The UK did not have a test and trace system at the start of 2020 that could be scaled up quickly. The ability to scale up diagnostic testing requires advance planning and resources. As Professor Whitty observed: “[It] cannot simply be switched on from a standing start once an emergency has begun.“435 As noted in the Inquiry’s Module 1 Report, the UK’s testing and contact tracing system at the start of the pandemic was:
“designed to deal only with small numbers of cases of emerging infectious diseases, as opposed to mass testing or contact tracing … The UK government and devolved administrations could and should have invested in this infrastructure in advance of the Covid-19 pandemic, but had not done so.”436 |
| 4.177. | The UK government and devolved administrations did not have in place adequate plans for manufacturing and laboratory facilities to be increased. Other countries were not so ill-prepared. South Korea, for example, was able to scale up and deploy testing and contact tracing as a result of prior experience and investment, particularly as a result of Middle East respiratory syndrome (MERS).437 Professor Whitty told the Inquiry that the UK had “much to learn” from other countries in this respect.438 |
| 4.178. | As a result of the lack of testing capacity, community testing had to be stopped and distribution of the tests restricted to those considered to be most in need. Not surprisingly, the virus continued to spread. Furthermore, little thought was then given to the possibility of putting stringent restrictions in place for a period of time to stop the spread and drive down infections, during which time test and trace capacity could have been increased to contain the exit wave. |
| 4.179. | As Dr Warner told the Inquiry, plans for stringent restrictions should have been worked up from the outset so they were available if they were needed.439 They were not. There was, therefore, no plan for the four governments to fall back on when it became apparent that stringent restrictions were necessary. |
| 4.180. | The absence of planning was further exemplified by the lack of an exit strategy from lockdown. Since the possibility of a prolonged period of mandatory lockdown was never contemplated in the initial plan, no thought had been given to a strategy for exiting a lockdown once one was imposed. Yet even when it became clear over the weekend of 14 and 15 March 2020 that a prolonged period of lockdown was distinctly likely, decision-makers did not direct work to begin on an exit strategy. |
| 4.181. | While a full exit strategy with identified milestones would not have been realistic, consideration should have been given prior to the implementation of the mandatory lockdown as to which tests would need to be met to exit the lockdown, as well as how the pandemic could ultimately be brought to an end. This would have enabled operational planning to be targeted towards creating those conditions. |
| 4.182. | While the Inquiry acknowledges the pressure that all four governments must have faced in the lead-up to the mandatory lockdown, given that no planning for that eventuality had previously been done, they should have made arrangements for work to commence on options for an exit strategy when a prolonged lockdown became a distinct possibility over the weekend of 14 and 15 March 2020. Instead, work on how the lockdown should be eased did not begin until 20 March 2020 in England, 6 April in Wales, mid-April in Scotland and 20 April in Northern Ireland. |
Inadequate guidance and restrictions before 16 March 2020
| 4.183. | One of the most effective ways to limit the spread of a virus (and therefore to avoid the need for stringent restrictions on the public) is to persuade members of the public to take their own precautions. However, as the virus spread during March 2020, the initial advice to the public was weak. It focused on hand hygiene and little else. Face masks were positively discouraged for the public, mass gatherings continued to take place, thereby reinforcing the message that close social contact was approved, and Mr Johnson’s optimistic nature frequently undermined the serious message he was meant to convey. In the Inquiry’s view, members of the public should have been trusted and advised to take their own precautions at a much earlier stage. |
| 4.184. | The first significant restriction to slow the spread of Covid-19 was not implemented until 12 March 2020 (self-isolation advice). On 16 March, an advisory lockdown was put in place and gradually tightened over subsequent days, including by the closure of schools, until a mandatory lockdown was announced on 23 March (although it was not given legal force until a few days later). |
| 4.185. | Restrictions were implemented too slowly by the four governments, allowing the virus to spread to the point when the imminent collapse of health services in parts of the UK left the governments believing that they had no alternative but to impose a UK-wide mandatory lockdown. |
| 4.186. | Professor Woolhouse’s view was that more proportionate and sustainable interventions (such as contact tracing, self-isolation, face coverings and respiratory hygiene) should have been introduced “as early as March 4th“.440 He stated that, if at least some of the “substantial interventions” brought in during the week of 16 March 2020 had been introduced earlier, the need for a full lockdown could have been avoided: “[M]y maxim is: if you go early, you don’t have to go so hard.“441 |
| 4.187. | Mr Johnson told the Inquiry that he thought it was “highly unlikely” that the imposition of earlier restrictions would have avoided a lockdown.442 However, had stringent restrictions short of a mandatory lockdown been introduced earlier than 16 March 2020 – when the number of Covid-19 cases was lower – the mandatory lockdown might have been shorter or, conceivably, avoided entirely. At the very least, there would have been time to establish what the effect of those restrictions on levels of incidence were and whether there was a sustained reduction in social contact. This would have enabled the governments to assess whether stringent restrictions short of a lockdown would suffice to prevent health services across the UK being overwhelmed and whether they were therefore a feasible policy option. |
| 4.188. | The reality is that the UK government and devolved administrations, through their slow responses in late February and early March 2020, denied themselves the possibility of being able to make that assessment. In effect, the likelihood of a mandatory lockdown significantly increased as a result of the failure to act more speedily before 16 March. That more stringent restrictions were not implemented before 16 March was the result of failures on the part of decision-makers, senior officials and scientific advisers. |
Failure of decision-makers to identify sufficiently specific objectives
| 4.189. | Over the weekend of 14 and 15 March 2020, it became apparent that the UK government was not willing to run the risk of the NHS collapsing, given the significant additional deaths that would result. However, prior to this, the outcome the four governments sought to achieve by implementing restrictions was not sufficiently specific to enable scientific advice to be provided on the options to achieve that objective. |
| 4.190. | As late as 20 February 2020, SAGE was still seeking clarity as to the objectives of the UK government’s response, in order properly to advise on which restrictions could be implemented to achieve them.443 Professor Vallance told the Inquiry that there were attempts “several times” to try to define a mortality number that the UK government was willing to tolerate as part of its initial plan for the response, but that “nobody would give that number“.444 |
| 4.191. | The Coronavirus: Action Plan of 3 March 2020 simply indicated that slowing the spread would have a beneficial outcome for the NHS since “health services are less busy in the summer months“.445 While the lack of specificity in the Action Plan might have been understandable as a communications document, there was no detailed internal plan containing the specific objectives of the response of the four governments. These objectives were necessary to inform scientific advisers of the extent of the pressure decision-makers sought to ease on the NHS in order to enable them to identify – and advise decision-makers of – the point at which restrictions needed to be imposed. |
| 4.192. | Instead, scientific advisers were forced to provide advice about restrictions on the basis of their ability to “flatten” the peak generally, but without an appreciation of what the UK government’s ‘red lines’ were in terms of numbers of infections or deaths, or the extent of the stringency of restrictions which the four governments would be willing to tolerate. |
| 4.193. | Professor Edmunds told the Inquiry that, because modellers on SPI-M-O did not know whether lockdowns were “politically acceptable“, they “did not spend as much time on them in early March as we should have“.446 The lack of clarity about what the governments were seeking to achieve “may well have led to SAGE advice being too timid, particularly in the early days of the epidemic“.447 Professor Ferguson stated:
“[P]reventing the NHS from being overwhelmed only became apparent (to me at least) as a clear government red line from 13th March onwards.”448 |
Flawed scientific advice about the timing of restrictions
| 4.194. | Until the weekend of 14 and 15 March 2020, Professors Whitty and Vallance advised that restrictions should not be implemented until closer to the peak of infections.449 This was, in part, due to their concerns about the severity of the indirect public health, social and economic impacts that the restrictions would have and, therefore, an understandable desire to limit the time the restrictions would be in place.450 However, it was also due in part to a concern that, since high compliance with restrictions during the peak was essential to reduce the strain on the NHS, restrictions should not be implemented too soon in case the public tired of complying with them before this point. |
| 4.195. | This notion of ‘behavioural fatigue’ was introduced by Professor Whitty.451 Mr Johnson told the Inquiry that Professor Whitty advised him in late February 2020:
“[T]here were limits to human patience, to the willingness of the population to do as they were told. That is why it was so essential to get the timing right. If you went too early, for instance, you might have to sustain restrictions for longer than people could endure.”452 Professor Whitty said that he was “rightly told off by my behavioural science colleagues” for using the terminology ‘behavioural fatigue’. He confirmed that it did not arise from SPI-B.453 |
| 4.196. | Professors Whitty and Vallance both told the Inquiry that concerns about behavioural fatigue did not influence their advice about the appropriate time to implement restrictions.454 However, on a number of occasions prior to mid-March 2020, both advised that restrictions should not yet be implemented for this reason.455 |
| 4.197. | Regardless of whether it was due to concerns about public compliance or the political will to sustain restrictions over a prolonged period, Professors Whitty and Vallance were clearly worried that restrictions might not be sustainable if implemented too early. They advised that restrictions should be implemented closer to the peak of infections.456 |
| 4.198. | As Mr Cummings pointed out to Mr Johnson on 14 March 2020, the scientific advice received prior to that point that decision-makers should not yet implement restrictions had been based only on the ‘time to peak’ rather than on the ‘time to NHS collapse’.457 |
| 4.199. | Scientific advisers had not appreciated the likelihood of the NHS being overwhelmed before then because of a lack of data in two areas:
Robust modelling on the likely impact of the virus on the NHS in England only became available following the meeting between NHS England and modellers on 1 March 2020. It was only then that it became clear that the NHS in England would be overwhelmed if the reasonable worst-case scenario materialised. |
| 4.200. | As a result, the need to implement stringent restrictions as a matter of urgency was underestimated by scientific advisers until 13 March 2020, when the real risk of imminent NHS collapse in England became apparent. |
| 4.201. | Professor Vallance observed that the lack of data “was detrimental to both the science advice and the political decision-making“.460 He conceded that scientific advice was:
“trying to be too precise in terms of the idea of an optimal timing of interventions“.461 He told the Inquiry: “[T]he focus on trying to get that timing exactly right was incorrect. It was an error to think that you could be that precise. That’s a really important lesson that came out of this … you need to go early.”462 Professor Whitty said that the 16 March 2020 restrictions should have been implemented “several days earlier“.463 |
| 4.202. | The Inquiry acknowledges the difficulties facing the UK government’s scientific and medical advisers. They were working under extreme pressure and in conditions of evidential uncertainty. However, they were aware that the absence of adequate data was likely to mislead as to the true extent of infection and the resulting impact on health services. Prior to 13 March 2020, they knew that they likely did not have an accurate understanding of the point at which the NHS would be overwhelmed. Accordingly, they should not have advised decision-makers up to mid-March that restrictions should not yet be implemented. At the very least, they should have made clearer to decision-makers the higher level of risk for the NHS that would arise from following that scientific advice, given the data gaps and assumptions on which it was based. In particular, Professor Whitty should have made clearer to decision-makers that his advice that public compliance with restrictions might wane if restrictions were implemented too early (the notion of ‘behavioural fatigue’) was based on an assumption he had made – and therefore could prove to be incorrect. He should have made it clearer that a decision to wait longer before implementing restrictions based on that assumption would therefore entail running certain risks in relation to NHS capacity. |
Failure of decision-makers adequately to interrogate scientific advice
| 4.203. | Decision-makers in all four governments relied on the scientific advice before the weekend of 14 and 15 March 2020 that social distancing restrictions should not be implemented until closer to the peak of infections.464 Mr Johnson explained that, prior to that weekend:
“[T]he scientific advice was that the measures that were necessary to delay and flatten the virus’s peak and to reduce pressure on the NHS should not be brought in too early because this would risk behavioural fatigue and a greater second peak.”465 |
| 4.204. | Mr Johnson told the Inquiry that he had not challenged the scientific advice to wait longer before implementing restrictions, despite “thinking there was something amiss“, given that this advice did not seem to be consistent with the graphs presented at COBR on 12 March 2020.466 The graphs indicated that the NHS would be overwhelmed in the reasonable worst-case scenario, even if all the restrictions were subsequently implemented. |
| 4.205. | Mr Hancock, Mr Sunak and Mr Gove all said the UK government accepted scientific advice that restrictions should not be implemented too early.467 |
| 4.206. | Mr Drakeford similarly explained that he had been advised by the Chief Medical Officer for Wales:
“[I]f you go too soon, you may lose the impact that you’re looking for, because people won’t be convinced … and the compliance may not follow up a level that you need.”468 |
| 4.207. | Ms Sturgeon confirmed:
“[T]here was a concern that introducing restrictions too early might limit their effectiveness should compliance have waned before optimal timing.”469 |
| 4.208. | This advice also influenced ministers in Northern Ireland. On 12 March 2020, Ms O’Neill raised the issue of whether Northern Ireland should introduce a similar set of restrictions (including school closures) to those introduced in the Republic of Ireland. Ministers were advised that there was “no medical/scientific evidence” to support the measures announced by the Government of Ireland and that there was a risk of creating a peak too early.470 Even as late as 16 March 2020 – the day an advisory lockdown was implemented across the UK – Mr Swann recorded in a note he made during a meeting of the Northern Ireland Executive Committee that restrictions:
“[h]ave to be sustainable – if introduce too early can’t sustain. What is best decision to take? Now is not right time to do it.“471 |
| 4.209. | Decision-makers and senior officials in all four governments failed adequately to interrogate the potential policy consequences of the scientific advice on which they relied in relation to the timing of the implementation of restrictions prior to the weekend of 14 and 15 March 2020. They should have done so to ensure that they understood the potential consequences for their healthcare systems of following the scientific advice to wait longer before implementing restrictions, given the incomplete data, uncertainties and scientific assumptions on which that advice was based. They could then have decided whether – in light of the potential policy consequences for their healthcare systems – they should follow the scientific advice or adopt a more cautious approach. Given the near collapse of health services in northern Italy, it was obvious that there was a high risk of health services in the UK being similarly overwhelmed if they did not act urgently. |
An earlier mandatory lockdown
| 4.210. | Over the weekend of 14 and 15 March 2020, it had become obvious to UK government decision-makers that much more stringent measures would have to be imposed in order to bring R below 1 and avoid the NHS in England being overwhelmed. The need for the ultimate intervention – an urgent mandatory lockdown – was openly debated. However, the package of measures that was agreed should be taken to COBR on Monday 16 March – and which was publicly announced later that day – did not expressly include taking such a step. The restrictions announced were advisory and did not constitute a mandatory lockdown. For example, there would be no compulsory closure of bars, restaurants, gyms or non-essential workplaces.472 Further, schools and retail would not be required to close. |
| 4.211. | Mr Hancock told the Inquiry that, although “no one called [the package of measures announced on 16 March 2020] a lockdown, that is what it was“.473 Professor Vallance explained that the package announced was “close to … a national lockdown, albeit one that was … advisory rather than mandatory“.474 The question of whether to implement a mandatory or advisory lockdown had been “a political issue, not a scientific one“.475 |
| 4.212. | There were a number of reasons why an advisory, rather than mandatory, lockdown was implemented on 16 March 2020. |
| 4.213. | Firstly, there was a desire to find the minimum level of restrictions that could reduce R below 1 by gradually increasing the stringency of the restrictions and monitoring their effect. It was hoped that an advisory lockdown might be sufficient if public compliance was high.476 As Professor Whitty told the Inquiry:
“[T]he real question … was what was the minimum set of interventions which could realistically move R from being above 1 to below 1 … Nobody wanted to introduce more restrictive interventions than necessary due to the very high social and public health cost of the interventions.”477 Mr Johnson suggested that, rather than “rushing in“, a period of 10 days was necessary while decision-makers and scientific advisers: “closely monitored the available data, considered alternatives and worked out when and how best to impose the lockdown“.478 |
| 4.214. | Secondly, the full operational planning to enable a mandatory lockdown to be implemented and enforced was not in place on 16 March 2020. For example, the Coronavirus Bill had not yet been passed and economic support packages, including furlough, were still being worked up. Even shielding, which had always been envisaged under the initial plan, was not ready to be implemented. As late as 19 March, the UK government had not yet finalised the categories of clinically high-risk people who would be advised to shield.479 There were also practical issues to be resolved in Scotland in relation to shielding, and, by 18 March 2020, there were no real plans for implementing shielding in Wales.480 |
| 4.215. | Thirdly, according to Mr Cummings, part of the reason a mandatory lockdown was not announced until 23 March 2020 was that Mr Johnson oscillated between alternative policy options from 16 to 23 March. He explained that Mr Johnson:
“backed and veered from supporting a lockdown to being incredibly concerned about the prospect of ordering a lockdown“.481 |
| 4.216. | Mr Johnson described his concern about ordering a lockdown as:
“an indication of the cruelty of the choice that we faced, and the appalling balancing act that I had to do throughout the pandemic“.482 It is wholly understandable that Mr Johnson should have wrestled with such a profound decision. Nevertheless, in the face of a virus that is spreading exponentially, failure to take early and decisive public health action is likely to have dire consequences. |
| 4.217. | By failing to take effective action at an earlier stage, the four governments left themselves insufficient time in which to determine whether the advisory measures would work. |
| 4.218. | The virus kept spreading and the threat to the healthcare systems of the four nations kept growing. By 23 March 2020, in the face of exponential spread and less than hoped-for levels of compliance, decision-makers could not afford to wait any longer. |
| 4.219. | The failure to announce a mandatory lockdown until 23 March 2020 meant that it was imposed at a higher and later stage of each nation’s epidemiological wave, thereby guaranteeing higher levels of mortality and reducing the ability of the measure to bring R down. Professor Edmunds stated that the one-week delay “almost certainly led to thousands of additional deaths“.483 Professor Ferguson told the Inquiry that in later work which analysed the impact of restrictions in England:
“we explicitly modelled the counterfactual scenario of moving the lockdown of 23rd March back to 16th March, and estimated mortality … would have been reduced by 48%“.484 That could have equated to a reduction in deaths in England from 48,600 to approximately 25,600 in the first wave up to 1 July 2020.485 |
| 4.220. | Moreover, because the lockdown was imposed at a relatively late stage of the epidemiological cycle, when the levels of incidence were higher, a longer lockdown was required to bring down R0. |
| 4.221. | Many witnesses – including Professor Vallance, Professor McLean, Mr Hancock, Sir Christopher Wormald, Mr Cummings and Mr Cain – also told the Inquiry that a mandatory lockdown should have been implemented earlier than 23 March 2020.486 Professor Whitty acknowledged:
“With the benefit of knowing what transpired and the ability retrospectively to piece together the timeline by which seeding of infection from Europe to the UK resulted in an upswing in domestic transmission, the first lockdown, and the various steps that led up to it, should have been implemented earlier. How much earlier is more debatable, but probably at least seven days.”487 Mr Gove stated that he had believed that it would have been appropriate to impose a lockdown during the week of 16 March 2020. Indeed, he said that he had reached that conclusion the week before.488 He expressed regret that he had not been more “forthright” in calling for an earlier lockdown.489 Mr Johnson disagreed. He said that he did “not believe that [the mandatory lockdown] should have been made earlier“.490 However, all the scientific evidence is against him and the Inquiry agrees with Mr Gove. |
| 4.222. | There was no need for any delay and an urgent need for immediate action. The fact that operational planning and processes were not fully in place was no reason for delay. They could have been built up in the first few days of the lockdown. |
| 4.223. | The imperative for mandatory lockdowns in Scotland, Wales and Northern Ireland was not as great as in England, given that these nations were not as far along the epidemiological curve, but a lockdown in England and not in the other three nations would have been epidemiologically and logistically impracticable. Baroness Foster stated: “[T]here was no realistic alternative but to follow the UK Government’s lead.“491 Mr Drakeford made a similar point.492 Ms Sturgeon said that it would have been “virtually impossible in practical terms for Scotland to have entered full lockdown earlier than the UK government decided appropriate“, given the need for the UK government to provide the resources for schemes such as furlough.493 The Inquiry accepts that it would not have been practical for one or all of the devolved administrations to take such a step in the absence of the UK government doing so. |
| 4.224. | Ms Sturgeon, Mr Drakeford and Ms O’Neill told the Inquiry that, with hindsight, the mandatory UK-wide lockdown should have been implemented earlier.494 Ms O’Neill recognised that this view was not unanimously held by the Northern Ireland Executive Committee.495 Ms Sturgeon said that she “would have wanted to introduce lockdown measures a week or so earlier. That we did not do so is a regret I carry.“496 Mr Drakeford said he had no reason to disagree with the “broad consensus that it could have happened a week earlier than it did“.497 |
The inevitability of a lockdown
| 4.225. | It is wholly understandable that any government leader should wrestle with the profound decision as to whether to order a nationwide lockdown. Given the damaging societal, economic and educational consequences it is bound to bring, enforcing a mandatory lockdown should be a measure of last resort. All viable measures short of a lockdown should be tried first and implemented early enough to allow time to analyse their effectiveness before a lockdown is imposed. |
| 4.226. | Had the many steps short of a mandatory lockdown been taken earlier in the pandemic, a mandatory UK-wide lockdown might not have become necessary or it might have been possible to reduce its length. To that extent, all four governments can be rightly criticised. |
| 4.227. | However, the Inquiry rejects the criticism that the four governments were wrong – in principle – to impose a lockdown. Indeed, the Inquiry accepts the consensus of the evidence before it that a mandatory lockdown should have been imposed one week earlier. |
| 4.228. | The UK government and devolved administrations had received clear and compelling advice by this time that the exponential growth in transmission, in the absence of a mandatory lockdown, would be likely to lead to loss of life on a scale that was reasonably to be regarded as unconscionable and unacceptable. No government, acting in accordance with its overarching duty to preserve life, could ignore such advice or tolerate the number of deaths envisaged. The governments’ laudable aim was therefore to minimise the numbers of deaths, particularly among the elderly and vulnerable, and to prevent the healthcare systems across the UK from collapsing at all costs. In this, they acted in common with many other countries. |
| 4.229. | It cannot be known whether – through their undoubted ability to expand at speed (including through the cancellation of elective care, the discharge of patients and the construction of Nightingale hospitals) and the incredible resourcefulness and commitment of their staff – the health services across the UK would have collapsed if there had been no lockdown. However, there was a serious risk, which the governments were reasonably entitled not to run, that exponential growth would lead to hospital cases of such a magnitude that, if the growth were not radically reduced, the point would inevitably be reached at which no health service would survive. At that point, the loss of life would be exacerbated by the collapse of the health system and the denial of care for Covid-19 cases, as well as for those suffering from serious, non-Covid-19 conditions. |
| 4.230. | No reasonable government could effectively gamble the lives of its citizens on its own assessment that the restrictions of 16, 18 and 20 March 2020 might, of themselves, be enough. There was no time to wait. |
| 4.231. | Through their own acts and omissions, the four governments had made lockdown inevitable. |
- INQ000273553_0058 para 9.6
- ‘Coronavirus: Italy extends emergency measures nationwide’, BBC News, 10 March 2020 (https://www.bbc.co.uk/news/world-europe-51810673; INQ000573840)
- ‘Coronavirus: The world in lockdown in maps and charts’, BBC News, 7 April 2020 (https://www.bbc.co.uk/news/world-52103747; INQ000573841)
- Helen MacNamara 1 November 2023 40/4-19
- INQ000249526_0066 para 211
- INQ000056209_0006; INQ000056158_0001 para 3. The reasonable worst-case scenario for Covid-19 estimated infection of “80% of the UK population, and up to 1% of this group will die as a direct result of the infection”; this was “up to 520,000 people” dying (INQ000146569_0001-0002).
- INQ000215035_0014 para 56
- INQ000215035_0014 para 56
- INQ000383739_0002-0003; INQ000425604; INQ000485979_0094 para 357
- INQ000232194_0064 para 270
- INQ000255836_0060 para 239; see also INQ000089005_0004
- INQ000273872_0053 para 232
- INQ000280647_0009 para 27
- INQ000283193
- INQ000280647_0009 para 27, footnote 5
- INQ000249526_0082-0083 para 254
- INQ000249526_0081-0082 para 251
- INQ000144792_0036 para 85; see also INQ000252722_0007 para 16
- INQ000147810_0029-0030 para 90
- Andrew Morris 23 January 2024 182/20-23; INQ000346264_0011 para 41
- INQ000226148_0004
- INQ000226942_0001; see also Mark Drakeford 13 March 2024 90/4-5; INQ000147283_0001
- Vaughan Gething 11 March 2024 56/16-20
- INQ000182427_0007
- ‘Written Statement: Critical care capacity and ventilation’, Vaughan Gething, Minister for Health and Social Services, Welsh Government, 5 April 2020 (https://www.gov.wales/written-statement-critical-care-capacity-and-ventilation; INQ000182395)
- INQ000083241_0004
- INQ000313127_0001
- INQ000356177_0022 para 77
- INQ000421704_0019-0020 para 45
- INQ000421704_0150-0152 para 326
- INQ000421704_0150-0152 para 326
- Ian Young 7 May 2024 153/18-22; INQ000437430_0090 para 282; Joanne McClean 2 May 2024 120/17-121/22
- See Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, recommendation 5 (https://covid19.public-inquiry.uk/documents/module-1-full-report); Covid-19 Inquiry: Resilience and preparedness (Module 1) Report. Executive response, The Executive Office, 16 January 2025, p14 (https://www.executiveoffice-ni.gov.uk/publications/executive-response-covid-19-module-1-report-jan-2025)
- INQ000109142_0002 para 1
- INQ000273553_0045-0047 para 8.13. As noted in Chapter 2: The emergence of Covid-19, in this volume, in late February 2020, two surveillance systems were put in place to get an estimate of prevalence of infection. Firstly, people in intensive care units with pneumonia were tested. Secondly, the Royal College of General Practitioners tested a random sample of patients attending GP practices for Covid-19.
- INQ000273553_0045-0047 para 8.13
- INQ000273553_0045-0047 para 8.13
- INQ000273553_0045-0047 para 8.13
- INQ000249526_0066 para 211
- INQ000249526_0066 para 212
- Michael McBride 10 May 2024 148/12-15
- Patrick Vallance 20 November 2023 45/4-21
- INQ000309529_0034 para 114(b)
- INQ000116811_0047 para 169
- INQ000109142_0004 para 30
- INQ000109142_0003 para 19
- INQ000109142_0003 para 20
- INQ000109142_0003 para 24
- INQ000064580_0002-0003
- INQ000109142_0004 para 26
- INQ000129100_0001; INQ000188738_0016 para 73; David Halpern 1 November 2023 177/5-21
- INQ000188738_0016 paras 74-75
- INQ000236391_0001 paras 1, 7
- INQ000109142_0002 para 2
- INQ000236389_0001
- INQ000236391_0001 para 2; INQ000251645_0092-0093 para 7.97
- INQ000232194_0063 para 267
- INQ000232194_0063 para 267; Matt Hancock 30 November 2023 31/1-34/11
- Boris Johnson 6 December 2023 122/2-6
- INQ000215035_0015 para 59
- INQ000149061_0001
- INQ000273872_0044 paras 25-27; INQ000269182_0034 para 115
- INQ000269182_0034 para 115; INQ000196056; INQ000149009
- INQ000273872_0044 paras 25-26
- INQ000273872_0044-0045 para 26
- INQ000273872_0044-0045 para 26
- INQ000273872_0039
- INQ000252711_0008-0009 para 34
- Helen MacNamara 1 November 2023 38/17-22
- INQ000273841_0032-0033 para 61
- INQ000273841_0032-0033 paras 60-61
- Helen MacNamara 1 November 2023 37/1-20; INQ000273841_0032 para 60; see also INQ000273872_0045 para 28
- INQ000048399_0002
- INQ000048399_0002
- Michael McBride 10 May 2024 148/4-11
- INQ000421704_0152-0153 para 329
- INQ000425611_0003-0004 paras 8, 11
- INQ000048399_0002
- INQ000048399_0003
- INQ000212052_0001
- INQ000238826_0081-0082 para 256
- INQ000228786_0001; INQ000212052_0001; see also INQ000048399_0006
- INQ000119697
- INQ000251645_0092 para 7.96
- INQ000232194_0064-0065 para 272
- INQ000136751_0001
- INQ000251645_0093 para 7.98
- INQ000259848_0019 para 32
- INQ000136751_0001
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000146636_0064-0065
- INQ000146636_0065
- INQ000232194_0065-0066 para 276
- INQ000269182_0038 para 134
- Boris Johnson 6 December 2023 124/24-25; see also INQ000146636_0070
- INQ000252711_0009 para 35
- INQ000215035_0016 para 64
- INQ000273872_0049 para 215
- INQ000255836_0047 para 198
- INQ000255836_0047-0048 paras 199, 202
- INQ000255836_0048 para 202
- INQ000048399_0003-0004
- INQ000048399_0003-0004
- INQ000048399_0003-0004
- INQ000048399_0004
- INQ000048399_0004
- INQ000048399_0005
- INQ000383721_0005
- INQ000383721_0005
- INQ000383721_0001-0002
- INQ000221921_0002
- The Public Health (Control of Disease) Act 1984, section 45c (https://www.legislation.gov.uk/ukpga/1984/22)
- INQ000276282_0024 para 104
- Mark Drakeford 13 March 2024 85/10-19
- INQ000228790_0001
- INQ000228790_0001
- INQ000048089_0002
- INQ000048089_0002
- INQ000195888_0001
- Neil Ferguson 17 October 2023 175/4-13; see also INQ000263373_0005 para 11
- INQ000207029
- INQ000238826_0084-0085 paras 264-266
- INQ000048090_0001; INQ000238826_0085-0086 para 267
- INQ000238826_0085-0086 para 267
- INQ000048399_0006
- INQ000048399_0006
- INQ000228799_0001
- INQ000207029_0001; INQ000228800
- Helen MacNamara 1 November 2023 43/21-25, 44/1-4; INQ000238826_0088-0089 para 272; Patrick Vallance 20 November 2023 47/7-18; Dominic Cummings 31 October 2023 200/7-17
- INQ000273841_0035-0036 para 65
- Helen MacNamara 1 November 2023 43/21-25, 44/1-4
- INQ000273841_0035-0036 para 65
- INQ000146579; INQ000106216
- INQ000119697_0004
- INQ000119697_0004
- INQ000174708; see also Covid-19 Dashboards for 17 March 2020 (INQ000055918), 18 March 2020 (INQ000056058), 19 March 2020 (INQ000055920) and 20 March 2020 (INQ000056076). The Covid-19 Dashboard was used to present data to decision-makers. Its role in decision-making is examined in Chapter 11: Government decision-making, in Volume II.
- INQ000174708_0005
- INQ000273872_0051 para 229
- INQ000238826_0088-0089 para 272
- INQ000238826_0088-0089 para 272; Patrick Vallance 20 November 2023 47/7-18
- INQ000280628_0056 para 104; Christopher Wormald 2 November 2023 143/10-144/18
- INQ000279910
- INQ000146579; INQ000215035_0016 para 65; INQ000280628_0057 para 106
- INQ000109142_0004 para 26
- INQ000245702_0001
- INQ000233522_0001
- INQ000233522_0002
- INQ000233522_0002
- Patrick Vallance 20 November 2023 45/12-19
- Patrick Vallance 20 November 2023 45/19-46/1
- Patrick Vallance 20 November 2023 46/2-6
- INQ000086883
- INQ000065689_0017
- INQ000087163
- INQ000182338_0002 para 4(a)
- INQ000250229_0024 para 94; INQ000182343; ‘New government structures to coordinate response to coronavirus’, Prime Minister’s Office, 10 Downing Street, Cabinet Office, Department of Health and Social Care, Foreign and Commonwealth Office, HM Treasury, Department for Business, Energy and Industrial Strategy and Boris Johnson, 17 March 2020 (https://www.gov.uk/government/news/new-government-structures-to-coordinate-response-to-coronavirus; INQ000086849)
- INQ000215035_0017 para 68; INQ000146636_0075-0078
- INQ000238826_0093-0094 para 287
- INQ000183892_0005
- INQ000056076
- INQ000249526_0082-0083 para 254
- INQ000249526_0081-0082 paras 250, 253
- INQ000238826_0092 para 284; INQ000075664
- INQ000075664_0002 para 10
- INQ000075664_0002 para 1
- INQ000075664_0002 paras 2-3
- INQ000075664_0003 paras 20
- INQ000075664_0003 para 21
- Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand, Imperial College London, 16 March 2020, p1 (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/disease-areas/covid-19/report-9-impact-of-npis-on-covid-19; INQ000228166)
- Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand, Imperial College London, 16 March 2020, p16 (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/disease-areas/covid-19/report-9-impact-of-npis-on-covid-19; INQ000228166)
- Report 9: Impact of Non-Pharmaceutical Interventions (NPIs) to Reduce COVID-19 Mortality and Healthcare Demand, Imperial College London, 16 March 2020, p2 (https://www.imperial.ac.uk/mrc-global-infectious-disease-analysis/disease-areas/covid-19/report-9-impact-of-npis-on-covid-19; INQ000228166)
- INQ000238826_0091 para 280
- INQ000119436_0001 para 3
- INQ000075664_0002 para 16
- INQ000075664_0002 paras 14-15
- INQ000075664_0002 para 17
- INQ000075664_0004
- INQ000075664_0004. NHSX was a unit of NHS England and the Department of Health and Social Care, responsible for setting policy and developing best practice for NHS technology, digital and data, including data-sharing and transparency.
- INQ000249526_0072 para 221
- Christopher Whitty 21 November 2023 26/2-7
- INQ000056183_0001
- INQ000056210_0004 para 1
- INQ000056184_0005
- INQ000056184_0005; INQ000056210_0004 para 3
- INQ000056184_0006
- INQ000056210_0004, 0008 paras 2, 3, 14; INQ000056184_0005
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0002)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0002)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0002)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0003)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0003)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0003)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0003)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 March 2020’, Prime Minister’s Office and Boris Johnson, 16 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-16-march-2020; INQ000052566_0003)
- ‘People advised to limit social contact’, Scottish Government, 16 March 2020 (https://www.gov.scot/news/people-advised-to-limit-social-contact; INQ000548030)
- ‘Statement from the Executive on Covid-19 response’, The Executive Office, 16 March 2020 (https://www.executiveoffice-ni.gov.uk/news/statement-executive-covid-19-response; INQ000114480)
- INQ000271921; ‘Chief Medical Officer for Wales announces death of first COVID-19 patient in Wales’, Welsh Government, 16 March 2020 (https://www.gov.wales/chief-medical-officer-wales-announces-death-first-covid-19-patient-wales; INQ000048732_0001)
- INQ000251645_0094-0095 para 7.104
- INQ000251645_0093-0094 para 7.100
- INQ000251645_0093-0094 para 7.100
- INQ000238826_0195-0196 para 597
- Jonathan Van-Tam 22 November 2023 202/9
- Christopher Whitty 21 November 2023 189/25-190/1-2
- Christopher Whitty 21 November 2023 189/13-24; INQ000251645_0087-0088 para 7.81
- INQ000251645_0087-0088 para 7.81
- INQ000421704_0098 paras 207-208; Michael McBride 10 May 2024 138/4-15
- Boris Johnson 6 December 2023 117/6-8, 118/20-23
- Nicola Sturgeon 31 January 2024 145/17-20
- Vaughan Gething 11 March 2024 109/8-10
- INQ000061512_0003 para 5; INQ000052045_0003 para 8; INQ000061519_0004 paras 14-15
- INQ000272142
- INQ000272142_0002
- INQ000272142_0001
- INQ000272142_0001
- Helen MacNamara 1 November 2023 23/23-24/17; INQ000273841_0016-0017 para 31
- INQ000273872_0053 para 232
- INQ000048313_0009
- INQ000056135_0004
- INQ000056135_0011
- INQ000087317_0002
- INQ000087317_0002
- INQ000087317_0002 ‘Coronavirus (COVID-19): speech by Cabinet Secretary for Health and Sport 17 March 2020’, Scottish Government, 17 March 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-scottish-parliament; INQ000357367)
- INQ000273984_0023-0024 para 101
- INQ000362664_0002 para 6
- INQ000362664_0002 para 3
- INQ000362664_0002 para 4
- INQ000362664_0003-0004 paras 13-14
- INQ000362664_0003 para 13
- INQ000362664_0003 para 13
- INQ000362664_0004 para 14
- INQ000362664_0004 para 14
- INQ000309139
- INQ000438173_0005 para 18
- INQ000362237_0024, 0026 paras 91, 97; see also INQ000349180_0003; Vaughan Gething 11 March 2024 132/20-25, 133/1-23
- INQ000362237_0026-0027 para 100
- INQ000215172_0001 para 3
- INQ000048313_0009
- INQ000061693_0002
- INQ000061693_0002
- INQ000056261; INQ000056050
- INQ000268013_0015 para 4.5.8
- INQ000056261_0003
- INQ000255836_0059 para 235
- INQ000056052; INQ000056261; INQ000107255
- INQ000056261_0003
- INQ000056261_0003
- INQ000056123_0001 paras 1, 4
- INQ000078529_0005 para c
- INQ000078529_0009 para 19d
- INQ000362664_0004-0005 para 18; INQ000273979_0009 para 19
- John Swinney 30 January 2024 185/5-14
- John Swinney 30 January 2024 186/2-9
- INQ000339033_0076 para 201
- John Swinney 30 January 2024 189/2-12
- John Swinney 30 January 2024 191/16-25
- ‘Coronavirus: Scottish schools “may be shut until summer”’, BBC News, 18 March 2020 (https://www.bbc.co.uk/news/uk-scotland-51947670; INQ000651704). This was confirmed by the Deputy First Minister on 19 March 2020 (INQ000573861).
- INQ000075664_0002 paras 2, 17; INQ000075778
- INQ000074903_0002 para 5
- INQ000074903_0002-0004 paras 8, 9, 18
- INQ000075778_0002 para 2
- INQ000075778_0002 para 3
- INQ000075778_0002 para 4
- INQ000075778_0003 para 28
- INQ000048313_0009
- INQ000238826_0094-0095 para 290
- INQ000251645_0058 para 5.48
- INQ000251645_0095 para 7.108
- INQ000056211
- INQ000056211_0005 paras 2-3
- INQ000056211_0005 para 4
- INQ000056211_0005 para 3
- INQ000056211_0007 Decision 1
- INQ000056211_0007 Decision 3
- ‘Schools, colleges and early years settings to close’, Department for Education and Gavin Williamson, 18 March 2020 (https://www.gov.uk/government/news/schools-colleges-and-early-years-settings-to-close; INQ000052716_0002)
- INQ000083097_0002
- INQ000289859; ‘Michelle O’Neill calls for the immediate closure of schools and universities’, Sinn Féin, 13 March 2020 (https://sinnfein.ie/news/michelle-oneill-calls-for-the-immediate-closure-of-schools-and-universities; INQ000226013); ‘O’Neill calls for an all-island approach to deal with Coronavirus’, Sinn Féin, 14 March 2020 (https://sinnfein.ie/news/oneill-calls-for-an-all-island-approach-to-deal-with-coronavirus;
INQ000226013); ‘Common sense approach needed to combat spread of COVID-19 – Michelle O’Neill’, Sinn Féin, 16 March 2020 (https://sinnfein.ie/news/common-sense-approach-needed-to-combat-spread-of-covid-19-michelle-oneill; INQ000226013); see also Michelle O’Neill 14 May 2024 81/4-25, 82/1-15 - INQ000065689_0037; INQ000437470_0007 para 25
- INQ000048447_0006 para 19
- David Sterling 1 May 2024 165/4-14
- INQ000083098_0003
- INQ000352697_0003; INQ000250231_0015, 0034 paras 81, 187; INQ000249526_0069 para 219(a)
- INQ000251645_0172 para 8.139
- INQ000268013_0014 para 4.5.6
- INQ000195890_0001
- INQ000280647_0011-0012 para 32; INQ000056051
- COVID-19 Hospital Discharge Service Requirements, Department of Health and Social Care, 19 March 2020, p3, paras 1.3-1.4 (https://www.gov.uk/government/publications/coronavirus-covid-19-hospital-discharge-service-requirements; INQ000049702)
- COVID-19 Hospital Discharge Service Requirements, Department of Health and Social Care, 19 March 2020, p7, para 2.5 (https://www.gov.uk/government/publications/coronavirus-covid-19-hospital-discharge-service-requirements;INQ000049702)
- INQ000232194_0074-0075 para 314. This is considered further in Chapter 13: Legislation and enforcement, in Volume II.
- INQ000056055
- INQ000056262_0004; INQ000056055
- INQ000056062
- INQ000056262_0005
- INQ000056262_0005
- INQ000056262_0005
- INQ000056262_0006
- INQ000056262_0006
- INQ000226185_0069
- INQ000146594
- INQ000226185_0069
- INQ000267920
- INQ000215035_0018-0019 para 74
- INQ000221436_0021 para 92
- INQ000146593
- ‘PM: We can “turn the tide” on coronavirus crisis’, BBC News, 19 March 2020 (https://www.bbc.co.uk/news/uk-51966721; INQ000573866)
- INQ000251645_0096 para 7.111
- Health and Social Care (NI) Summary Covid-19 Plan for the Period Mid-March to Mid-April 2020, Department of Health (Northern Ireland), 19 March 2020 (https://www.health-ni.gov.uk/publications/health-and-social-care-ni-summary-covid-19-plan-period-mid-march-mid-april-2020; INQ000103714)
- Health and Social Care (NI) Summary Covid-19 Plan for the Period Mid-March to Mid-April 2020, Department of Health (Northern Ireland), 19 March 2020, p7 (https://www.health-ni.gov.uk/publications/health-and-social-care-ni-summary-covid-19-plan-period-mid-march-mid-april-2020; INQ000103714)
- Health and Social Care (NI) Summary Covid-19 Plan for the Period Mid-March to Mid-April 2020, Department of Health (Northern Ireland), 19 March 2020, p6 (https://www.health-ni.gov.uk/publications/health-and-social-care-ni-summary-covid-19-plan-period-mid-march-mid-april-2020; INQ000103714)
- Health and Social Care (NI) Summary Covid-19 Plan for the Period Mid-March to Mid-April 2020, Department of Health (Northern Ireland), 19 March 2020, p6 (https://www.health-ni.gov.uk/publications/health-and-social-care-ni-summary-covid-19-plan-period-mid-march-mid-april-2020; INQ000103714)
- INQ000065737_0008
- INQ000425539_0014-0016
- Robin Swann 13 May 2024 135/ 3-9
- Robin Swann 13 May 2024 134/22-25
- INQ000071111_0001 para 1
- INQ000075778_0002 para 12
- INQ000071111_0001 para 5
- INQ000071111_0001 para 3
- INQ000056265_0004
- INQ000056265_0004
- INQ000255836_0065 para 252
- INQ000056265_0005; INQ000056066
- INQ000056265_0005; INQ000056066
- INQ000056265_0005-0007; INQ000056066_0001-0002
- INQ000056265_0007-0008; INQ000056066
- INQ000056212
- INQ000255836_0066 para 254
- INQ000361417_0003
- INQ000056212; INQ000273747_0016-0017 para 48
- INQ000056212_0004 para 1
- INQ000106263
- INQ000106263_0001 para 2
- INQ000106263_0002 para 5
- INQ000106263_0003 para 11a
- INQ000056212_0004 para 2
- INQ000106263_0002 para 4
- INQ000238826_0095-0096 para 293
- INQ000056212_0005-0006 para 6
- INQ000056212_0007 Decision 1
- Michael Gove 28 November 2023 77/16-78/2
- ‘Prime Minister’s statement on coronavirus (COVID-19): 20 March 2020’, Prime Minister’s Office and Boris Johnson, 20 March 2020 (https://www.gov.uk/government/speeches/pm-statement-on-coronavirus-20-march-2020; INQ000086757)
- INQ000339033_0076 para 202; ‘Statement by First Minister on additional measures announced by Prime Minister’, Welsh Government, 20 March 2020 (https://www.gov.wales/statement-first-minister-additional-measures-announced-prime-minister; INQ000350705); ‘Coronavirus: Closure of social venues will lower death toll’, BBC News, 20 March 2020 (https://www.bbc.co.uk/news/uk-northern-ireland-51972262; INQ000605481)
- The Health Protection (Coronavirus, Business Closure) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/327/contents); The Health Protection (Coronavirus, Business Closure) (Wales) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/326/contents/made)
- INQ000056212_0007 Decision 2
- ‘How coronavirus advice from Boris Johnson has changed’, The Guardian, 23 March 2020 (https://www.theguardian.com/world/2020/mar/23/how-coronavirus-advice-from-boris-johnson-has-changed; INQ000273360_0002)
- INQ000049748_0012
- INQ000249526_0084 para 260
- INQ000056076_0002
- INQ000056263_0002
- INQ000056263_0002
- INQ000056263_0002
- INQ000056263_0003
- INQ000056263_0003-0004
- INQ000056263_0003
- INQ000056263_0004-0005
- INQ000056073
- INQ000215035_0019 para 76
- INQ000376650
- INQ000228862
- INQ000228862
- INQ000056076_0016
- INQ000056078_0005
- INQ000232194_0076 para 319
- INQ000056266_0004
- INQ000056266_0006
- INQ000056085
- INQ000203890_0001 para 1
- INQ000106286
- INQ000106286_0006; INQ000255836_0087-0088 para 330
- INQ000056094
- INQ000074912_0001
- INQ000196761
- INQ000071111
- INQ000071111_0001 para 1
- INQ000071111_0001 para 2
- INQ000071111_0001 para 3
- INQ000071111_0001 para 4
- INQ000052717_0002 paras 1, 8
- INQ000052717_0002 para 1
- INQ000052717_0002, 0003 paras 2, 20
- INQ000312930_0001 para 4
- INQ000336319_0002
- INQ000056264
- INQ000056264_0004
- INQ000056264_0004-0005
- INQ000056264_0007-0008
- INQ000056264_0011-0012
- INQ000056264_0012
- INQ000056264_0012
- INQ000056264_0012
- INQ000056264_0012
- INQ000056102
- INQ000056098; INQ000056258
- INQ000056098_0001
- INQ000056258_0001
- INQ000056096
- INQ000056096
- Boris Johnson 6 December 2023 134/4-6
- INQ000228874
- INQ000228874
- INQ000056213
- This meeting was originally planned to take place on 22 March but it was postponed (INQ000061710); INQ000366557
- INQ000089938_0001-0002 paras 5-6; INQ000056213_0004 para 4
- INQ000089938_0003 para 15
- INQ000056213_0004 para 1
- INQ000056213_0006 para 12; see also INQ000255836_0071-0072 para 275
- INQ000056213_0004 para 3
- INQ000056213_0007
- INQ000056213_0006 para 12
- INQ000056136
- ‘Prime Minister’s statement on coronavirus (COVID-19): 23 March 2020’, Prime Minister’s Office and Boris Johnson, 23 March 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020; INQ000086759_0003)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 23 March 2020’, Prime Minister’s Office and Boris Johnson, 23 March 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020; INQ000086759_0003)
- ‘Coronavirus (COVID-19) update: First Minister’s speech 23 March 2020’, Scottish Government, 23 March 2020 (https://www.gov.scot/publications/first-minister-covid-19-update-1; INQ000354217); ‘First Minister of Wales’ statement on new coronavirus measures’, Welsh Government, 23 March 2020 (https://www.gov.wales/first-minister-of-wales-statement-on-new-coronavirus-measures; INQ000350706)
- ‘Executive publishes list of essential businesses’, The Executive Office, 24 March 2020 (https://www.executiveoffice-ni.gov.uk/news/executive-publishes-list-essential-businesses; INQ000215024)
- The Health Protection (Coronavirus, Restrictions) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/350/contents/made); The Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/353/contents/made);
The Health Protection (Coronavirus) (Restrictions) (Scotland) Regulations 2020 (https://www.legislation.gov.uk/ssi/2020/103/contents); INQ000290207;
The Health Protection (Coronavirus, Restrictions) Regulations (Northern Ireland) 2020 (https://www.legislation.gov.uk/nisr/2020/55/contents/made) - INQ000371209_0037-0038 paras 120-121; see also INQ000371209_0039 para 125; Mark Drakeford 13 March 2024 104/13-21
- INQ000339033_0044 para 115
- INQ000449440_0059-0060 para 171; see also Michelle O’Neill 14 May 2024 119/9-120/18
- David Sterling 1 May 2024 140/4-6
- Michelle O’Neill 14 May 2024 120/15-21; Arlene Foster 15 May 2024 88/10-12
- INQ000421704_0164 para 354; see also INQ000418976_0023 para 75; INQ000436641_0022 para 78
- Michelle O’Neill 14 May 2024 114/9-16; Arlene Foster 15 May 2024 88/17-22
- INQ000086935
- INQ000250231_0015-0016 para 85
- INQ000250231_0051 para 285
- INQ000238826_0077-0078 para 244
- UK Influenza Pandemic Preparedness Strategy 2011, Department of Health, 10 November 2011 (https://assets.publishing.service.gov.uk/media/5a7c4767e5274a2041cf2ee3/dh_131040.pdf;
INQ000022708); Christopher Wormald 2 November 2023 108/10-11; Imran Shaf i 30 October 2023 143/8-15 144/8-10 - Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 4 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000051883_0002 para 11
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.42 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000061510_0003 para 20
- INQ000281260_00010 para 37
- INQ000281260_0008-0009 para 30
- INQ000119430_0001 para 9; INQ000212223_0002; INQ000151558_0003; INQ000056221_0005 para 2; INQ000048399_0003; INQ000236391_0002 para 24
- INQ000188738_0039, 0040 paras 160, 163
- INQ000251645_0101 para 7.126
- See Module 1: The resilience and preparedness of the United Kingdom, UK Covid-19 Inquiry, July 2024, Chapter 5 (https://covid19.public-inquiry.uk/documents/module-1-full-report)
- INQ000251645_0085 para 7.70
- INQ000251645_0101 para 7.125
- Ben Warner 6 November 2023 153/4-23
- INQ000250231_0027 para 149
- Mark Woolhouse 16 October 2023 40/9-12
- INQ000255836_0087 para 329
- INQ000061517_0003 paras 7-8
- Patrick Vallance 20 November 2023 30/10-13
- Coronavirus: Action Plan: A Guide to What You Can Expect Across the UK, Department of Health and Social Care, 3 March 2020, p18, para 4.42 (https://assets.publishing.service.gov.uk/media/5e5e2e91e90e071110454391/Coronavirus_action_plan_-_a_guide_to_what_you_can_expect_across_the_UK.pdf; INQ000182380)
- INQ000273553_0021-0022 para 6.6.2
- INQ000273553_0104-0105 para 16.8
- INQ000263373_0005 para 11
- ‘Watch again: Boris Johnson says government is moving towards “delay phase” of coronavirus’, YouTube, undated (https://www.youtube.com/watch?v=Yc1alOEjDVA; INQ000223088_0004-0005); ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0002-0004)
- INQ000251645_0111 para 7.162; INQ000238826_0072 para 229
- Christopher Whitty 22 November 2023 23/18-25/13; INQ000273901_0003
- INQ000255836_0022 paras 88-89
- Christopher Whitty 22 November 2023 25/12-17; INQ000251645_0111 para 7.161
- INQ000251645_0111 para 7.162; INQ000238826_0071-0072 para 228
- INQ000056219_0005 para 6; ‘Watch again: Boris Johnson says government is moving towards “delay phase” of coronavirus’, YouTube, 9 March 2020 (https://www.youtube.com/watch?v=Yc1alOEjDVA; INQ000223088_0004-0005); ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0002-0004)
- INQ000048039; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0002)
- INQ000048313_0007
- INQ000238826_0098-0099 para 303
- Patrick Vallance 20 November 2023 32/2-13
- INQ000238826_0021 para 50; see also INQ000309529_0032 para 108
- INQ000238826_0098 para 302
- Patrick Vallance 20 November 2023 38/2-6
- Christopher Whitty 22 November 2023 33/7-11
- INQ000056132_0005-0006; INQ000056221_0007 para 8; ‘UK Prime Minister Boris Johnson holds a press conference on coronavirus’, YouTube, 12 March 2020 (https://www.youtube.com/live/cAE8-e5_EKY; INQ000231053_0001)
- INQ000255836_0086-0087 para 326
- Boris Johnson 6 December 2023 116/3-15; INQ000255836_0036 para 150
- Rishi Sunak 11 December 2023 65/6-68/5; Michael Gove 28 November 2023 53/16-58/23; Matt Hancock 30 November 2023 129/12-134/6
- Mark Drakeford 13 March 2024 69/12-72/3
- INQ000339033_0089 para 244
- INQ000232525_0001; INQ000289859_0001
- INQ000065689_0007
- INQ000238826_0093-0094 para 287
- INQ000232194_0066 para 280
- INQ000238826_0089 para 274
- Patrick Vallance 20 November 2023 46/6-7
- Christopher Whitty 22 November 2023 34/25-35/15
- INQ000251645_0094 para 7.102
- INQ000255836_0086-0087 para 326
- INQ000056055; INQ000215035_0017 para 67; INQ000252711_0010 para 40; Dominic Cummings 31 October 2023 250/21
- INQ000370154; Reg Kilpatrick 6 March 2024 191/3-13
- Dominic Cummings 31 October 2023 206/16-18; INQ000273872_0055 para 247
- Boris Johnson 6 December 2023 128/23-25
- INQ000273553_0059-0060 para 9.9
- INQ000249526_0092 para 280; ‘Key epidemiological drivers and impact of interventions in the 2020 SARS-CoV-2 epidemic in England’, E.S. Knock, L.K. Whittles, J.A. Lees, P.N. Perez-Guzman, R. Verity, R.G. FitzJohn, et al., Science Translational Medicine (2021), 13(602), eabg4262 (https://doi.org/10.1126/scitranslmed.abg4262; INQ000212077)
- ‘Key epidemiological drivers and impact of interventions in the 2020 SARS-CoV-2 epidemic in England’, E.S. Knock, L.K. Whittles, J.A. Lees, P.N. Perez-Guzman, R. Verity, R.G. FitzJohn, et al., Science Translational Medicine (2021), 13(602), eabg4262 (https://doi.org/10.1126/scitranslmed.abg4262; INQ000212077)
- INQ000238826_0098 paras 300-301; INQ000309529_0038 para 126; INQ000232194_0006 para 23; INQ000280628_0065 para 122; INQ000273872_0106-0107 para 534; INQ000252711_0011 para 43
- INQ000251645_0116 para 8.8
- Michael Gove 28 November 2023 80/16-17
- Michael Gove 28 November 2023 84/15-23
- INQ000255836_0086 para 325
- INQ000418976_0025 para 82
- INQ000371209_0039 para 125
- INQ000339033_0076 para 203
- INQ000339033_0076 para 203; Mark Drakeford 13 March 2024 105/5-10; INQ000436641_0025 para 87
- INQ000436641_0024 para 83
- INQ000339033_0076 para 203
- Mark Drakeford 13 March 2024 105/5-10
Chapter 5: Exit from lockdown (April to early July 2020)
Introduction
| 5.1. | This chapter examines how the UK government and devolved administrations decided to exit from lockdown. Divergence between them began to emerge as they each adopted different approaches to the easing of restrictions. The UK government was prepared to ease restrictions at a time when the prevalence of the virus was still high. In contrast, the devolved administrations took a more cautious approach to the easing of restrictions. |
| 5.2. | The UK government’s Covid-19 Dashboard dated 31 March 2020 recorded the total number of confirmed cases of Covid-19 in the UK as 25,150, with 3,009 new daily cases. The total number of confirmed deaths globally was 2,352.1 |
| 5.3. | By 2 April 2020, there had been 2,602 confirmed cases of Covid-19 in Scotland, with 126 confirmed deaths.2 In Wales, by 1 April, 1,837 people had tested positive and 98 people had died.3 Northern Ireland had 871 confirmed cases of Covid-19 by 1 April, with 45 deaths.4 |
Figure 13: Daily confirmed cases from 1 March to 30 April 2020 across the UK
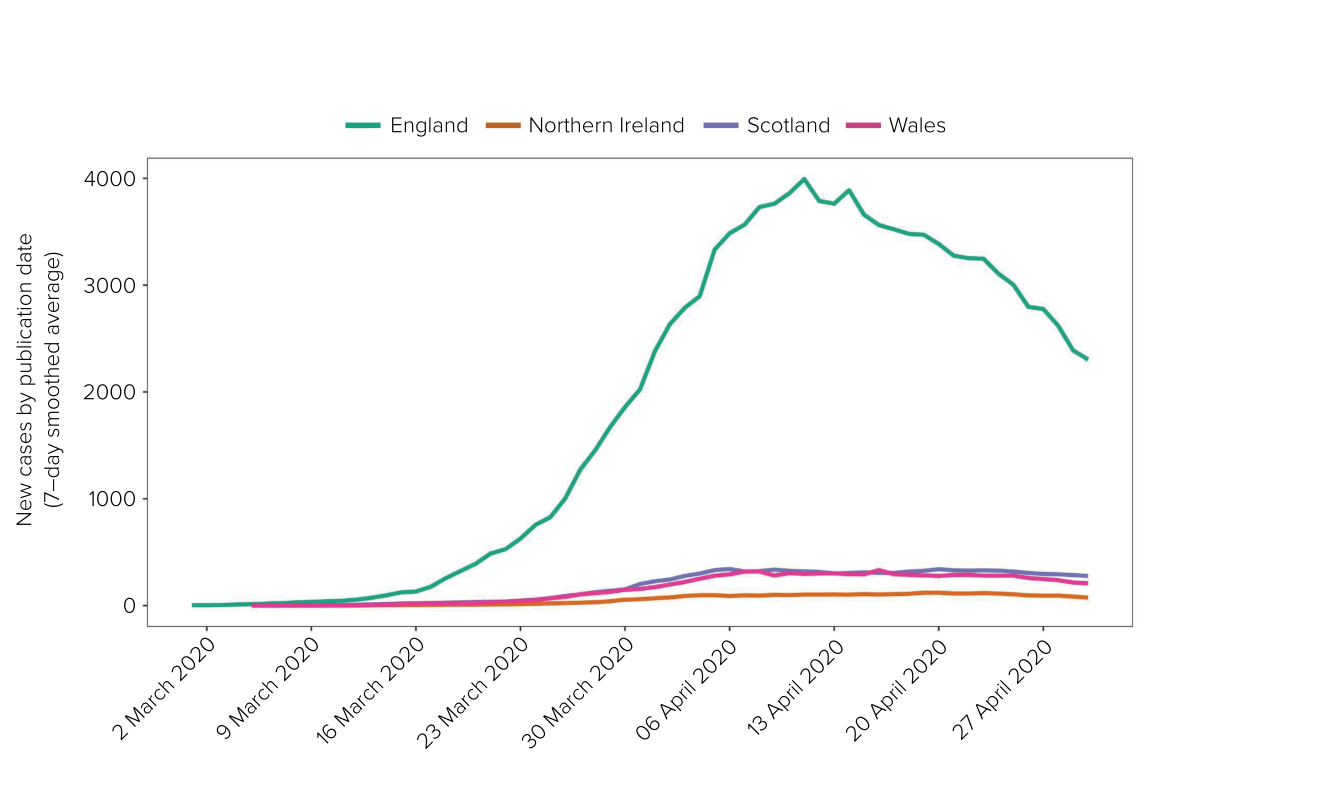
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 5.4. | Weekly deaths involving Covid-19 during this period (defined as deaths where Covid-19 was referred to on the death certificate) peaked in the week ending 17 April 2020 in England (8,355 deaths) and in the week ending 24 April in Scotland, Wales and Northern Ireland (662, 413 and 128 deaths respectively).5 |
Figure 14: Daily deaths per 100,000 population by date of death from 23 March to 13 July 2020 across the UK
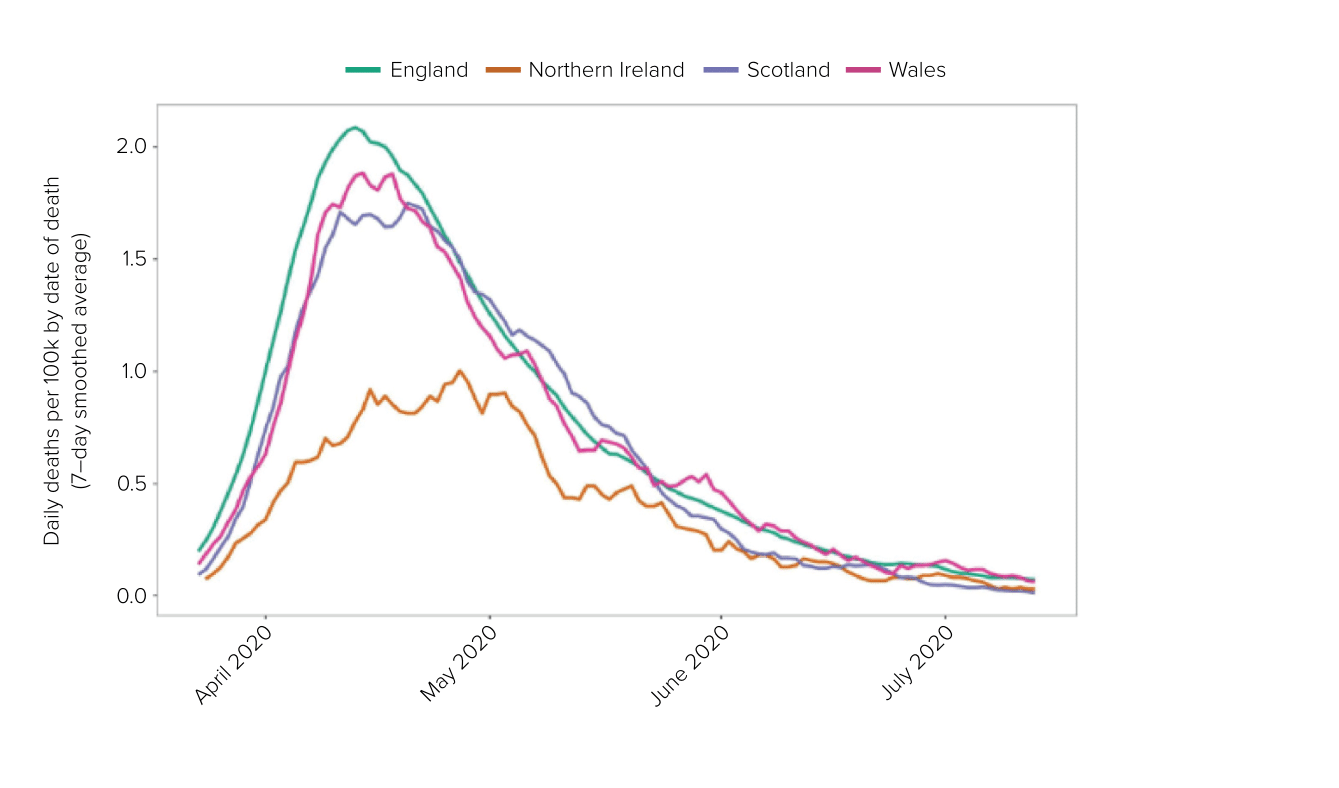
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 5.5. | To respond to the growing number of cases, NHS capacity was being increased across the UK. The first NHS Nightingale hospital was announced in England on 24 March 2020.6 It was agreed at a Covid-19 Strategy Ministerial Group meeting that day that a clear plan should be developed by the Department of Health and Social Care for the construction of a further nine new hospitals. The Department of Health and Social Care and the NHS were to work with the Ministry of Defence to ensure the 10 new hospitals were operational as soon as possible.7 Construction started on the NHS Louisa Jordan in Glasgow, a 300-bed hospital, with the ability to expand that capacity to 1,000 beds if required.8 By 20 April 2020, the Dragon’s Heart Hospital, located in the Principality Stadium in Wales, officially opened for patients, with a capacity for up to 2,000 additional beds for people with Covid-19.9 The first Nightingale hospital in Northern Ireland was announced on 2 April and had a capacity of 230 beds.10 |
| 5.6. | The need to scale up testing was also widely recognised. On 2 April 2020, Matt Hancock MP, Secretary of State for Health and Social Care from July 2018 to June 2021, set out a five-pillar strategy to expand testing capacity and publicly announced a target to carry out 100,000 tests a day by the end of April 2020.11 Mr Hancock told the Inquiry that he did so as “the testing system [was] not scaling as fast as we needed” and the target was needed “to galvanise the whole system to deliver more tests“.12 At that time, capacity was only 12,000 tests a day.13 |
| 5.7. | The Scottish Government announced its aim to increase testing capacity from 1,900 tests a day to 3,500 tests a day by the end of April.14 The Welsh Government announced that there would be capacity for 9,000 tests a day in Wales by the end of April.15 In Northern Ireland, testing had been scaled up from 40 tests per day in January 2020 to 736 tests per day. Northern Ireland’s testing strategy would “align with the UK’s strategic approach to scale-up of testing” where possible and would “also take account of testing plans in the Republic of Ireland“.16 The Inquiry is addressing the systems for test, trace and isolate in detail in Module 7: Test, trace and isolate. |
Plans for reviewing lockdown
| 5.8. | When Boris Johnson MP, Prime Minister from July 2019 to September 2022, made his announcement of a UK-wide lockdown on 23 March 2020, he stated:
“[W]e will keep these restrictions under constant review. We will look again in three weeks, and relax them if the evidence shows we are able to.“17 |
| 5.9. | The three-week review period was reflected in subsequent regulations.18 However, upon entering lockdown, the UK government and devolved administrations did not have a formal plan, set of criteria or strategy to exit lockdown. They began to devise these properly only once the UK was in lockdown. |
| 5.10. | The UK Cabinet met on 24 March 2020.19 It had not had the opportunity to discuss the mandatory lockdown decision until this point. Mr Johnson explained that the implementation of the restrictions announced the previous day had been “timed to last as little time as possible“.20 A ‘Framework for a comprehensive National Strategy’ was presented at the meeting.21 This had been commissioned by Sir Mark Sedwill (later Lord Sedwill), Cabinet Secretary and Head of the Civil Service from October 2018 to September 2020, on or around 20 March, as an “overarching strategy” for the response to “provide the framework for the operational elements“.22 Sir Philip Barton (Director General, Consular and Security in the Cabinet Office from 2017 to 2020) was tasked with leading the preparation of a “high level plan” setting out this overarching strategy, under which it was intended that the Department of Health and Social Care’s three-month battle plan to tackle Covid-19 would sit.23 Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, and senior officials at the Government Office for Science provided their input.24 |
| 5.11. | This work resulted in the production of the ‘Framework for a comprehensive National Strategy’ paper.25 It explained that the current approach to suppress the reproduction number (R) below 1 was “not sustainable indefinitely” and that decision-makers had three options in terms of an exit strategy:
The framework explained that a ‘controlled release’ was “currently the only viable option“, but it was based on the assumption that immunity was possible.27 This was the first time decision-makers had been presented with a potential strategy for how the pandemic would eventually end, but the minutes record little discussion of the framework and no decisions were made on the preferred approach.28 |
| 5.12. | On 26 March 2020, the Scientific Advisory Group for Emergencies (SAGE) agreed “to plan a forward-looking piece of work on how and when to release measures and on future needs“.29 A few days later, on 29 March 2020, SAGE noted:
“[F]urther work is required to understand how best to release measures and the scale of any resultant epidemic peaks.“30 |
| 5.13. | Shortly afterwards, Professor Dame Angela McLean, Chief Scientific Adviser to the Ministry of Defence from 2019 to 2023, emailed Professor Vallance and Professor (later Sir) Christopher Whitty, Chief Medical Officer for England from October 2019. She set out the choice for decision-makers between low and high incidence, ie the number of Covid-19 infections, when deciding the strategy for easing the lockdown.31 She explained that decision-makers would need to decide whether to:
|
| 5.14. | While a low-incidence scenario would keep deaths from Covid-19 as low as possible, there would likely be high economic and social costs as a result of keeping stringent restrictions in place for a longer period of time. Conversely, easing restrictions sooner – while incidence was still high – would be likely to cause fewer economic and social harms. It would also potentially enable the population to build up some natural immunity to Covid-19 as the infection spread through it, but would result in a greater number of deaths from the virus. |
| 5.15. | The Department of Health (Northern Ireland) had prepared a Covid-19 Emergency Response Strategy, which set out seven broad, strategic aims:
However, the strategy did not mention any specific plans about exiting lockdown.33 |
| 5.16. | An early draft of an Executive Strategy and Action Plan was considered by the Northern Ireland Executive on 30 March 2020, when it was agreed that:
“further work should be undertaken to populate it with information from departments, and that the key elements of the Department of Health’s Emergency Response Strategy should be integrated within it“.34 A revised draft was agreed on 3 April 2020.35 However, the Covid-19 Testing Strategy was not embedded into the Northern Ireland Executive Strategy and Action Plan, as had been envisaged. Robin Swann MLA, Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024, requested that the only actions within the Executive Strategy for the Department of Health (Northern Ireland) should relate to the delivery of the strategy (with all other actions for the department to be removed) to “ensure that there is no confusion or duplication“.36 This was an early example of the compartmentalisation of departments, which is discussed in greater detail in Chapter 11: Government decision-making, in Volume II. |
| 5.17. | On 31 March 2020, the Scottish Cabinet observed that “recent ‘green shoots’ messaging” by members of the UK government suggested “a degree of optimism about the rate of spread of the pandemic that did not yet appear justified by the facts“.37 It considered that this might turn out to be counter-productive because it could reduce public compliance with the lockdown measures.38 |
April 2020: Reviews of lockdown
| 5.18. | On 2 April 2020, the Scottish Government Resilience Room agreed to:
“[b]uild active rebuttal of the idea perpetuated by UKG [UK government] that social distancing measures may be lifted at Easter into marketing campaigns and communications“.39 It was anticipated that lockdown measures would need to be in place for at least two months to avoid a much higher peak. As such, the Scottish Government would work towards “the possibility of a different approach” from the UK government.40 |
| 5.19. | On 4 April 2020, the First Ministers of Scotland and Wales and the First Minister and deputy First Minister of Northern Ireland wrote jointly to Mr Johnson in anticipation of “a further set of co-ordinated announcements on or around 13 April“.41 They suggested a COBR meeting the following week to discuss the upcoming review of the lockdown, commenting that there was “no reason not to ensure an orderly process is established ahead of this predictable milestone“.42 They also requested a:
“transparent and collaborative approach to sharing and producing analysis, options appraisal, and papers for any COBR meeting next week“.43 Regular four-nation meetings were yet to be established, but a COBR meeting was subsequently convened on 9 April. |
| 5.20. | On 5 April 2020, Dr Catherine Calderwood, Chief Medical Officer for Scotland from April 2015 to April 2020, resigned after making two trips to her second home during the lockdown.44 (The impact of alleged rule-breaking by advisers and decision-makers is examined in Chapter 11: Government decision-making, in Volume II.) Dr Calderwood was succeeded on an interim basis by Professor (later Sir) Gregor Smith, who had been Deputy Chief Medical Officer for Scotland from April 2015. His appointment was made permanent in December 2020. |
| 5.21. | That same day, Professors Whitty and Vallance shared a paper they had drafted on possible approaches to the next phases of the pandemic with the Cabinet Office and 10 Downing Street.45 One of the paper’s central conclusions was that variations of social distancing, possibly enhanced by “track and trace” and shielding the most vulnerable, were “the most realistic routes to controlling the effects of this epidemic“.46 It also warned that, although vaccines or drugs might assist in the longer term:
“[T]hey will take time and should not be relied on as the easy way out. It is a policy choice whether to run R as low as it can be achieved … or running R as near to 1 as it can be managed within the boundaries the NHS can cope with. The latter would imply an ongoing significant direct COVID-19 mortality but potentially with less social damage and indirect mortality, and quicker although still lengthy exit from the epidemic as population immunity accumulates (assuming it does).“47 |
| 5.22. | Also on 5 April 2020, Sir Mark Sedwill provided Mr Johnson with a paper concerning the next phase of the pandemic. It set out key questions in advance of the first review of the lockdown restrictions, as the government aimed to “navigate the country through the next few months and seek to turn the tide by early summer“.48 It advised that it was necessary to consider whether it was now possible to allow the economy and society to recover:
“some normalcy while also managing the immediate and subsequent peak public health risks“.49 Sir Mark Sedwill advised that modelling from SAGE indicated that the first review of the lockdown restrictions at a COBR meeting in mid-April 2020 would be likely to coincide with the peak in deaths and pressure on the NHS. Therefore, that now might be “the wrong moment to contemplate any relaxation of the restrictions“.50 However, since: “the practical effect of the ‘stay home’ measures had exceeded the requirements set out by SAGE, notably on work in the workplace … [w]e could use the political theatre of the review to re-set the public narrative, and bring others like the mayors and DAs [devolved administrations] into alignment, by confirming that people should work safely in the workplace or outdoors if they cannot work from home.“51 |
| 5.23. | Mr Johnson was admitted to hospital later on 5 April 2020, having contracted Covid-19.52 Following a deterioration in his condition, he was admitted to intensive care where he remained for several days.53 (Chapter 11: Government decision-making, in Volume II, examines the lack of leadership contingency arrangements in place when Mr Johnson was admitted to hospital.) |
| 5.24. | In Scotland, Nicola Sturgeon MSP, First Minister of Scotland from November 2014 to March 2023, led a ‘deep dive’ meeting into social distancing measures on 6 April 2020. The briefing paper said that it was “highly unlikely” that any easing of lockdown measures would be advised for COBR’s mid-April review but demand was growing for “an exit strategy“.54 |
| 5.25. | On 7 April 2020, the Private Office at 10 Downing Street sent Dominic Raab MP, Secretary of State for Foreign and Commonwealth Affairs and First Secretary of State from July 2019 to September 2021 – who deputised for Mr Johnson while he was in hospital – a note ahead of the first review of the lockdown regulations.55 It stated that it was “not likely we’ll recommend changing the social distancing measures immediately“, given the review would potentially coincide with peak deaths.56 However, one possible exception to this concerned attendance at work, which was lower than had been anticipated due to compliance with the ‘Stay Home’ order. The note advised that Mr Raab might wish to “consider setting out a strategy for the months ahead for managing the spread and exit from the pandemic“.57 |
| 5.26. | A SAGE meeting held on the same day concluded that “there is no current evidence that transmission is accelerating; it may be slowing“.58 |
| 5.27. | SAGE advice on 9 April 2020 stated that the World Health Organization had “concluded there is currently no conclusive evidence that facemasks are beneficial for community use“. However, SAGE advised that at its next meeting it would review a paper on the matter from the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG).59 |
| 5.28. | A COBR meeting was held on the afternoon of 9 April 2020, chaired by Mr Raab.60 Mark Drakeford MS, First Minister of Wales from December 2018 to March 2024, had spoken the previous day to Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021, Minister for the Cabinet Office from February 2020 to September 2021, but “no commitment was made by him to hold a further COBR meeting” at that time.61 The devolved administrations therefore received less than 24 hours’ notice of this meeting. The agenda contained three brief items: “1) Current situation update 2) Update on social distancing 3) Communications over Easter”.62 |
| 5.29. | In the absence of any clarity about the purpose of the meeting, the First Ministers of Scotland, Wales and Northern Ireland, the deputy First Minister of Northern Ireland and the Mayor of London agreed a joint position of their own: that they “expect[ed] restrictions to remain in place for some weeks yet“.63 A paper presented at the meeting advised that public communications in advance of Easter should emphasise the importance of continued compliance with the lockdown. It also confirmed that restrictions were being kept under review and SAGE would meet the following week to assess their impact in light of further data becoming available.64 It was agreed that communications should set out the:
“need for continued compliance with social distancing measures, without raising expectations that the measures will be lifted the following week“.65 |
| 5.30. | On 10 April 2020, the Cabinet Office sent Mr Raab a note setting out the need for a medium-term strategy for the Covid-19 response.66 It explained that a 12-month plan was needed for a “new normal” that balanced the health, social and economic impacts of the virus.67 This required an integrated approach of interventions that best controlled the virus while allowing society to open up again – “not a simple trade-off” between health and economic considerations.68 The note set out proposed programmes of work, including work on population segmentation, the development of new measures that better balanced health, social and economic impacts (described as ‘smart’ interventions) and support for vulnerable groups. |
| 5.31. | A working group meeting of SAGE considered “‘[t]he science of exit’ from lockdown” on 10 April.69 On 14 April, this working group produced a paper on lockdown exit strategies. It compared the benefits and disbenefits of exiting lockdown at a time when there were low or high levels of Covid-19 infections circulating in the population.70 The paper was subsequently discussed at meetings of this SAGE working group on 24 April and 27 April.71 |
| 5.32. | On 14 April 2020, SAGE advised that “[e]vidence does not currently support use of face masks to protect the wearer in the general population“.72 It explained that the evidence that cloth face coverings could prevent spread was “weak, but probably marginally in favour of a small effect“.73 |
The first review of the lockdown regulations
| 5.33. | The first review of the lockdown regulations was due to take place by 16 April 2020 in England, Scotland and Wales and by 18 April in Northern Ireland. On 15 April, Mr Gove met with the devolved administrations and the Mayor of London. They agreed to aim for a single approach to lifting the restrictions as far as possible.74 However, this was a decision for each government. |
| 5.34. | On 14 April 2020, the Scottish Government Covid-19 Advisory Group recommended to the Scottish Government that lockdown measures should be retained, advising that it would “not be possible (for the foreseeable future) to eradicate the virus” in Scotland and “[w]e therefore need to find ways of living with the virus“.75 The Scottish Government agreed to extend the lockdown for another three weeks.76 |
| 5.35. | On the same day, the Scottish Cabinet observed that there “had been no discussion of when easing of the restrictions might begin” across the four nations but that detailed discussions were required.77 The Scottish Government Covid-19 Advisory Group had prepared a paper for the Scottish Government entitled Covid-19 Lockdown Exit Strategies, which considered a wide range of options for relaxing lockdown measures.78 The group identified the most promising approaches as being likely to involve a combination of: (i) active surveillance, contact tracing and quarantine; (ii) enhanced shielding of vulnerable groups; and (iii) innovative approaches to maintain and enhance social distancing.79 The Covid-19 Advisory Group noted that these measures would be reliant on increasing testing capacity to 16,000 tests per day and improving real-time data flows from the health and social care sectors.80 |
| 5.36. | In England, the Cabinet Office advised the UK government that lockdown restrictions should be maintained, given advice from SAGE that there was a risk that changing the restrictions might push R above 1.81 On 15 April 2020, the UK government ministerial ‘Quad’ – comprising Mr Raab, Mr Hancock, Mr Gove and Rishi Sunak MP, Chancellor of the Exchequer from February 2020 to July 2022 – agreed that the lockdown should continue for at least another three weeks in England.82 That decision was approved by the UK Cabinet the following day.83 |
| 5.37. | The Northern Ireland Executive Committee considered the review on 15 April 2020.84 A paper submitted by Mr Swann confirmed that case numbers were rising in Northern Ireland. It said that it could be safely assumed that the true number of cases was significantly higher than the number of confirmed cases.85 The Executive Committee concluded that restrictions should not be lifted at that time.86 |
| 5.38. | Internal Welsh Government legal advice on 11 April 2020 stated that ministers’ reasons for ending lockdown would “need to be firmly rooted in public health considerations” and that other considerations such as the economy “should not be the primary focus“.87 The advice said:
“There is merit in Ministers therefore seeking to ensure that in so far as is possible the approach to exit is similar (even if not identical) to that in England in particular to avoid unintended consequences for public health in Wales that could be impacted by a different approach to relaxation.“88 On 14 April 2020, the Welsh Government received advice supported by Dr (later Sir) Frank Atherton, Chief Medical Officer for Wales from August 2016, which recommended retention of the full package of requirements.89 On 16 April, following discussions with ministers in the morning, Mr Drakeford confirmed that the restrictions would remain in force with some minor amendments in Wales.90 |
| 5.39. | Subsequently, at a COBR meeting on 16 April 2020 chaired by Mr Raab, it was agreed that the lockdown should continue across the four nations for at least a further three weeks, until 7 May 2020.91 Mr Raab announced this in a 10 Downing Street press conference later that day and set out five tests to be met before restrictions would be eased in England.92 |
Figure 15: Five tests for adjusting the lockdown, 16 April 2020
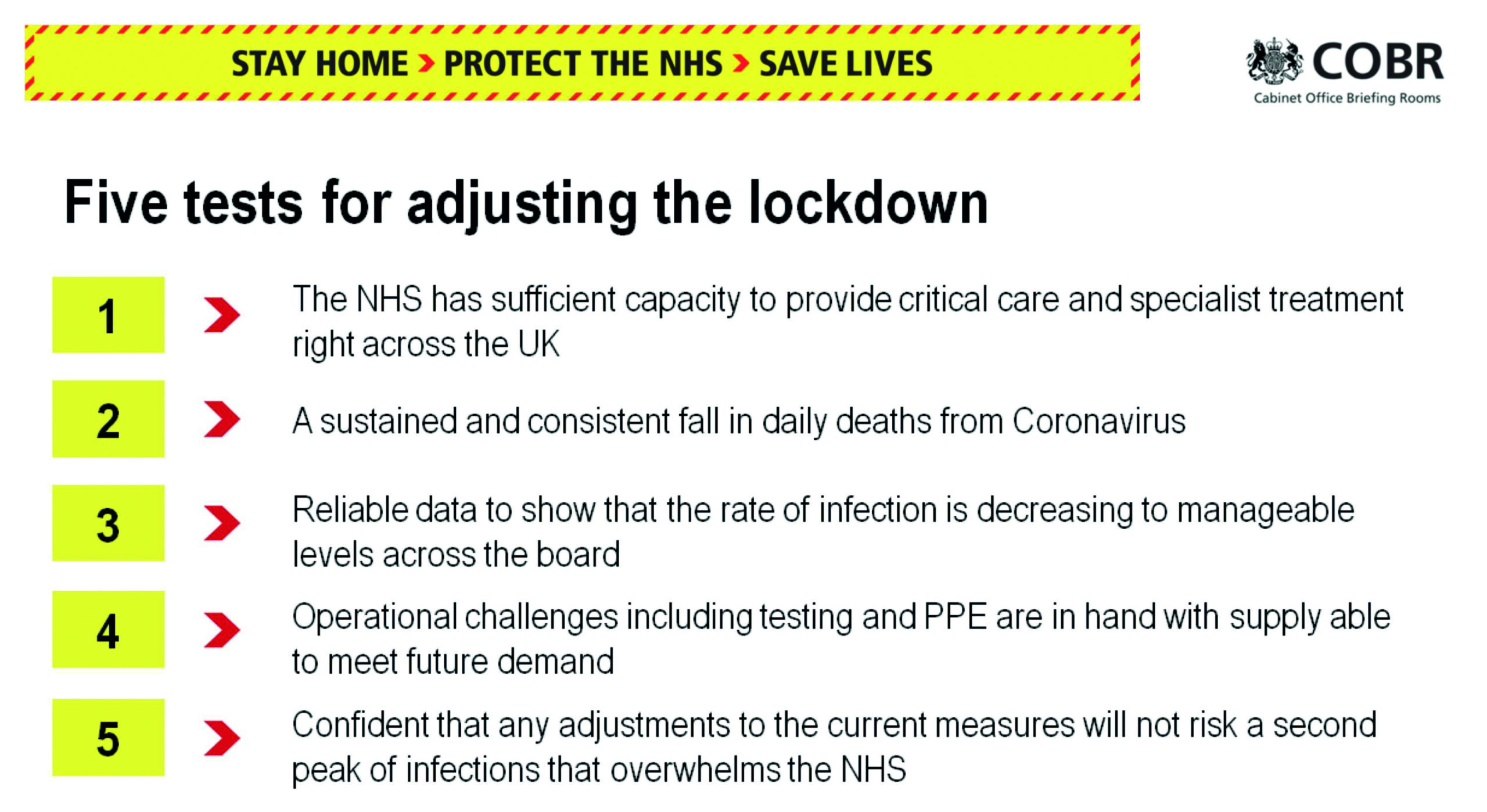
Source: INQ000651575
| 5.40. | Professor Vallance told the Inquiry that SAGE was not asked to comment on the five tests set out by Mr Raab. However, the tests did reflect the issues SAGE had discussed and on which he and Professor Whitty had provided advice.93 |
| 5.41. | These tests did identify the broad direction of travel needed before restrictions could be eased. However, their lack of specificity – for example, “manageable levels” of infection rates were not defined – meant that it remained unclear how each of the tests would be measured.94 |
| 5.42. | There had been concerns about supplies for the health services, in particular in relation to testing, bed and staff capacity, ventilators and personal protective equipment (PPE) since late March 2020.95 By mid-April 2020, Wales was at risk of running out of some items of PPE within two to four weeks.96 PPE shortages also continued in England throughout April.97 Mr Johnson subsequently appointed Paul Deighton, Lord Deighton, as ‘PPE tsar’, responsible for coordinating a “resilient PPE industry in the UK“.98 The issue of the lack of PPE in hospitals and around the UK is being further explored in detail in Module 3: Impact of the Covid-19 pandemic on healthcare systems in the four nations of the UK and Module 5: Procurement. |
| 5.43. | On 16 April 2020, SAGE agreed to produce revised advice on face coverings so they could be considered as a measure to be implemented as part of the easing of the lockdown.99 It advised that evidence of their effectiveness beyond healthcare settings was weak but “marginally positive” and highlighted the risk of community use of face coverings threatening stocks for healthcare settings.100 On the same day, there was discussion in a WhatsApp group that included Mr Hancock and Professors Vallance and Whitty about requiring members of the public to wear a face covering, following public comments made by the Mayor of London. Mr Hancock said:
“WE DO NOT HAVE ENOUGH MASKS TO SAY THESE THINGS. Talking about this before we are ready risks taking masks from nurses and social care workers who really need them … we must hold the line on masks – or they will go like loo roll.“101 |
Preparing for the second review
| 5.44. | On 20 April 2020, Mr Drakeford wrote to Mr Gove stating that, depending upon scientific and medical advice, there might be an opportunity to consider easing restrictions at the next review point. He said:
“[W]e should endeavour to work even more closely together to agree a common approach where that is possible and to assist appreciation of difference where that is necessary.“102 Mr Drakeford also called for a “regular rhythm” of intergovernmental meetings, in which officials met early in the week, devolved administrations and the Mayor of London met with Mr Gove in the middle of the week, and there was a COBR meeting at the end of the week.103 The issue of the intergovernmental relationships between the UK government and devolved administrations is addressed in detail in Chapter 14: Intergovernmental working, in Volume II. |
| 5.45. | On 21 April 2020, SAGE advised that there was evidence to support the wearing of face coverings as a precautionary measure in higher-risk settings such as shops and transport where social distancing was not possible. Any decision to require members of the public to wear face coverings should not jeopardise the availability of masks for use in healthcare settings.104 It stated that the effect of wearing a face covering was “small but not zero“.105 |
| 5.46. | On 22 April 2020, the UK government Quad discussed a draft strategy for the next phase of the Covid-19 response.106 A few days earlier, Dominic Cummings, Adviser to the Prime Minister from July 2019 to November 2020, had sent an email to Cabinet Office officials informing them that Mr Johnson wanted Mr Raab to take the Quad through an “Escape Plan paper“.107 Drafting was to be worked up that week which Mr Johnson would subsequently review.108 This resulted in proposals, developed by the Cabinet Office C19 Strategy Unit, to moderate lockdown restrictions, including prioritising getting people back to work and reopening schools and non-essential retail when easing the lockdown.109 The Quad approved the advice.110 |
| 5.47. | Mr Johnson was still recovering from Covid-19 and did not attend the Quad meeting.111 However, Sir Mark Sedwill sent the papers considered by the Quad to Mr Johnson as he had requested. He also sent an advice note to Mr Johnson in which he detailed that the papers set out strategic choices for the easing of the lockdown and that they had been reviewed and approved by Mr Raab and “key senior ministers“.112 New operating models were being developed for workplaces, schools, transport, and public and recreational spaces.113 Sir Mark Sedwill identified schools as “the trickiest issue“, with the key question being “whether to re-open (some) schools after Whitsun half-term or keep them all closed until September” – SAGE having advised that “full re-opening would likely tip R back above 1“.114 One significant question posed was whether, in easing the lockdown restrictions, the UK government should:
“target low general incidence, which requires R to stay well below 1, or low serious incidence, i.e. minimise the number of those who have a dangerous not just unpleasant bout [of Covid-19]”.115 Sir Mark Sedwill advised that making a choice about the level of incidence might affect decisions about the speed and prioritisation of easing the lockdown restrictions.116 |
| 5.48. | On 23 April 2020, testing was extended to all essential workers in England and members of their households showing symptoms.117 |
| 5.49. | On 23 April 2020, the Scottish Government published COVID-19 – A Framework for Decision Making.118 This framework recognised four harms that emanated from the virus:
This framework was intended to be integral to the Scottish Government’s decision-making through the pandemic. On the same day, Ms Sturgeon also said that the lifting of restrictions in Scotland was “likely to be phased“, with some measures remaining in place until 2021 “or beyond“.120 |
| 5.50. | The Welsh Government published Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery on 24 April 2020.121 Work had commenced on the framework in early April.122 Mr Drakeford said that this framework “formed the basis for the 21-day reviews that were carried out by Cabinet from 7 May onwards“.123 It summarised the Welsh Government’s approach to lifting restrictions in line with three pillars: (i) how the government would judge the current infection level and transmission rates; (ii) the seven principles that would guide the easing of restrictions (including whether the measure had a “high positive equality impact“); and (iii) how its public health surveillance and response systems would be enhanced to “closely track the virus as restrictions are eased“.124 It outlined the four ways in which the Welsh Government understood that harms could be caused by the virus. These were: (i) direct harm from infection; (ii) harm caused if services, including the NHS, became overwhelmed; (iii) harms from non-Covid-19 illness; and (iv) socio-economic and other societal harms. |
| 5.51. | Having been informed that the peak of deaths per day had occurred on 15 April 2020 and that deaths were starting to decrease, the Northern Ireland Executive agreed on 24 April to permit the first easing of restrictions to allow access to burial grounds for purposes other than funerals.125 A few days earlier, officials had discussed seeking agreement “on a series of tests or principles which will need to apply before any relaxation can begin“.126 |
| 5.52. | On 27 April 2020, Professor Ian Young, Chief Scientific Adviser to the Department of Health (Northern Ireland) from November 2015, established the Strategic Intelligence Group. This group was to synthesise information from SAGE and produce regular analysis specific to Northern Ireland.127 |
| 5.53. | In a bilateral meeting with the Secretary of State for Northern Ireland on 28 April 2020, it was recorded that Michelle O’Neill MLA, deputy First Minister of Northern Ireland from January 2020 to February 2022:
“updated that the NI Executive was beginning to consider post-COVID environment with a focus on recovery planning“.128 Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021, is recorded as having: “noted that other devolved regions had issued recovery plans but NI has yet to do so, reinforcing the importance of regular early engagement and advance warning of HMG [the UK government] direction of travel“.129 |
| 5.54. | In Northern Ireland, more than 1,000 tests were carried out on 23 April 2020.130 The Scottish Government’s target was 3,500 daily tests by the end of April and, by 28 April, it was considered that the target was on course to be met.131 On 21 March 2020, Wales had set a target of 9,000 tests a day by the end of April. However, this was abandoned on 20 April.132 By 23 April, Wales had the capacity for only 1,800 tests a day.133 Mr Hancock had set a target of scaling up testing to 100,000 tests a day in England by the end of April. While Module 7: Test, trace and isolate is exploring whether this target was met, it is clear that testing capacity was significantly expanded during April.134 |
| 5.55. | A meeting of the Covid-19 Strategy Ministerial Group on 30 April 2020 discussed the UK government’s plans to scale up test and trace through the use of an app. Mr Hancock explained that the app would work best when “the overall number of cases was relatively small“.135 |
| 5.56. | Despite the acknowledgement that incidence needed to be low for test and trace to work effectively, the UK government did not explicitly make a decision about whether to ease restrictions in a low-incidence or high-incidence scenario. The consequence was that the government ultimately eased restrictions without defining a level of Covid-19 deaths that it was prepared to tolerate to enable restrictions to be eased without access to a vaccine or medical treatments. |
| 5.57. | Professor McLean explained that the SAGE working group’s “general consensus was that low incidence was preferable” when easing restrictions and implementing an effective test and trace system, given immunity might not be long lasting and to avoid test and trace systems being overwhelmed by new cases.136 She further explained:
“[T]he strategy that the [UK] government in fact adopted post lockdown was to keep R below 1, without taking a view about how many infections were tolerable … Without a commitment to a target level of infections, the aim of keeping below 1 [was] only half a strategy.“137 She said it was only “half a strategy” because setting a target for R was not the only relevant strategic consideration. Identifying a level of infections that the UK government did not wish to be exceeded when restrictions were eased was also a critical strategic consideration. This is due to the fact that the higher the number of infections in the population, the higher the number of deaths – even if R remains below 1. For example, the number of deaths would be much higher if the number of infections in the population was 1 million as opposed to 100, even where R is below 1 in both scenarios. |
| 5.58. | On 27 April 2020, Mr Johnson returned to work fully. The next day, Mr Drakeford wrote to him outlining that the Welsh Government had now published Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery and stated his preference that the steps taken to ease elements of the lockdown would be agreed together and implemented in line with a “common timetable“.138 This reflected the Welsh Government’s framework, which stated:
“The whole of the UK entered ‘lockdown’ in the same ways and at the same time, and our preference as a government would be that all four nations retain a common approach to lifting the restrictions.“139 |
| 5.59. | Mr Johnson subsequently announced on 30 April 2020 that there would be a comprehensive plan set out the following week to restart the economy, reopen schools and for travel to work in England.140 Mr Drakeford said this was “without consultation with the Welsh Government“.141 |
The risk of an exit wave
| 5.60. | Each government was advised about the risk of an exit wave occurring once the lockdown restrictions were lifted, particularly if they were lifted too quickly and at a point at which cases were too high to be controlled by test, trace and isolate capacity. Any exit strategy was obliged to take account of this risk. |
| 5.61. | A Cabinet Secretariat briefing for COBR dated 6 March 2020 had advised that an exit wave was likely to occur if stringent restrictions were implemented and then lifted.142 SAGE had provided advice about the risk of an exit wave on 13 March 2020 and Professor Vallance had raised this directly with Mr Johnson on 14 March.143 Indeed, the risk of an exit wave occurring after stringent restrictions were lifted was a critical factor in the reluctance to impose a lockdown in the first place (see Chapter 3: The first 12 days of March 2020, in this volume). Scientific advisers continued to voice these concerns in the context of easing the first UK-wide lockdown restrictions. A few days later, on 2 April 2020, SAGE advised:
“There is a danger that lifting measures too early could cause a second wave of exponential epidemic growth â�� requiring measures to be re-imposed.“144 |
| 5.62. | On 6 April 2020, in Scotland, a briefing paper prepared for the deep dive meeting into social distancing measures recommended:
“Work on post-peak choices is needed to influence that debate away from simplistic ‘exit’ solutions that risk a massive second peak.“145 |
| 5.63. | Scottish Cabinet minutes dated 14 April 2020 recorded:
“Any move away from the current ‘lockdown’ regime, even partial, should be introduced with great caution. A gradual and systematic relaxation of social distancing would need to go hand-in-hand with a rigorous ‘track, trace, and isolate’ model, whenever new cases were identified, so as to guard against a new ‘second wave’ of infection spreading back into the community.“146 |
| 5.64. | In Wales, the Technical Advisory Cell’s Chief Medical Officer briefing on 31 March 2020 advised that a “second wave is likely if controls are relaxed too early, SAGE will now focus on this“.147 The Welsh Government’s framework specifically addressed the risk of a second wave, stating:
“We will not do anything without being as sure as we possibly can be that we do not risk a second significant wave of infection, and therefore have to re-introduce some restrictions.“148 |
| 5.65. | At the time of the initial relaxation of restrictions in Northern Ireland, the Northern Ireland Executive Committee did not yet have an overarching strategy for its decision-making. The decision to relax restrictions relating to burial grounds appears to have been triggered at the request of individual ministers, rather than as the result of a strategic approach. Nevertheless, it is clear that, in considering that decision, the Executive Committee did take into consideration the potential impact upon transmission and the possibility of a second wave of infections in the autumn.149 Professor Young advised in his first modelling paper dated 1 April 2020 that there would be an exit wave when restrictions were relaxed.150 The Executive Committee was also advised on 15 April that it would be necessary:
“to plan for a potential second wave of Covid-19 cases later in the year, and possibly further waves, once restrictions are eased or lifted and normal life gradually resumes“.151 At the Executive Committee meeting of 24 April, Professor (later Sir) Michael McBride, Chief Medical Officer for Northern Ireland from September 2006, commented that tracking and testing would be “crucially important” in order to avoid a second wave.152 |
Developments in surveillance data
| 5.66. | The Coronavirus (Covid-19) Infection Survey was a UK-wide study initiated by the Office for National Statistics, which ran from April 2020 until March 2023. Its purpose was to provide an understanding of the number of infections in the community, including regional and age breakdowns.153 The survey provided hugely valuable insights into demographic change and infection trends, including the scale of asymptomatic infections.154 It led to the UK being the:
“only country in the world that had a robust estimate of the number of infections at any point in time“.155 From May 2020, the Real-time Assessment of Community Transmission (REACT) study measured the prevalence of Covid-19 in different areas of England – including in people who did not have any symptoms – and provided consistent, representative data on Covid-19 positivity in the community.156 While both the Coronavirus (Covid-19) Infection Survey and REACT captured useful data for use in the pandemic, they started too late.157 |
May 2020: Planning for lifting lockdown
| 5.67. | By May 2020, the Vaccine Taskforce had been established and the Department of Health and Social Care had set up the Therapeutics Taskforce.158 Although Covid-19 vaccines were ultimately rolled out from December 2020 (as is being examined in detail in Module 4: Vaccines and therapeutics), there was considerable uncertainty at this stage about if and when an effective vaccine would be developed. Decisions had to be taken therefore in the context of a deadly virus with no pharmaceutical tools available to stop its spread. |
| 5.68. | The UK government’s Covid-19 Strategy Ministerial Group decided on 1 May 2020 that an announcement should be made recommending the voluntary use of cloth face coverings by members of the public.159 |
| 5.69. | On 2 May 2020, the Cabinet Office advised Mr Johnson that he should set out a roadmap for easing the lockdown.160 This note was the origin of the UK government’s May 2020 Roadmap.161 The Cabinet Office note advised Mr Johnson to announce the following week:
|
| 5.70. | The key elements of the draft roadmap, discussed further below, were agreed that evening at a meeting between Mr Johnson, the Quad and Professors Whitty and Vallance.163 They discussed a “shift from the current stay at home messaging, to balance continued vigilance and gradual easing“, a phased reopening of schools and “an aspirational date for the earliest possible re-opening of non-essential retail“.164 |
| 5.71. | At a meeting on 4 May 2020, Mr Sunak and Mr Johnson discussed non-essential retail reopening in mid-May 2020, schools in early June and hospitality in July.165 |
| 5.72. | On 5 May 2020, SAGE considered the potential impact of the steps in the draft roadmap on transmission of Covid-19. It advised that Step 1 was “unlikely” to push R above 1.166 Step 2 (reopening of primary schools and non-essential retail) was “not likely to push ‘R’ above 1 but this is dependent on having an effective test and trace programme” in place.167 The lifting of further restrictions beyond this, however, was “highly likely” to push R above 1.168 The minutes of its meeting on 7 May noted:
“As steps are taken to ease the lockdown, each step needs to be accompanied by very clear communication of the continued public health justification for remaining restrictions.“169 |
The second review
| 5.73. | The second review of the lockdown restrictions was due by 7 May 2020 in England, Scotland and Wales and by 9 May in Northern Ireland. |
| 5.74. | On 5 May 2020, the Scottish Cabinet agreed that the time did not appear right for any substantive relaxation in lockdown restrictions in Scotland.170 There were estimated to be around 26,000 people in Scotland who were infected and R lay somewhere between 0.7 and 1.0 (with a best estimate of 0.8).171 This was considered to be “insufficiently low to be able to say, with confidence, that the outbreak was under control or to make anything other than marginal changes to restrictions“.172 The Scottish Cabinet also had growing concerns about “a lack of information about what the UK Government was planning, despite repeated requests for updates“.173 It was noted:
“Notwithstanding the advantages of UK-wide alignment (provided the evidence supported it), Scottish Ministers had an overarching responsibility to reach evidence-based decisions that were right for Scotland, and that Scottish Ministers’ legal responsibilities under the relevant legislation could not be outsourced.“174 |
| 5.75. | As at 6 May 2020, 3,934 laboratory-confirmed cases and 418 deaths associated with Covid-19 had been reported in Northern Ireland.175 David Sterling (later Sir David Sterling), Head of the Northern Ireland Civil Service and Permanent Secretary to The Executive Office from June 2017 to August 2020, provided ministers with two options for a roadmap setting out the future lifting of restrictions. The first was a “a three stage illustration of the steps to relaxation of restrictions against six key areas of daily activity“, while the second was a “higher level” five stages proposed by the Department of Health (Northern Ireland).176 |
| 5.76. | At its second periodic review on 7 May 2020, the Northern Ireland Executive Committee was advised that case numbers in Northern Ireland continued to rise but at a slower rate – the curve was flattening.177 If R were to rise above 1, there were two options: to accept a significant increase in cases and deaths; or to reimpose restrictions for four to six weeks.178 Professor Young described R as on a “knife edge“.179 The Executive Committee agreed that ministers should provide further comments and a revised paper should be circulated for consideration the following week.180 The Executive Committee decided to keep the regulations in place.181 At its next meeting on 11 May, further amendments were made to the roadmap paper, which was subsequently agreed by the First Minister and deputy First Minister later that day.182 |
| 5.77. | The second and subsequent 21-day reviews in Wales were undertaken in Welsh Cabinet meetings. The Cabinet considered on 7 May 2020 that “[t]oo early or extensive easement of restrictions could lead to a return of exponential growth of viral transmission“.183 However:
“[T]here were concerns about the indirect harms that arose from lockdown measures, and the potential for disproportionate harms to both socio-economically disadvantaged and younger people.“184 |
| 5.78. | In considering evidence from SAGE that infection rates had “dropped to between 0.6 – 0.8” in Wales, the Welsh Cabinet agreed to some minor changes to the restrictions.185 Mr Drakeford held a press conference to confirm that “the stay-at-home regulations will remain in place until the next review date” but that “people will be able to go outside to exercise more than once a day, but we want people to stay local“.186 |
| 5.79. | Mr Johnson met with the Quad on 6 May 2020 to discuss the second review of the lockdown restrictions due to take place the following day and to discuss again the plan for the easing of the lockdown in the coming months. They agreed to present to the Cabinet that the formal review indicated that existing measures remained necessary.187 The following day, the UK Cabinet was, in effect, asked to approve a decision that had already been made by Mr Johnson and the Quad. |
Easing restrictions
| 5.80. | At the same Quad meeting on 6 May 2020, it was also agreed that the first step in easing restrictions should be a direction to return to work for those who could not work from home. The second step of the reopening of non-essential retail and phased reopening of schools was targeted for 1 June 2020, although secondary schools would not reopen until September 2020 at the earliest. An “aspirational” date of 4 July 2020 was agreed for reopening hospitality.188 The UK Cabinet agreed on 7 May that lockdown restrictions should continue and discussed the general approach proposed to ease the lockdown in England.189 |
| 5.81. | On 10 May 2020, the day before the May 2020 Roadmap was published, the UK Cabinet was informed of the details of the plans for easing the first lockdown in England, as well as plans to introduce travel quarantine.190 The Cabinet was again asked to approve a decision that had already been made by Mr Johnson and the Quad. |
| 5.82. | Mr Johnson then chaired a COBR meeting, attended by the leaders of the devolved administrations.191 A paper was presented setting out the steps in the draft roadmap that the UK government planned to take in easing the lockdown in England.192 Mr Gove had outlined the likely content of the roadmap to the First Ministers of Wales, Scotland and Northern Ireland three days before its publication.193 At COBR, the discussion recognised:
“that it may be appropriate for difference in approach/speed depending on the scientific evidence but messaging was crucial and should not undermine the Four Nations approach or stay at home messaging“.194 COBR agreed the importance of: “continuing a UK-wide four nations approach to controlling the spread of the virus … acknowledging the spread of the disease may mean differentiations in approach“.195 COBR also outlined plans for the introduction of travel quarantine at the UK border and for the establishment of a new Joint Biosecurity Centre that would analyse data on Covid-19 infection rates across the UK.196 The centre was subsequently established in May 2020 to provide a single point of public health analysis in order to advise the Prime Minister, UK Cabinet and others.197 This also clarified whose role it was to collate pandemic-related health data.198 The Joint Biosecurity Centre became a command and control centre for the data received from health services across the UK, the Office for National Statistics and technology companies.199 |
| 5.83. | Mr Johnson also confirmed to COBR the UK government’s intention to change its messaging to ‘Stay Alert’, although he also said that its core messaging would remain that the public should stay at home.200 Mr Johnson suggested that divergence of messaging across the UK would be “fine as the leaders of each part of the UK needed to tailor their message to the individual circumstances that they faced“.201 |
| 5.84. | The devolved administrations retained the express message to stay at home.202 This was the first point of substantive divergence in the responses in the four nations. Mr Drakeford did not agree to the change to Stay Alert because the Welsh Government had “no prior notice, no sharing of the basis on which the change had been made, no ability to explain to me what the new message was meant to convey to anybody“.203 Baroness Foster explained that the message was not changed in Northern Ireland, in part due to the higher R number in Northern Ireland at the time.204 Ms O’Neill reflected that the Stay Alert messaging was also “less clear and more abstract“.205 Ms Sturgeon considered that the change in message was premature, since:
“data … suggested the R number remained high and, at that time, was possibly higher in Scotland than in other parts of the UK. Given that we still lacked effective treatments and vaccines, I feared that making such a change at that time would cause infection rates to increase again and that this would cause more severe illness, put more pressure on the NHS and, ultimately, cost lives.“206 |
| 5.85. | In answering questions at the Covid-19 briefing (before Mr Johnson had made his announcement) about why the Scottish Government was not taking the same decision as the UK government, Ms Sturgeon was critical of the UK government’s new core public message. She said that she did not know what ‘Stay Alert’ meant and:
“For Scotland right now, given the fragility of the progress we have made, given the critical point we are at, it would be catastrophic for me to drop the ‘stay at home’ message, which is why I am not prepared to do it … particularly in favour of a message that is vague and imprecise.“207 |
| 5.86. | Ms Sturgeon told the Inquiry that she did not set out to be explicitly critical of Mr Johnson but acknowledged that it was “inevitable” that her comments would be interpreted in that way.208 She described this as “the first point of public disagreement” and said:
“The only way I could have avoided this was to quietly acquiesce in a decision that I thought to be misguided. That would have been a serious abdication of my responsibilities to the Scottish people.“209 |
| 5.87. | Ms Sturgeon’s comments at the Covid-19 briefing were not well received within the UK government. Mr Gove considered her comments “unhelpful” and “premature“.210 He said that he was “concerned about the presentational impact these interactions had on the public, and the impact it may have on public adherence to measures and regulations“.211 |
| 5.88. | That evening, Mr Johnson announced the publication of the UK government’s May 2020 Roadmap.212 He explained that its provisional dates were conditional on meeting the five tests set out by Mr Raab on 16 April 2020, which would be supported by a new Covid Alert System run by the new Joint Biosecurity Centre.213 Mr Johnson also outlined the new public health messaging for England: “stay alert, control the virus and save lives“.214 That same day, Professor Vallance recorded in his evening notes:
“I have clearly said that the proposal to open as much as possible will push R > 1 Chris and I both made it very clear that we think speed and timescale too fast.“215 |
| 5.89. | The May 2020 Roadmap confirmed the following provisional dates for the easing of the first lockdown in England:
No further steps were set out beyond 4 July.219 |
Figure 16: UK government steps of adjustment to current social distancing measures
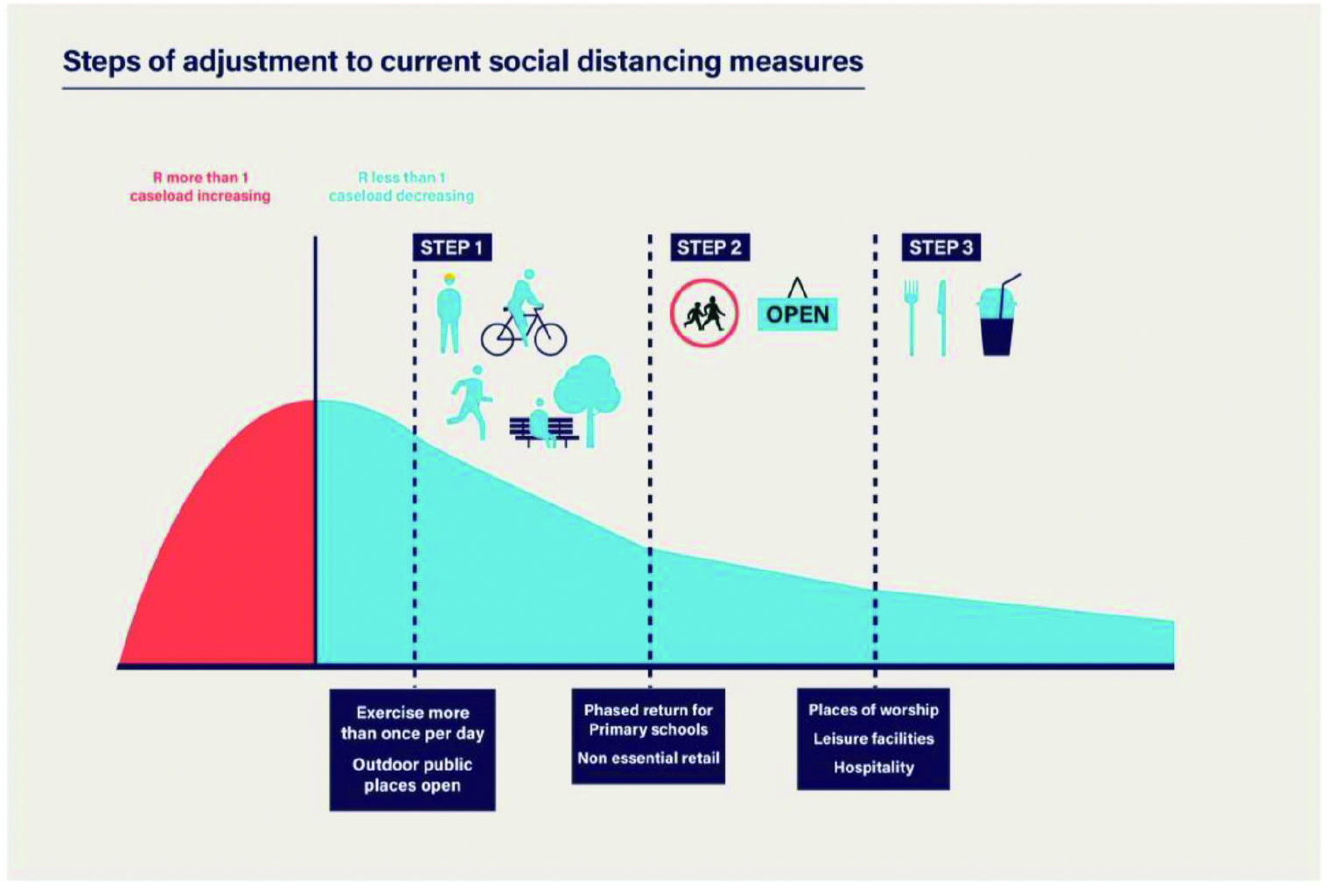
Source: Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020, p21, Figure 6 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892)
| 5.90. | Helen MacNamara, Deputy Cabinet Secretary from January 2019 to February 2021, said that the May 2020 Roadmap “created the framework for all subsequent decision making” in England and that it “probably was the most useful thing that was produced in those early months“.220 Ms MacNamara had raised a number of concerns about the content of the first draft shared on 6 May 2020, noting that there had not been “any debate or advice about the policy or choices“.221 |
| 5.91. | The May 2020 Roadmap was published on 11 May, a full seven weeks after the first UK-wide lockdown had been announced on 23 March 2020. This was too long and reflected the lack of advance planning for the implementation of stringent restrictions and therefore how those restrictions might later be eased. Lord Sedwill told the Inquiry that there had been “intensive” debate about the May 2020 Roadmap. He said that it was developed:
“through the course of April, when the Prime Minister was away, under the leadership of the First Secretary [Mr Raab] in a series of ministerial meetings known as the quad, the chairs of the MIGs [Ministerial Implementation Groups], with some input from other ministers“.222 Stuart Glassborow (Deputy Principal Private Secretary to the Prime Minister from May 2019 to May 2022) described it as being “led by the Cabinet Office, co-ordinating across other departments“, with the Quad working on the “key elements … over several meetings” before agreeing it on 2 May 2020.223 Ms MacNamara said the May 2020 Roadmap “was probably read by fewer than 30 people before it was published“, due to concerns about leaking.224 Despite its significance, only a small group of advisers and decision-makers were involved in its development or scrutiny. Wider scrutiny – for example, by the UK Cabinet – would have been beneficial to ensure its proposals and their potential impacts on health, the economy and society had been robustly tested. |
| 5.92. | On 13 May 2020, Step 1 of the May 2020 Roadmap commenced in England. Amendments were made to the law to allow people to leave their homes to exercise with one or more members of their own household or with one person from another household.225 Those who could not work from home were encouraged to return to work. |
| 5.93. | On 15 May 2020, the Welsh Government published Unlocking Our Society and Economy: Continuing the Conversation.226 This was intended to build on the April 2020 Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery.227 It set out a ‘traffic light’ guide for easing the lockdown and provided an overview of restrictions – ‘lockdown’, ‘red’, ‘amber’ and ‘green’ (of which ‘green’ represented the least restrictive measures). It specifically referenced the UK government’s May 2020 Roadmap and stated that the challenges presented by Covid-19 were “the same as those which confront the rest of the United Kingdom“.228 Unlike the UK government’s plan, no dates were indicated for the relaxation of restrictions. However, the document clearly outlined the reasons why the Welsh Government believed it could “only move forward cautiously” and confirmed that “we have to reduce the number of new cases by keeping the transmission rate (R) below 1“.229 |
| 5.94. | The Northern Ireland Executive had published its Coronavirus: Executive Approach to Decision-Making on 12 May 2020.230 No restrictions were removed at this point and the Executive Committee declined to set provisional dates for the relaxation of specific restrictions. Professor McBride explained that the approach should be guided by “data not dates” and that any consideration of further relaxations should only be given once the impact on community transmission of previous relaxations could be fully assessed.231 The Coronavirus: Executive Approach to Decision-Making therefore set out a number of key guiding principles for the regular reviews and consideration of easing restrictions, including the need to control transmission when there was a reasonable prospect of maintaining R at or below 1 and protecting healthcare capacity. |
| 5.95. | On 21 May 2020, the Scottish Government published Scotland’s Route Map Through and Out of the Crisis.232 This was a more detailed, evidence-led, four-phase plan, laying out the order in which restrictions would be relaxed and the criteria that would need to be met to move out of each phase, consistent with the Scottish Government’s cautious approach to removing restrictions. Details of plans for Phase 1 included allowing people to meet outside with people from one other household from 28 May 2020, subject to the number of new cases of Covid-19 continuing to fall. Plans also included schools reopening on 11 August 2020, with a “blended model” of part-time study at school combined with some learning at home.233 |
| 5.96. | The devolved administrations proposed, in broad terms, more cautious approaches to easing the lockdown than the one announced by the UK government in England. |
The third review
| 5.97. | The third review of lockdown restrictions was due to take place by 28 May 2020 in England, Scotland and Wales and by 30 May in Northern Ireland. In England, in line with the May 2020 Roadmap, Step 2 was due to be implemented no earlier than 1 June 2020. On 18 May, the UK government announced that everyone in the UK with symptoms of Covid-19 would now be eligible to book a test.234 |
| 5.98. | On 21 May 2020, SAGE advised that test, trace and isolate could quickly be overwhelmed by new cases if the restrictions were eased at a time when there was a relatively high level of incidence and prevalence of Covid-19 in the population.235 The Covid-19 Dashboard dated 21 May 2020 recorded that laboratories were processing around 41,099 tests a day.236 SAGE stated:
“[T]he lower the number of infections at the point when measures are lifted, the better this would be in terms of managing the epidemic. Not only would there be fewer people being infected, becoming ill and dying but: contact tracing and testing capacities are less likely to be overwhelmed.“237 |
| 5.99. | SAGE warned that if test, trace and isolate was overwhelmed, “re-imposition of significant NPIs [non-pharmaceutical interventions]” would be “the only way to regain control of the epidemic“.238 Further, in terms of the implementation of Step 2 of the May 2020 Roadmap planned for 1 June 2020 in England, SAGE considered modelling produced by the Scientific Pandemic Influenza Group on Modelling (SPI-M) of various easing scenarios and advised in relation to further easings that “[w]ith schools closed and R 0.7-1.0, as now, there is little headroom with no contact tracing in place“.239 Additionally, the figures it was considering did not take into account any changes that had resulted from the easings in Step 1.240 SAGE was strongly of the view that it was too risky to make any further easements on 1 June, especially when “track and trace” would only just be getting up and running at that stage. In its view, it was better to wait a further month.241 |
| 5.100. | Mr Johnson informed the UK Cabinet on 21 May 2020 that it was unlikely that the full easing of restrictions planned for 1 June 2020 could be implemented, given the impact this would have on R.242 That same day, Professor Vallance recorded in his evening notes:
“PM talked about caution etc and then said, ‘Yes, we must go ahead with breezy confidence and get this country going again.’ Both CW [Professor Whitty] and I rather shocked by breezy confidence.“243 |
| 5.101. | A few days later, on 25 May 2020, the UK Cabinet considered a proposal that Step 2 of the May 2020 Roadmap be implemented in two phases, with early years settings and certain year groups returning to school on 1 June 2020. Some other year groups and the remainder of non-essential retail would follow on 15 June.244 This timetable was approved.245 Professor Vallance recorded in his evening notes that Mr Johnson “seems very bullish and wants to have everything released sooner and more extremely than we would“.246 |
| 5.102. | On 25 May 2020, Mr Cummings held a press conference in the garden of 10 Downing Street in which he made a statement concerning his trip to Durham and Barnard Castle on 12 April 2020. He also answered questions about whether this had breached the lockdown rules.247 The impact of alleged rule-breaking by advisers and decision-makers is examined in Chapter 11: Government decision-making, in Volume II. |
| 5.103. | On 26 May 2020, Professors Whitty and Vallance, Professor (later Dame) Jenny Harries (Deputy Chief Medical Officer for England from July 2019 to March 2021) and Professor (later Sir) Jonathan Van-Tam (Deputy Chief Medical Officer for England from October 2017 to March 2022) wrote to Simon Case (later Lord Case), Permanent Secretary at 10 Downing Street from May to September 2020. They warned of the risk of easing restrictions in the absence of a central body with oversight of the cumulative impact of cross-government decisions.248 |
| 5.104. | Mr Johnson was advised by Cabinet Office officials on 27 May 2020 that the rules in England should be changed at the third review to allow gatherings of up to six people outdoors, while maintaining restrictions on gatherings indoors.249 He also received a paper outlining decisions to be made in relation to the proposed reopening on 1 June 2020 of schools and to non-essential retail, social contact, shielding and outdoor spaces.250 |
| 5.105. | On 28 May 2020, Mr Johnson announced that, from 1 June 2020, up to six people would be allowed to meet outside while observing social distancing rules. He also confirmed the reopening of nurseries, early years settings and years one and six would go ahead on 1 June, with some other year groups returning from 15 June. The reopening of most non-essential retail would be delayed until 15 June.251 That same day, Ms Sturgeon announced the move in Scotland to Phase 1 of Scotland’s Route Map Through and Out of the Crisis, beginning on 29 May 2020.252 With deaths and new cases having fallen in Wales and fewer people in critical care beds, the Welsh Cabinet agreed to change its messaging to ‘Stay Local’ (using within five miles of home as a “rule of thumb“) and agreed that two households could meet outside.253 These changes were announced on 29 May and came into effect on 1 June 2020.254 |
| 5.106. | An Executive Paper dated 28 May 2020 from the Department of Health (Northern Ireland) recommended that the existing restrictions in Northern Ireland be amended to allow marriages and civil partnerships to be conducted outdoors (subject to a limit of 10 people), the opening of outdoor sports courts and the conduct of business by outdoor, non-food retailers and certain larger, non-food retail outlets.255 The Executive Paper recommended that the proposed amendments ought not to take effect until the week commencing 8 June 2020, subject to R remaining at or below 0.9 at that time. It further advised that the matter should be discussed at an Executive Committee meeting on 4 June, at which time a final decision could be made.256 The proposed course was agreed by the Executive Committee at its meeting of the same day.257 At that meeting, Mr Swann advised that “we are in position to ease restrictions as agreed“, noting that R was 0.7/0.9.258 Notes of the meeting indicate that Mr Swann also advised that Northern Ireland was “in a position to cope with 2nd surge” and that “if we are in position on 18 June … cd [could] move to next steps“.259 The Executive Committee confirmed that, in light of the rate of R at that time, the amendments previously considered at its meeting on 28 May should be implemented in the week commencing 8 June.260 |
| 5.107. | Also in Northern Ireland, a decision to scale back the NI Hub (Northern Ireland’s coordination centre) had been made a week earlier.261 Similarly, the Civil Contingencies Group (Northern Ireland) was meeting less frequently.262 The rationale for scaling back these arrangements was the downward trend in infection levels and the corresponding reduction of pressure on hospitals in Northern Ireland at that time.263 By 29 May 2020, hospital admissions in Northern Ireland were the lowest they had been since March 2020.264 |
Organisational changes
| 5.108. | As considered in more detail in Chapter 11: Government decision-making, in Volume II, a number of structural changes were also introduced around this time. |
| 5.109. | From 15 May 2020, the Covid-19 Strategy Ministerial Group meeting became known as the Covid-19 Dashboard meeting, also chaired by Mr Johnson.265 The Ministerial Implementation Groups were disbanded on 28 May.266 The Covid-19 Strategy Committee (Covid-S) and Covid-19 Operations Committee (Covid-O) were established to replace them.267 Mr Johnson was to chair Covid-S, which would consider strategy and first met on 4 June 2020.268 Covid-O would drive the policy and operational aspects of the response and was chaired by Mr Gove.269 Its first meeting was on 29 May.270 |
| 5.110. | Mr Johnson had been advised by Ms MacNamara and Mr Case that major decisions were still to be taken by the UK Cabinet.271 A Joint Ministerial Committee was to be convened to “manage conversations with the DAs“.272 However, this was ultimately not convened. |
| 5.111. | The Covid-19 Taskforce was created at the end of May 2020.273 It was initially led by Mr Case, who was therefore responsible for leading on advice for easing the first lockdown in England.274 It was formed as a result of the recommendation in Ms MacNamara’s review that a unit was required in the Cabinet Office to provide strategic leadership on the response and advise decision-makers on the development of strategy and the probable health, economic and societal consequences of any potential decision.275 It served as the secretariat for Covid-S and Covid-O and commissioned the papers and agendas for their meetings.276 |
June 2020: Reopening
| 5.112. | On 1 June 2020, as announced, it became lawful for six people to meet outside in England. It remained illegal to meet indoors with anyone from a different household.277 Part of Step 2 of the May 2020 Roadmap was implemented in England, with early years childcare and certain year groups returning to school on 1 June and the reopening of outdoor markets and car showrooms. |
| 5.113. | Contact tracing in Wales also commenced on 1 June 2020.278 On the same day, the Northern Ireland Executive Committee confirmed that hotels and other tourist accommodation would be permitted to reopen from 20 July 2020 and that, from 8 June, those shielding would be able to go outside. However, this was noted to be subject to “controlling the rate of transmission of the virus“.279 |
| 5.114. | At a UK Cabinet meeting on 2 June 2020, Mr Johnson commissioned a review of the two-metre social distancing rule.280 Professor Vallance explained that measures could be taken to mitigate the impact of reducing the distance, including wearing of a face covering.281 Mr Johnson told the Inquiry that his support for the introduction of the wearing of face coverings on public transport was primarily a public messaging device, rather than because of the effect they might have on preventing transmission of Covid-19.282 The Inquiry notes that this rationale was equally applicable before June 2020. Some witnesses to the Inquiry believed that the UK government should have required face coverings to be worn at an earlier stage.283 |
| 5.115. | Kirsty Williams MS, Minister for Education in the Welsh Government from May 2016 to May 2021, announced on 3 June 2020 that schools would reopen on 29 June to give the opportunity for all students to return before the summer holidays. Students would return in phases with staggered starts, lessons and breaks – with at most a third of pupils present in schools at any one time.284 Module 8: Children and young people is considering whether this plan came to fruition. |
| 5.116. | On 4 June 2020, SAGE confirmed its advice that two metres for social distancing should continue to be observed, noting that “1m [one metre] separation carries 2-10 times the risk of 2m separation“.285 Noting that shorter distances presented higher risk, SAGE stated:
“Other mitigations … should particularly be considered where it is necessary for people to be closer than 2m for a prolonged period, or where someone has multiple, frequent interactions with others at a shorter distance.“286 |
| 5.117. | That same day, at its first meeting, Covid-S agreed that the social distancing guidance should be reviewed.287 Mr Sunak had written to Mr Johnson on 3 June 2020, urging him to reopen outdoors hospitality on 22 June 2020, followed by all hospitality on 4 July 2020. He stated: “We need flexibility around the 2m rule to ensure the businesses we want to reopen are viable.“288 |
| 5.118. | A paper presented to Covid-S explained the important remaining strategic choice in the UK government’s approach to easing the lockdown restrictions in England related to incidence. It outlined that incidence in the UK was higher than in other countries, such as Germany, Italy and Spain, which were pursuing similar strategies to that proposed by the UK government in its May 2020 Roadmap – moving from national lockdowns to more targeted and local restrictions. Those countries had fewer than 700 confirmed cases per day, compared to 1,600 in the UK with estimated cases of about 10,000.289 It explained that easing restrictions when incidence was still high was undesirable as it would lead to more deaths from Covid-19, that test and trace would be harder to deliver and that the risk of a second peak would be increased. The paper outlined: “In the Government’s current strategy, a vaccine or game-changing treatment provide the only route out of the epidemic.“290 It stated that Covid-S would be asked to make a decision the following week about whether the strategy to ease the lockdown in England should proceed on the basis of levels of incidence rather than dates. If reducing incidence were to be prioritised, this would lead to the restrictions being eased more slowly than they would be if minimising the economic and other costs of the restrictions were to be prioritised. |
| 5.119. | However, the evidence received by the Inquiry indicates that Covid-S did not reconvene again until 19 June 2020 and did not consider this strategic issue at that meeting.291 Ultimately, no target level of cases was incorporated by the UK government into its strategy for easing restrictions in the summer of 2020. Instead, the government sought to try to release restrictions gradually to reduce the economic and social impact of the pandemic, while still retaining enough restrictions to keep R below 1. |
| 5.120. | On 5 June 2020, the World Health Organization updated its guidance to advise that governments should encourage the public to wear face coverings in specific settings.292 It stated that, although widespread use of face coverings was “not yet supported by high quality or direct scientific evidence“, the clear knowledge of pre-symptomatic and asymptomatic transmission supported the public being encouraged to wear face coverings in settings where social distancing could not be consistently achieved.293 In Wales, Dr Atherton recommended that non-medical face coverings should be worn by the public in “moderately risky (confined indoor spaces)“, but he remained of the view that “the evidence of benefits does not justify a mandatory or legislative process“.294 This position was supported by the Technical Advisory Cell.295 On 9 June 2020, the Welsh Government recommended – but did not mandate – face coverings in areas where social distancing could not be maintained.296 |
| 5.121. | On 7 June 2020, no new deaths had been recorded for Scotland or Northern Ireland over the most recent 24-hour period. This was the first time Scotland had recorded no new deaths since lockdown began in March 2020.297 The UK government’s Covid-19 Dashboard recorded on 8 June that there were 1,205 new daily cases in the UK and 55 daily deaths.298 |
| 5.122. | The UK government and devolved administrations all passed regulations that came into force on 8 June 2020, requiring all travellers entering the UK from overseas to self-isolate for 14 days on arrival.299 |
The fourth review
| 5.123. | The next review of restrictions took place on 17 June 2020 in Wales, on 18 June in Northern Ireland and Scotland and on 23 June in England. The divergence in review dates was the consequence of a UK government decision at the end of May 2020 to extend its maximum review period for the lockdown regulations in England from 21 to 28 days.300 |
| 5.124. | On 9 June 2020, Mr Johnson informed the UK Cabinet that the further easing of restrictions, including those affecting non-essential retail and the return of other year groups to schools, would take place in England on 15 June.301 This was announced by Mr Johnson the following day. He explained that it would not be possible to reopen primary schools for all pupils before the summer holidays because:
“the rate of infection is not yet quite low enough, and because we are not able to change our social distancing advice including smaller class sizes in schools“.302 |
| 5.125. | On 11 June 2020, Professor Young explained the potential impact of further easing restrictions to the Northern Ireland Executive Committee. He suggested that the system in Northern Ireland could tolerate R at higher than 1 for a few months. If R reached 1.2, it could just about cope, but not if R went to 1.3.303 Professor McBride regarded the position as finely balanced. The purpose of this meeting was to agree a strategic approach to decisions around easing Covid-19 restrictions. The Executive Committee agreed that information presented to the Executive could be published to increase public understanding of the progress of the pandemic, the measures being taken to mitigate against it and the context within which the Executive was considering easing restrictions. It was agreed that the matter of household visits would be discussed further at the Executive Committee meeting of 15 June 2020.304 |
| 5.126. | On 15 June 2020, Diane Dodds MLA, Minister for the Economy in Northern Ireland from January 2020 to June 2021, presented an Executive Paper setting out proposals for reopening the wider tourism and hospitality industry around 3 July 2020.305 The paper noted that the conditional reopening date for tourism and hospitality in England had been brought forward to 4 July and that the Scottish Government had announced that reopening in Scotland would take effect from 15 July.306 Dates in respect of reopening in Wales had not yet been announced. It further noted that, when the Northern Ireland Executive had agreed the provisional reopening date of 20 July for tourist accommodation, this brought Northern Ireland into alignment with the Republic of Ireland. However, the Irish government had subsequently also brought forward the reopening of tourism and hospitality to 29 June 2020.307 At its meeting the same day, the Executive Committee agreed to the timeframe set out in Ms Dodds’ proposal, noting that “this would be conditional on the continued containment of the spread of COVID-19“.308 Notes of the meeting indicate that Professor McBride advised:
“Paper DFE [Department for the Economy (Northern Ireland)] – early July, carries risk – spread of virus. Conditional, can be reversed. Risks – but also societal costs to economy … Exec wd [would] need to be satisfied with mitigation.“309 |
| 5.127. | On 15 June 2020, the remainder of Step 2 of the May 2020 Roadmap was implemented in England.310 The remaining year groups returned to school and non-essential retail was permitted to reopen. It was also made an offence to not wear a face covering on public transport in England.311 |
| 5.128. | On 16 June 2020, the Scottish Government Covid-19 Advisory Group provided further advice to the Scottish Government.312 Under the heading ‘Long Term Strategy’, it stated:
“There is a need for greater overall clarity as to whether the approach that the Government is pursuing is still one of containment or elimination … elimination would require UK-wide strict border controls (currently centred on self-quarantine). These would be needed for arrivals from every country with COVID-19 – likely to be a large number in the foreseeable future. The Group considers this cannot be a Scotland only aspiration, and that the aim is to suppress the virus to as low a level as possible.“313 |
| 5.129. | The following day, Professor Devi Sridhar, Professor of Global Public Health at the University of Edinburgh and a member of the Scottish Government Covid-19 Advisory Group, sent an advisory note to Ms Sturgeon.314 The note set out how:
“using existing capacity within Scotland, a major push for elimination could be made in July. Elimination being a continual push to zero infections in Scotland and elimination of any clusters emerging.“315 Ms Sturgeon suggested that she call Professor Sridhar during the course of that week to discuss this further.316 As discussed further in Chapter 6: The second wave, in this volume, and Chapter 12: Public health communications, in Volume II, the language of ‘elimination’ was inaccurately used by Ms Sturgeon during this period. This gave the impression to the public that the pandemic might imminently be over in Scotland, without recognising the risks of the second wave.317 |
| 5.130. | When the Welsh Cabinet undertook its review on 17 June 2020, deaths from Covid-19 in Wales were the lowest they had been for six weeks.318 The Cabinet decided that, from 22 June, non-essential retail could reopen, subject to social distancing.319 In his written statement following the review, Mr Drakeford confirmed that, while the Stay Local requirement remained in place: “We will however, make it clear that travel outside a person’s local area is permitted on compassionate grounds.“320 On 19 June, Dr Atherton’s advice was to “take advantage of the summer months where there are more opportunities to be outdoors in the open air“.321 |
| 5.131. | On 18 June 2020, Ms Sturgeon announced the move to Phase 2 of Scotland’s Route Map Through and Out of the Crisis, with a staged introduction of changes commencing on 19 June.322 |
| 5.132. | The Northern Ireland Executive’s fourth review of the restrictions also took place on 18 June 2020. The Department of Health (Northern Ireland) advised that, while earlier easements had not increased R above 1:
“[A]s yet there is no signal in relation to more recent easements though in some cases it remains too early to measure the impact.“323 R was estimated at between 0.6 and 0.9.324 The conclusion of the Department of Health (Northern Ireland), supported by Professors McBride and Young, was that, at that time, each of the restrictions and requirements was still needed.325 At the Northern Ireland Executive Committee meeting that day, Professor McBride indicated that community transmission was at a “low level” but cautioned about the need to prepare for a re-emergence of the virus.326 Mr Swann is recorded as saying: “Epidemic not over, proceed with caution. In a good place. Recomm no major changes today.“327 In line with the advice from the Department of Health (Northern Ireland), the Executive Committee did not agree to any further relaxations.328 On 19 June, Northern Ireland had its first day on which no new Covid-19 cases were reported.329 The Northern Ireland Executive subsequently agreed an indicative timeline of further relaxations during June, July and August 2020, which would be implemented if R remained below 1.330 |
| 5.133. | There were increasing concerns about the risk of a second wave. On 21 June 2020, Thomas Shinner, Adviser to the Prime Minister from March to July 2020, sent Mr Case and Simon Ridley, Director General for Policy and Strategy on the Covid-19 Taskforce from May 2020 to July 2021, a note on action that could be taken to prepare for a second, winter wave of Covid-19.331 It stated:
“I think we are more vulnerable to a second wave of COVID than is apparent … and that too few people across Whitehall are yet focussed on these problems.“332 |
| 5.134. | Covid-S met on 22 June 2020 and agreed to proceed with Step 3 of the May 2020 Roadmap in England on 4 July 2020.333 Prior to the meeting, Professor Whitty had raised concerns with the Covid-19 Taskforce that Step 3 was too far skewed in favour of reopening everything.334 At the meeting, he stated that Step 3 was:
“at the top end of the risk boundary … although this package … should not push ‘R’ above one, taken together with the reopening of schools in September, it was more likely than not to do so“.335 Professor Whitty underlined that the “most risky areas of the package were indoor hospitality and the prospect of reopening schools in September“.336 A note made by Professor Vallance after the meeting recorded that Professor Whitty had told Covid-S that “this is high risk and you are treading the line between high risk and being foolhardy“.337 |
| 5.135. | However, Mr Johnson told Covid-S that the “five tests the Government had set were met” and that there was agreement to proceed with the “bold and well-justified” Step 3 package, which, in his opinion, “represented a sensible and cautious approach to opening up the economy“.338 At this time, as acknowledged in a paper presented at the meeting, the effect of the Step 2 easings made on 15 June 2020 would not be fully known before Step 3 was implemented and:
“The incidence and prevalence of the disease in the UK remains higher than in most other European countries which have eased their lockdowns.“339 |
| 5.136. | Moving to Step 3 and the reduction in social distancing from two metres to ‘one-metre plus’ was approved by the UK Cabinet on 23 June 2020, despite Professor Whitty reiterating his concerns that this took the UK government “to the high end of the risk curve“.340 Mr Johnson announced that day that Step 3 would be implemented on 4 July 2020.341 |
| 5.137. | On 22 June, face coverings became mandatory on public transport in Scotland.342 |
| 5.138. | On 30 June 2020, Ms O’Neill, Conor Murphy MLA, Minister of Finance from January 2020 to October 2022, Carál Nà ChuilÃn MLA, Minister for Communities from June to December 2020, and other senior Sinn Féin politicians attended the funeral of Bobby Storey in Northern Ireland. The impact of alleged rule-breaking by advisers and decision-makers is examined in Chapter 11: Government decision-making, in Volume II. |
Reducing the two-metre rule
| 5.139. | Following his letter to Mr Johnson on 3 June 2020 concerning the reopening of hospitality, Mr Sunak again urged Mr Johnson on 8 June to change the social distancing guidance “to 1m as soon as practically possible to ensure the viability of businesses as sectors begin to reopen“.343 In his letter, Mr Sunak expressed his view that “the UK is fast becoming an outlier internationally … there are at least 24 countries who provide for flexibility to go below 2m“.344 |
| 5.140. | Mr Case, Professors Whitty and Vallance and Clare Lombardelli, Chief Economic Adviser at the Treasury from April 2018 to April 2023, agreed to conduct a review of the social distancing guidance.345 At a SAGE meeting on 4 June 2020, the same day as Covid-S’s decision to review the two-metre social distancing rule, it was confirmed that SAGE continued to advise that two-metre social distancing should be observed wherever possible, given that a reduction to one metre would carry two to ten times the risk of two-metre distance.346 At a meeting on 5 June 2020 with Treasury officials, Professor Whitty advised that reducing social distancing guidance to “less than 2m on hospitality would have a big impact on R“.347 |
| 5.141. | In WhatsApp messages on 11 June 2020, Mr Johnson and Mr Case discussed the timing of the social distancing review. Mr Johnson said that the review needed to be concluded “in good time for July 4“.348 Mr Case confirmed that he would “conclude the ‘review’ next Friday“, after which Mr Johnson could:
“consider conclusions on 22/23 June and then we announce our intention, assuming incidence continues to fall, to drop to 1m from 4 July“.349 It is clear from this WhatsApp exchange that Mr Johnson had decided from the outset that the guidance on social distancing should be reduced from two metres. This was most probably to allow for the implementation of Step 3 on 4 July 2020, so that businesses, including hospitality, could reopen in an economically viable way. He had been urged by Mr Sunak to ensure this.350 Mr Case told the Inquiry he approached the review with an open mind.351 However, he conceded that he was under political pressure to conclude that social distancing should be reduced to one metre.352 |
| 5.142. | On 14 June 2020, in his evening notes, Professor Vallance recorded:
“On Friday the 2M rule meeting made it abundantly clear that no one in no 10 [10 Downing Street] or CO [Cabinet Office] had really read or taken time to understand the science advice on 2M. Quite extraordinary.“353 |
| 5.143. | SAGE had already advised on 4 June 2020 that two-metre social distancing should continue to be observed, noting that “1m separation carries 2-10 times the risk of 2m separation“.354 Despite this, the UK government’s social distancing review concluded that guidance should change “to state that 2m or 1m with risk mitigation (where 2m is not viable) are acceptable“.355 Risk mitigation related to the use of measures such as face coverings. The review said that there were “severe economic costs to maintaining 2m distancing” as it was not financially viable for many businesses to reopen on 4 July 2020 with two-metre distancing.356 Mr Johnson explained: “It was clear that the economic costs of maintaining two metres social distancing were severe.“357 He also told the Inquiry that, when reaching the decision to reduce the social distancing guidance: “I did not place more emphasis on the economy than public safety; public health always remained my priority.“358 |
| 5.144. | However, Professor Vallance told the Inquiry:
“[T]he economic arguments for reducing the guidance on social distancing were advanced forcefully and presumably were a powerful influence on the decision that was made.“359 Similarly, Professor Whitty confirmed that “the driver was the stated economic impact of the 2 metre rule“.360 Professor Van-Tam said that the decision to change the social distancing guidance, rather than being based on scientific advice, was: “entirely about the impact that the two-metre rule was having on the economy generally and the hospitality sector specifically“.361 |
| 5.145. | In mid-June 2020, the Northern Ireland Executive Committee considered a proposal to reduce social distancing from two metres to one metre.362 Professor McBride was recorded as having said that he was “extremely uncomfortable with [a] move to less than 2m“.363 |
| 5.146. | Mr Drakeford said that he first heard of the UK government’s intention to reduce the social distancing guidance from two metres in a call with Mr Gove on 23 June 2020. He said the underlying evidence had not been shared with the Welsh Government.364 It retained the two-metre social distance. Mr Drakeford said that the rule had been “a cornerstone of the Welsh Government’s successful effort to persuade the public of the need to adhere to a small number of tangible actions” and to change it might have confused the Welsh Government’s messaging.365 He also confirmed that “no one at all, of whom I was aware, argued that 2m distances did not provide greater protection“.366 |
| 5.147. | There had been discussion within the Scottish Cabinet on 16 and 23 June 2020 about whether it might be “safe” to reduce social distancing from two metres to one metre.367 The Scottish Government received advice from the Scottish Government Covid-19 Advisory Group in draft form on 29 June that focused on the possibility of limited exceptions to the two-metre physical distancing rule in different settings.368 The draft advice noted that the final decision would be a matter of policy for the Scottish Cabinet. This was because considerations of physical distancing requirements were not a binary discussion of what was either safe or unsafe, but required to be weighed up against the likely combined effect of the policy choices on the four harms recognised in the Scottish Government’s COVID-19 – A Framework for Decision Making.369 On 2 July 2020, Ms Sturgeon announced that the two-metre rule would remain, with exemptions in Phase 3 of Scotland’s Route Map Through and Out of the Crisis for certain sectors such as hospitality and retail, which could choose to operate with a one-metre distance on the condition that agreed mitigations were implemented.370 Ms Sturgeon explained that these exemptions were created because of the “serious economic implications” of the two-metre rule on these sectors.371 |
Scotland: an alternative strategy (zero Covid)
| 5.148. | In late June 2020, on a day when no deaths or new cases of Covid-19 were reported in Scotland for the most recent 24-hour period, Ms Sturgeon announced: “Suppressing the virus, driving it as far as we can towards total elimination has to be our overriding priority.“372 She predicted that Scotland was “not far away” from eliminating the virus.373 |
| 5.149. | During this period, the Scottish Government was considering an alternative strategy – one of ‘zero Covid’. Professor Stephen Reicher, Professor of Psychology at the University of St Andrews and participant in the Scientific Pandemic Insights Group on Behaviours (SPI-B), explained at the time:
“A Zero Covid strategy is based on a refusal to believe in any ‘acceptable’ level of Covid infections and deaths in the community and a relentless effort to drive it down.“374 |
| 5.150. | Ms Sturgeon told the Inquiry:
“I knew that our circumstances – particularly if the rest of the UK was not following suit – meant it was unlikely to be completely achievable for any sustained period of time. But by aiming to drive infection levels as close to zero as possible, it was likely that we would keep them lower than we would otherwise do.“375 She emphasised the importance of the distinction between the concepts of ‘elimination’ (which she equated with maximum suppression) and ‘eradication’ (which she understood to be an epidemiological concept that meant getting rid of the virus altogether – something that she understood was not achievable in the summer of 2020 in the absence of a vaccine).376 Others agreed that zero Covid was simply a way of expressing the aim of reducing transmission and, hence, suppressing the virus as much as possible.377 |
| 5.151. | Professor Mark Woolhouse, Professor of Infectious Disease Epidemiology at the University of Edinburgh and member of the Scottish Government Covid-19 Advisory Group, agreed. He told the Inquiry that the idea of eliminating the virus from Scotland in the summer of 2020 was also incompatible with the gradual relaxation of restrictions.378 He said that the Scottish Government was “flirting with a zero Covid strategy” over the summer of 2020, which showed that it “didn’t accept that the virus was here to stay“.379 Professor Woolhouse explained that the Scottish Government’s approach:
“signalled to me that the government did not accept the epidemiological assessment that there would be a second wave if too many restrictions were lifted, an assessment dating back to early March“.380 He was concerned that a second wave would occur once R rose above 1, regardless of the time it took to reach that point.381 In other words, “[a]ny threat to public health would come from unlocking too far not too fast“.382 |
| 5.152. | It was clear to Professor Thomas Evans, Professor of Molecular Microbiology at the University of Glasgow and member of the Scottish Government Covid-19 Advisory Group, that, by the summer of 2020:
“re-infection and thus waning immunity to infection was not uncommon. Unless strict lockdown remained in place, reintroduction and spread was always going to occur.“383 He therefore “never believed that a policy of zero COVID was likely [to] work“.384 |
| 5.153. | The Scottish Government considered its formal strategy in the summer of 2020 to be one of maximum suppression of the virus, rather than elimination. Zero Covid was described by the Scottish Government as its “stretch aim“.385 However, the language of ‘elimination’ was used by Ms Sturgeon, Jeane Freeman MSP (Cabinet Secretary for Health and Sport in the Scottish Government from June 2018 to May 2021) and Professor Smith in statements to both the Scottish Parliament and the media.386 |
| 5.154. | The idea of eliminating the virus from Scotland was inappropriate and destined to fail in the light of an open border with England and there being no agreement with the UK government to close it. The references by Ms Sturgeon and others to elimination of the virus from Scotland might have created the impression for the public that life could return to normal. This was described by Professor Sridhar as an “unintended consequence” of the Scottish Government’s messaging at that time.387 |
| 5.155. | It may also have had another unintended and unfortunate practical effect. Public Health Scotland suggested that the use of different language by the Scottish Government to express policy intent led to challenges in its development of guidance.388 |
Further easing of restrictions in July 2020
| 5.156. | On 2 July 2020, the UK government’s Covid-19 Dashboard recorded 89 daily deaths in the UK and 25,000 people estimated to be infected with the virus in England.389 R was estimated to be between 0.7 and 0.9 in England.390 |
| 5.157. | In England, Covid-S met on 2 July 2020 to consider winter preparedness. A Covid-19 Taskforce paper prepared for the meeting set out three scenarios of increasing severity to form the basis of the UK government’s winter planning:
|
| 5.158. | In July 2020, the UK government’s strategy for responding to Covid-19 began to shift towards local and more targeted measures. On 3 July, Mr Johnson announced publicly that the UK government intended to move away from “national lockdowns” to imposing targeted local lockdowns and local restrictions where necessary.392 Mr Johnson also gave instructions that the possibility of population segmentation should be explored.393 At the start of July, the use of “smart” interventions that sought to “maximise the impact on transmission while minimising the economic and/or social impact” was also considered.394 It is not clear to the Inquiry to what extent this work on ‘smarter’ interventions was ever seriously taken forward. |
| 5.159. | At a 10 Downing Street press conference in the late afternoon of 3 July 2020, Mr Johnson announced the latest figures for infections and deaths and gave details of which businesses would be allowed to reopen and of the social distancing restrictions that continued to apply.395 He stated that a timetable would be provided the following week for the reopening of other businesses, such as those in the arts and events industry, indoor gyms and nail bars.396 He warned, however, that “we are not out of the woods yet” and that targeted local lockdowns could be expected to be reimposed.397 Mr Johnson urged the British public to act safely.398 Mr Johnson further noted that the devolved administrations were going in the “same direction” as England, but perhaps at “slightly different speeds“.399 Professor Whitty warned that the virus was “not going to be gone for a very long time” and that, while Step 3 was “a reasonable package of measures“, it was not “risk-free“.400 |
| 5.160. | On 4 July 2020, Step 3 of the May 2020 Roadmap was implemented in England. This easing of restrictions constituted the reopening of many sectors of the economy and included the reduction to social distancing from two metres to one metre with mitigations. Restaurants, pubs, hairdressers and cinemas, among other outlets, were permitted to reopen in England, although people were urged to keep their distance from those outside their household and to try to stay two metres apart at all times. Some places remained shut, including nightclubs, bowling alleys, spas and swimming pools. In place of the previous restrictions on gatherings, gatherings of more than 30 people were banned.401 However, the UK government continued to advise that only up to six people (from no more than two households) should meet indoors or outdoors. On the same day, a local lockdown was imposed on Leicester.402 |
| 5.161. | Mr Johnson told the Inquiry that Step 3 was “a sensible and cautious approach to opening the economy and was predicated upon clear scientific, behavioural and economic advice“.403 He further claimed that “we were appropriately cautious in how we eased the first lockdown” and again that “[p]ublic health always remained my priority“.404 |
| 5.162. | Many of Mr Johnson’s advisers and ministers did not appear to agree with this characterisation. Scientific advisers had voiced concerns about the speed with which the first lockdown restrictions were eased, particularly in respect of Step 3 on 4 July 2020. Professors Whitty and Vallance had highlighted their concerns about Step 3 at Covid-S on 22 June 2020 and at a UK Cabinet meeting on 23 June. Professor Vallance had also advised decision-makers that, in making decisions about the timing of the easing of the lockdown, both R and overall prevalence were important considerations.405 This was because higher prevalence means that the easing of restrictions takes place in an environment where infections can grow more quickly. Test and trace was also likely to be overwhelmed where large numbers of people were passing on the virus to others. |
| 5.163. | Decision-makers and advisers in the UK government were aware of the risks inherent in Step 3.406 Both Mr Case and Mr Hancock had expressed concerns in mid-July 2020 about the speed with which restrictions were being eased.407 For example, on 13 July, Mr Hancock sent Mr Johnson a WhatsApp message stating: “I’m very worried about winter. We’ve gone fast on releasing lockdown.“408 Mr Case told the Inquiry that the failure of the UK government to adopt an incidence-based measure to guide its approach to unlocking led to a high-incidence environment in the autumn of 2020. This undermined the effectiveness of test and trace and restrictions at that time which aimed to avoid a second England-wide lockdown.409 |
| 5.164. | The easing of the majority of restrictions took place in England on 4 July 2020. The reality was that both Mr Johnson and Mr Sunak were in favour of restrictions being lifted as soon as possible in the summer of 2020, given what they saw as the imperative of restarting the economy, despite being informed by scientific advisers that this was an inherently high-risk approach. |
| 5.165. | Although the timing and scale of easing was a matter for politicians to decide, Mr Johnson was unwise to have run this risk. Despite his awareness of the clear risk of a second wave and his acknowledgement that another England-wide lockdown would be a disaster (as he told the UK Cabinet on 2 July 2020), he pushed ahead with reopening almost all sectors on 4 July.410 |
| 5.166. | The decision of the UK government to significantly ease restrictions in England on 4 July 2020, despite scientific advisers’ concerns about the public health risks of doing so, was high risk. It ran the risk that R would be pushed above 1 and that the effectiveness of test and trace and interventions to contain the subsequent spread of the virus would be fatally undermined. |
| 5.167. | Moreover, Mr Johnson was the Prime Minister of the whole of the UK. He should have considered the implications of his decision to ease restrictions significantly in England on the epidemiological positions and pandemic response in Scotland, Wales and Northern Ireland – given that there were open internal borders. There was nothing to prevent people resident in England from travelling across the porous internal borders of the UK. The high-risk approach adopted by the UK government to the easing of lockdown restrictions on 4 July 2020 risked undermining the effectiveness of the more cautious responses of the devolved administrations. Both Mr Drakeford and Ms Sturgeon subsequently wrote to Mr Johnson regarding travel across internal borders.411 |
| 5.168. | In contrast, the governments of Scotland, Wales and Northern Ireland adopted a cautious approach to the relaxation of restrictions throughout the summer of 2020. The Scottish Cabinet regularly discussed, such as on 14 April 2020 and 19 May 2020, that any relaxation of restrictions “should be introduced with great caution” and that a:
“careful, precautionary approach, which some might criticise as too slow, was necessary in order to ensure that the country did not slip back into a second wave of deadly infection“.412 |
| 5.169. | The Scottish Government implemented its first localised measures on 2 July 2020.413 This followed work undertaken to plan for localised measures, building on the publication of its Scotland’s Route Map Through and Out of the Crisis on 21 May 2020, which stated that the Scottish Government was keeping an “open mind on the potential for regional variation” in the phased approach to varying restrictions.414 |
| 5.170. | On 8 July 2020, the Scottish Cabinet observed that the “biggest threat to the Scottish Government’s ambition to eliminate the virus in Scotland was the importation of cases from other countries“.415 This had been the initial source of community transmission in early spring, when Scottish tourists had returned from mid-term breaks in Italy and Spain.416 On 9 July 2020, Ms Sturgeon announced the move to Phase 3 of Scotland’s Route Map Through and Out of the Crisis.417 This included changes to indoor and outdoor household gatherings from 10 July, the reopening of shops in shopping centres and dentists from 13 July and the reopening of hairdressers, pubs, restaurants, holiday accommodation, visitor attractions, cinemas and places of worship from 15 July, with some restrictions. |
| 5.171. | Mr Drakeford noted that, while there was a “shared direction of travel“, in his opinion the approach of the UK government “was to do so more swiftly and aggressively, and at the edge, rather than at the central thrust of scientific and medical opinion“.418 |
| 5.172. | Although the prospect of local restrictions was considered by the Covid-19 Core Group days earlier, the Welsh Government confirmed on 3 July 2020 the lifting of the Stay Local requirements from 6 July. It also confirmed that two households would be able to form a single, extended household for the purpose of the restrictions.419 The first day of no Covid-19-related deaths in Wales since 19 March 2020 occurred on 6 July. At the Welsh Cabinet review on 7 July 2020, “the situation was stable and improving with around seven to eight new cases a day being confirmed” and about 3,000 tests being carried out each day.420 In line with its published plans for easing restrictions, the Welsh Government continued to “follow a step by step, week by week approach“.421 However, by 10 July, Wales had experienced “recent increases linked to the two outbreaks at meat and food processing plants in Wrexham and Anglesey and an incident in Merthyr Tydfil“.422 The Welsh Government therefore considered that restrictions might need to be reimposed “in specific areas should the rate of transmission increase“.423 |
| 5.173. | Nonetheless, on 10 July, following its review of restrictions on 7 July, the Welsh Government indicated a number of changes, including the reopening of outdoor hospitality and indoor close-contact services from 13 July.424 It also outlined a number of further week-by-week relaxations. It confirmed that two-metre social distancing would remain in place but – for “exceptional” situations where it was “not always practical” – guidance for mitigations would be published.425 In reality, this was a similar step to that taken by the UK government in moving to Step 3 on 4 July and recognised that the distance of two metres was not viable for certain businesses. |
| 5.174. | Advice was also being developed to help inform the Welsh Government’s decision-making on the use of interventions.426 On 10 July 2020, the Technical Advisory Group produced a comprehensive list of triggers – “circuit breakers” and “early warning indicators“. These provided the Welsh Government with a list of indicators “designed to provide early warning of rising infection rates which in turn may mean that reverses in the lockdown measures need to be considered“.427 These were designed to help ministers decide “how and whether to reverse the easing of restrictions“.428 This was a helpful approach to monitoring the risks of Covid-19 in Wales and provided a signal as to whether further restrictions might need to be imposed. |
| 5.175. | By 2 July, Northern Ireland had experienced no Covid-19 deaths for 15 days, had no Covid-19 patients in intensive care units and had reduced numbers of cases in hospitals.429 On 6 July 2020, the Northern Ireland Executive agreed that indoor marriage ceremonies and baptisms could resume from 10 July, with venues and places of worship to determine numbers attending on a risk-assessed basis.430 The use of face coverings became mandatory on public transport from 10 July in Northern Ireland.431 |
| 5.176. | From an early stage, the Northern Ireland Executive had been advised of the likelihood of a second wave of Covid-19 infections in the autumn of 2020 and that the relaxation of restrictions would lead to an increase in the rate of transmission. Its approach to the relaxation of restrictions centred on five guiding principles: (i) controlling transmission (maintaining R below 1); (ii) protecting healthcare capacity; (iii) necessity; (iv) proportionality; and (iv) reliance on evidence in making any changes to existing restrictions. The Executive Committee did not seek to prescribe dates for the relaxation of specific restrictions. Instead, it adopted an approach of making decisions on the basis of these five principles. This cautious approach to the potential relaxation of non-pharmaceutical interventions was an appropriate one, given the picture of transmission in Northern Ireland at the time. |
The divergence of approaches across the UK
| 5.177. | Although a strong four-nations approach had been taken when entering into the first UK-wide lockdown, similar efforts were not made to discuss strategies on the exit from that lockdown. This resulted in the first signs of divergence of the UK-wide approach to the pandemic response in May 2020. The UK government’s desire to return to normality faster contrasted with the more cautious approaches of the governments of Scotland, Wales and Northern Ireland. |
| 5.178. | The Inquiry understands the need to balance the wide range of harms caused by stringent restrictions and the harms caused by the virus. However, the pace at which the UK government eased the first lockdown restrictions – particularly in respect of Step 3 on 4 July 2020 – was not without risk. It created the prospect of more stringent restrictions or a second lockdown becoming necessary later in the year. In contrast, the more gradual easing of restrictions in Scotland, Wales and Northern Ireland, against a background of a positive epidemiological position in the early summer of 2020, at least created a greater prospect of further lockdowns not being necessary or, if they were, not being necessary for so long. |
| 5.179. | However, despite the diverging approaches to the easing of restrictions, all four nations were hit by a second wave and were forced ultimately, albeit at different times, into further nationwide or (in Scotland’s case) regional lockdowns. |
- INQ000088326_0001
- ‘Coronavirus (COVID-19) update: First Minister’s speech 2 April 2020’, Scottish Government, 2 April 2020 (https://www.gov.scot/publications/first-minister-covid-19-update-10; INQ000354191)
- INQ000321135_0001
- INQ000430391_Tab 1
- See UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download).
- INQ000232194_0078 para 326; INQ000233779. Nightingale hospitals are temporary medical facilities set up during a crisis.
- INQ000056105_0001-0002
- ‘Temporary COVID-19 medical facility’, Scottish Government, 30 March 2020 (https://www.gov.scot/news/temporary-covid-19-medical-facility; INQ000587949). The hospital became operational on 19 April 2020.
- INQ000113672
- INQ000411550_0107-0108 paras 323-324
- ‘Health and Social Care Secretary’s statement on coronavirus (COVID-19): 2 April 2020’, Department of Health and Social Care, 2 April 2020 (https://www.gov.uk/government/speeches/health-and-social-care-secretarys-statement-on-coronavirus-covid-19-2-april-2020;
INQ000086583); ‘Health Secretary sets out plan to carry out 100,000 coronavirus tests a day’, Department of Health and Social Care, 2 April 2020 (https://www.gov.uk/government/news/health-secretary-sets-out-plan-to-carry-out-100000-coronavirus-tests-a-day; INQ000237310) - INQ000232194_0080 para 334
- INQ000088606_0004
- ‘Coronavirus (COVID-19) update: First Minister’s speech 3 April 2020’, Scottish Government, 3 April 2020 (https://www.gov.scot/publications/first-minister-covid-19-update-9; INQ000354245)
- INQ000391237_0122-0123 para 469
- INQ000103649_0011-0012 paras 2.7, 3.3
- ‘Prime Minister’s statement on coronavirus (COVID-19): 23 March 2020’, Prime Minister’s Office and Boris Johnson, 23 March 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-23-march-2020; INQ000086759)
- In England, regulations were initially required to be reviewed every 21 days, increasing to every 28 days from June 2020 (The Health Protection (Coronavirus, Restrictions) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/350/2020-03-26;
INQ000391420_0002 para 3(2)); The Health Protection (Coronavirus, Restrictions) (England) (No. 3) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/750/made; INQ000348053_0002 para 2(2))). - INQ000056136_0001-0003
- INQ000056136_0004
- INQ000146695
- INQ000197998; INQ000252914_0008 para 16
- INQ000197998
- INQ000061722
- INQ000056136_0008; INQ000146695
- INQ000146695_0005
- INQ000146695_0005
- INQ000056136
- INQ000061527
- INQ000061528
- INQ000212100; INQ000212094
- INQ000309529_0039-0040 para 131
- INQ000130409
- INQ000065748; INQ000048450_0002 para 5. This was commissioned in mid-March 2020 (INQ000309139).
- INQ000449440_0066 para 192
- INQ000259487; INQ000438173_0006 para 21
- INQ000214646_0003 para 12(b)
- INQ000214646_0003 para 12(b)
- INQ000233346_0001
- INQ000233346_0002
- INQ000256826_0001
- INQ000256826_0001
- INQ000256826_0002
- Nicola Sturgeon 31 January 2024 119/2-121/1; INQ000273978_0005 para 24
- INQ000148847
- INQ000148847_0003-0004; see also INQ000238826_010 -0105 para 317
- INQ000238826_0104-0105 para 317; INQ000148847
- INQ000182368_0001 para 1
- INQ000182368_0003 para 9
- INQ000182368_0004 para 15
- INQ000182368_0005 paras 16, 17
- INQ000255836_0092 para 345
- INQ000255836_0092 para 345
- INQ000233375_0006
- INQ000220042; ‘Statement from Downing Street: 6 April 2020’, Prime Minister’s Office, 6 April 2020 (https://www.gov.uk/government/news/statement-from-downing-street-6-april-2020; INQ000182383)
- INQ000220042_0001
- INQ000220042_0001
- INQ000061531
- INQ000120504_0002 paras 12, 13
- INQ000268041_0040-0041 para 132; INQ000083830_0001
- INQ000273747_0023-0024 para 73
- INQ000061811
- INQ000256839_0001; INQ000256829
- INQ000083787_0002
- INQ000083830_0004
- INQ000220051
- INQ000220051
- INQ000220051
- INQ000309529_0039-0040 para 131; INQ000216188
- INQ000216188
- INQ000216188; INQ000309529_0040 para 132
- INQ000061533_0004 para 15
- INQ000061533_0004 paras 16, 18
- INQ000198990; INQ000259848_0034 para 56
- INQ000217506_0001; INQ000217503
- ‘Coronavirus (COVID-19) update: First Minister’s speech 16 April 2020’, Scottish Government, 16 April 2020 (https://www.gov.scot/publications/first-minister-covid-19-update-17; INQ000357360)
- INQ000214644_0002 para 6
- INQ000352514; INQ000217505
- INQ000352514_0005 para 28
- INQ000352514_0005 para 30
- INQ000220052_0001 paras 1, 2; see also INQ000220054; INQ000109278
- INQ000195907; INQ000220057
- INQ000089020_0009
- INQ000048455
- INQ000065643_0003 para 10
- INQ000048455
- INQ000349314_0002 para 9
- INQ000349314_0003 para 13
- INQ000145553
- INQ000389184_0040-0041 paras 138-140; INQ000023238; INQ000361513
- INQ000083827_0006,0008-0009
- ‘Foreign Secretary’s statement on coronavirus (COVID-19): 16 April 2020’, Foreign and Commonwealth Office, Prime Minister’s Office and Dominic Raab, 16 April 2020 (https://www.gov.uk/government/speeches/foreign-secretarys-statement-on-coronavirus-covid-19-16-april-2020; INQ000086576_0004)
- INQ000238826_0105-0106 para 321
- INQ000651575_0001
- INQ000183916_0001; INQ000255836_0081 para 305; INQ000411550_0112 para 341
- INQ000216598_0001
- INQ000232194_0086 para 356; see also INQ000182367_0001 para 2
- ‘Olympics chief brought in to boost PPE production’, Department of Health and Social Care and Matt Hancock, 19 April 2020 (https://www.gov.uk/government/news/olympics-chief-brought-in-to-boost-ppe-production; INQ000198247); INQ000232194_0086 para 357
- INQ000075780_0002-0003 paras 2, 23
- INQ000075780_0003 para 24
- INQ000102697_0033
- INQ000216489_0001
- INQ000216489_0001
- INQ000061535_0004 paras 12, 14
- INQ000061535_0004 para 11
- INQ000182349; INQ000182350; INQ000182351
- INQ000048313_0018 para 3
- INQ000048313_0018 para 3
- INQ000182353
- INQ000182367_0001 para 1
- INQ000249543
- INQ000250229_0033 para 124; INQ000182367
- INQ000182367_0002 para 6
- INQ000182367_0002 para 8
- INQ000182367_0002 para 5
- INQ000182367_0002 para 5
- ‘Coronavirus testing extended to all essential workers in England who have symptoms’, Department of Health and Social Care, 23 April 2020 (https://www.gov.uk/government/news/coronavirus-testing-extended-to-all-essential-workers-in-england-who-havesymptoms; INQ000497452)
- COVID-19 – A Framework for Decision Making, Scottish Government, 23 April 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making; INQ000369689)
- COVID-19 – A Framework for Decision Making, Scottish Government, 23 April 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making; INQ000369689)
- ‘Lifting of Scottish coronavirus lockdown “likely to be phased”’, BBC News, 23 April 2020 (https://www.bbc.co.uk/news/uk-scotland-52394685; INQ000357796); ‘Looking beyond lockdown’, Scottish Government, 23 April 2020 (https://www.gov.scot/news/looking-beyond-lockdown; INQ000369715)
- Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery, Welsh Government, April 2020 (https://www.gov.wales/sites/default/files/publications/2020-04/leading-wales-out-of-the-coronavirus-pandemic.pdf; INQ000349353)
- INQ000215197; INQ000215196
- INQ000371209_0047-0048 para 154
- Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery, Welsh Government, April 2020, p7 (https://www.gov.wales/sites/default/files/publications/2020-04/leading-wales-out-of-the-coronavirus-pandemic.pdf; INQ000349353)
- INQ000065751_0016-0021; INQ000048459
- INQ000317372_0001
- Ian Young 7 May 2024 132/11-133/20; INQ000409589_0016-0017 para 47
- INQ000232549_0002
- INQ000232549_0002
- INQ000232549_0002 para 2
- INQ000214575_0003 para 10
- INQ000391237_0122-0123 para 469
- INQ000222807_0001
- INQ000283921_0005
- INQ000088694_0007
- INQ000309529_0040 para 135; INQ000061546_0002, 0003, 0006 paras 3, 21, 31
- INQ000309529_0041 para 136
- Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery, Welsh Government, April 2020 (https://www.gov.wales/sites/default/files/publications/2020-04/leading-wales-out-of-the-coronavirus-pandemic.pdf; INQ000349353); INQ000256845_0001; see also INQ000255836_0092,0097 paras 345, 362
- Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery, Welsh Government, April 2020, p3 (https://www.gov.wales/sites/default/files/publications/2020-04/leading-wales-out-of-the-coronavirus-pandemic.pdf; INQ000349353)
- ‘Coronavirus: Boris Johnson says UK is past the peak of outbreak’, BBC News, 30 April 2020 (https://www.bbc.co.uk/news/uk-52493500; INQ000573837)
- INQ000273747_0026-0027 para 82
- INQ000151558_0003
- INQ000236391_0002 para 24; INQ000048399_0003
- INQ000120503_0002 para 4
- INQ000233375_0006
- INQ000214644_0003 para 7(a)
- INQ000299989_0003
- Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery, Welsh Government, April 2020, p2 (https://www.gov.wales/sites/default/files/publications/2020-04/leading-wales-out-of-the-coronavirus-pandemic.pdf; INQ000349353)
- INQ000065751_0005-0009
- INQ000137369; Ian Young 7 May 2024 160/15-23
- INQ000065643_0003 para 12
- INQ000065751_0009
- INQ000195909; INQ000238826_0018 para 45b. For the first three months, the survey was piloted in England only. Wales was the first of the devolved nations to join the survey, in late June 2020 (Ian Diamond 29 February 2024 67/23-68/20, 69/17-70/3). Northern Ireland joined in July 2020 and Scotland in September 2020 (INQ000268012_0018 para 82).
- INQ000396876_0025 para 75
- INQ000269182_0047 para 174; see also INQ000147810_0029-0030 para 90.
- Technical Report on the COVID-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, p126, p159 point 4 (https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642)
- The critical role of surveillance studies, including the Coronavirus (Covid-19) Infection Survey and REACT, was emphasised in the Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, p87 (https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642).
- INQ000232194_0091 para 377; Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, pp321-322 (https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642)
- INQ000088527_0001-0002 paras 5, 7
- INQ000183928; INQ000183927; INQ000255836_0101-0102 paras 377, 378
- Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892); ‘Prime Minister’s statement on coronavirus (COVID-19): 10 May 2020’, Prime Minister’s Office and Boris Johnson, 10 May 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-10-may-2020; INQ000065338)
- INQ000183927_0008-0009
- INQ000255836_0102-0103 para 380; INQ000183926; INQ000302484_0026 para 96
- INQ000236585_0001
- INQ000236585_0001-0002
- INQ000061541_0004 para 21
- INQ000061541_0004 para 22
- INQ000061541_0004 para 23
- INQ000061542_0002 para 5
- INQ000214723_0003 para 11(a)
- INQ000214723_0002 para 4
- INQ000214723_0002 para 4
- INQ000214723_0003 para 10
- INQ000214723_0003 para 10
- INQ000065566_0006 para 16
- INQ000289218
- INQ000065566_0006 para 16
- INQ000065566_0008 para 27
- INQ000065724_0006
- INQ000048464_0005 para 13
- INQ000048464_0003 para 8
- INQ000048465_0003-0004 paras 9-10
- INQ000048792_0002 para 1.6
- INQ000048792_0002 para 1.7
- INQ000048792_0005 para 1.29
- INQ000090560_0002
- INQ000249584
- INQ000249584
- INQ000183933_0004-0008; INQ000185094
- INQ000232194_0095 para 391; INQ000250229_0034 para 130; INQ000268041_0047 para 149
- INQ000083828_0001-0003
- INQ000083782
- INQ000256846
- INQ000083828_0005–0006 para 6
- INQ000083828_0007
- INQ000083828_0007
- Gavin Freeguard 10 October 2023 177/16-22
- INQ000238826_0020 para 48
- INQ000147810_0029-0030 para 90
- INQ000083828_0006 para 7
- INQ000088983_0002
- ‘First Minister of Wales’ message to the people of Wales’, Welsh Government, 10 May 2020 (https://www.gov.wales/first-minister-wales-message-people-wales; INQ000090561); INQ000083136_0002
- Mark Drakeford 13 March 2024 110/8-111/23; see also INQ000273747_0030 para 94; INQ000216537
- INQ000083136_0002; INQ000255838_0030 para 110
- INQ000273783_0031 para 159
- INQ000339033_0027 para 63
- ‘Nicola Sturgeon leads chorus of disapproval over Johnson’s “stay alert” message’, The Guardian, 10 May 2020 (https://www.theguardian.com/world/2020/may/10/nicola-sturgeon-leads-criticism-of-uks-new-stay-alert-coronavirus-lockdown-advice; INQ000351048)
- INQ000339033_002 para 64
- INQ000339033_0027-0028 paras 63, 64
- INQ000371583_0018-0019 para 58
- INQ000371583_0018-0019 para 59
- Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892); ‘Prime Minister’s statement on coronavirus (COVID-19): 10 May 2020’, Prime Minister’s Office and Boris Johnson, 10 May 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-10-may-2020; INQ000065338)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 10 May 2020’, Prime Minister’s Office and Boris Johnson, 10 May 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-10-may-2020; INQ000065338_0004)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 10 May 2020’, Prime Minister’s Office and Boris Johnson, 10 May 2020 (https://www.gov.uk/government/speeches/pm-address-to-the-nation-on-coronavirus-10-may-2020; INQ000065338_0007)
- INQ000273901_0047. Professor Vallance recorded his personal views in his ‘evening notes’ on an almost daily basis during the pandemic response. These were private notes kept by him during a period of “enormous stress” in which he reflected on the day’s events as a “day-by-day release valve” (INQ000238826_0157-0159, paras 471-480).
- There was never in fact any legal limit on the number of times outdoor exercise could be taken in England as there had been in Wales – see Regulation 8 of The Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/353/contents)
and Regulation 6 of The Health Protection (Coronavirus, Restrictions) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/350/contents). - Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020, p27 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892)
- Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020, p27 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892)
- Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892)
- INQ000273841_0065-0066 para 131
- INQ000308305_0001
- Mark Sedwill 8 November 2023 97/3-98/7
- INQ000302484_0026 paras 96, 97
- INQ000273841_0065 para 130
- Regulation 2 of The Health Protection (Coronavirus, Restrictions) (England) (Amendment) (No. 2) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/500/contents/made)
- Unlocking Our Society and Economy: Continuing the Conversation, Welsh Government, 15 May 2020 (https://www.gov.wales/sites/default/files/publications/2020-05/unlocking-our-society-and-economy-continuing-the-conversation.pdf; INQ000320855)
- Leading Wales out of the Coronavirus Pandemic: A Framework for Recovery, Welsh Government, April 2020 (https://www.gov.wales/sites/default/files/publications/2020-04/leading-wales-out-of-the-coronavirus-pandemic.pdf; INQ000349353)
- Unlocking Our Society and Economy: Continuing the Conversation, Welsh Government, 15 May 2020 (https://www.gov.wales/sites/default/files/publications/2020-05/unlocking-our-society-and-economy-continuing-the-conversation.pdf; INQ000320855_0003)
- Unlocking Our Society and Economy: Continuing the Conversation, Welsh Government, 15 May 2020 (https://www.gov.wales/sites/default/files/publications/2020-05/unlocking-our-society-and-economy-continuing-the-conversation.pdf; INQ000320855_0003)
- Coronavirus: Executive Approach to Decision-Making, Northern Ireland Executive, May 2020 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/execuitveour-approach-to-decision-making.pdf; INQ000137371)
- INQ000421704_0164 para 361
- Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072)
- Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072)
- ‘Everyone in the United Kingdom with symptoms now eligible for coronavirus tests’, Department of Health and Social Care, 18 May 2020 (https://www.gov.uk/government/news/everyone-in-the-united-kingdom-with-symptoms-now-eligible-for-coronavirus-tests; INQ000497453)
- INQ000061546_0002 para 3
- INQ000283895_0015
- INQ000061546_0002-0003 para 21
- INQ000061546_0003 para 21
- INQ000061546_0002 para 13
- INQ000061546_0002 para 13
- INQ000088056
- INQ000089051_0009
- INQ000273901_0062
- INQ000185076
- INQ000089074_0009
- INQ000273901_0066
- ‘Coronavirus: I don’t regret what I did, says Dominic Cummings’, BBC News, 25 May 2020 (https://www.bbc.co.uk/news/uk-politics-52800595; INQ000651561)
- INQ000137216
- INQ000183937_0008; INQ000255836_0106 para 395
- INQ000183936; INQ000255836_0106 para 395
- ‘Prime Minister’s statement on coronavirus (COVID-19): 28 May 2020’, Prime Minister’s Office and Boris Johnson, 28 May 2020 (https://www.gov.uk/government/speeches/pm-press-conference-statement-on-the-five-tests-28-may-2020;
INQ000065357); INQ000255836_0106-0107 para 396 - Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072); ‘Coronavirus (COVID-19) update: First Minister’s speech 28 May 2020’, Scottish Government, 28 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-28-2020; INQ000369675)
- INQ000090566_0001
- INQ000048926_0002-0003 paras 1.4-1.5, 1.9-1.10; Jeremy
Miles 12 March 2024 179/2-15; INQ000090566 - INQ000065586_0010-0011 para 42
- INQ000065586_0014 para 61
- INQ000048469_0003 para 8
- INQ000065718_0002
- INQ000065718_0002
- INQ000048471_0002 para 5
- INQ000255317; INQ000417311
- INQ000272088_0004; INQ000279225; INQ000449440_0110 para 304
- INQ000438171_0019 para 83; INQ000449440_0110 para 304
- INQ000430391_Tab 1
- INQ000255836_0211 para 719(d)
- INQ000092893_0006 para 1.24
- INQ000087165
- INQ000183934_0005; INQ000250229_0035-0036 para 134; INQ000255836_0108 para 401
- INQ000183934_0006
- INQ000259848_0009 para 16(f)(ii)
- INQ000183934_0002
- INQ000183934_0003 para 6; see also INQ000255836_0098-0099 paras 367, 368
- INQ000273841_0073 para 148; INQ000092893_0040
para 5.53; Simon Ridley 7 November 2023 39/15-19 - INQ000207294_0002-0003,0019-0021 paras 1.5, 3.19; INQ000092893_0040 para 5.53
- INQ000136763_0005 para 9; INQ000273841_0073 para 148; INQ000207294_0015-0016 paras 3.8.2, 3.11; Simon Ridley 7 November 2023 38/3-17; INQ000252914_0094 para 408; INQ000092893_0040 para 5.53; INQ000281724; INQ000302484_0034 para 130; INQ000092893_0040 para 5.54; Rishi Sunak 11 December 2023 19/22-20/5; INQ000248852_0002-0003 para 1.7
- INQ000255836_0214-0215 paras 721(f), 721(g); Simon Ridley 7 November 2023 40/15-20
- The Health Protection (Coronavirus, Restrictions) (England) (Amendment) (No. 3) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/558/contents/made)
- INQ000389184_0058-0059 para 201
- INQ000065816_0002
- INQ000088938_0009
- INQ000088938_0009
- INQ000255836_0107 para 398
- INQ000237819_0021 para 48; INQ000273872_0107 para 536
- ‘“Check in, catch up, prepare for summer and September” – all schools in Wales to enter next phase’, Welsh Government, 3 June 2020 (https://www.gov.wales/check-catch-prepare-summer-and-september-all-schools-wales-enter-next-phase; INQ000300048_0001)
- INQ000120526_0003 para 33
- INQ000120526_0004 paras 34-35
- INQ000088234_0007-0008
- INQ000088059. In May 2020, Mr Sunak had encouraged the opening of all non-essential retail from 1 June as part of Step 2 of the May 2020 Roadmap, rather than a phased approach (INQ000088054; INQ000232085_0002 para 13).
- INQ000233834_0002 para 6
- INQ000233834_0006 para 23
- INQ000088241
- ‘Advice on the use of masks in the context of Covid-19’, World Health Organization, 5 June 2020 (https://iris.who.int/handle/10665/332293; INQ000229307)
- ‘Advice on the use of masks in the context of Covid-19’, World Health Organization, 5 June 2020 (https://iris.who.int/handle/10665/332293; INQ000229307_0006)
- INQ000281742_0002-0003
- INQ000311901
- ‘3 layer face coverings recommended, but not mandatory, in certain situations in Wales’, Welsh Government, 9 June 2020 (https://www.gov.wales/3-layer-face-coverings-recommended-not-mandatory-certain-situations-wales; INQ000350831)
- ‘Scotland reports no new virus deaths for first time since lockdown as UK reports lowest number of fatalities since March’, ITV News, 7 June 2020 (https://www.itv.com/news/2020-06-07/scotland-reports-no-new-coronavirus-deaths-for-first-time-since-lockdown; INQ000357844); INQ000048472_0002 para 4
- INQ000283697_0001
- ‘Written Statement: The Health Protection (Coronavirus, International Travel) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 5 June 2020 (https://www.gov.wales/written-statement-health-protection-coronavirus-international-travel-wales-regulations-2020; INQ000023244); The Health Protection (Coronavirus, International Travel) England Regulations 2020 (Regulations applying in England)(https://www.legislation.gov.uk/uksi/2020/568/contents/made; The Health Protection (Coronavirus, International Travel) (Wales) Regulations 2020 (Regulations applying in Wales) (https://www.legislation.gov.uk/wsi/2020/574/introduction/made); The Health Protection (Coronavirus, International Travel) Regulations (Northern Ireland) 2020 (Regulations applying in Northern Ireland (https://www.legislation.gov.uk/nisr/2020/90/part/2/2020-06-08); The Health Protection (Coronavirus) (International Travel) (Scotland) Regulation 2020 (Regulations applying in
Scotland) (https://www.legislation.gov.uk/ssi/2020/169/made) - INQ000050763
- INQ000088978_0005
- ‘Prime Minister’s statement on coronavirus (COVID-19): 10 June 2020’, Prime Minister’s Office and Boris Johnson, 10 June 2020 (https://www.gov.uk/government/speeches/pm-statement-at-the-coronavirus-press-conference-10-june-2020; INQ000075728)
- INQ000065729_0003
- INQ000048473_0002 para 6
- INQ000207249
- INQ000207249_0001-0002 paras 5, 6
- INQ000207249_0002 paras 6, 7
- INQ000048474_0004 para 15
- INQ000065730_0008
- See Regulation 1(3) of The Health Protection (Coronavirus, Restrictions) (England) (Amendment) (No. 4) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/588/contents/made.
- The Health Protection (Coronavirus, Wearing of Face Coverings on Public Transport) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/592/contents/made)
- INQ000217684
- INQ000217685_0003
- INQ000236653_0010. A key message contained in the note was the view that “Scotland is now in a strong position to eliminate the Covid-19 virus.” Though the paper predicted that further cases would probably be imported, it also said that “if these are identified quickly, traced and all exposed isolated” the elimination strategy could “facilitate a return to a largely ‘normal’ daily life for most”.
- INQ000236653_0008
- INQ000236653_0007; INQ000398982_0013
- ‘Scotland “not far away” from eliminating coronavirus’, BBC News, 26 June 2020 (https://www.bbc.co.uk/news/uk-scotland-53195166; INQ000357836); Jason Leitch 23 January 2024 158/21-159/24
- INQ000048799_0002 para 1.4
- INQ000048799_0003 para 1.9
- ‘Written Statement: Review of Lockdown Measures and The Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 19 June 2020 (https://www.gov.wales/written-statement-review-lockdown-measures-and-health-protection-coronavirus-restrictions-wales-0; INQ000023247_0003)
- ‘Written Statement: Review of Lockdown Measures and The Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 19 June 2020 (https://www.gov.wales/written-statement-review-lockdown-measures-and-health-protection-coronavirus-restrictions-wales-0; INQ000023247)
- Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072); INQ000354125
- INQ000065611_0005 para 27
- INQ000065611_0005 para 28; INQ000061550_0002 para 6
- INQ000065611_0009-0010 paras 46, 47
- INQ000065773_0005
- INQ000065773_0004
- INQ000048475_0003
- INQ000065774_0001
- INQ000279355
- INQ000174752
- INQ000174752_0001
- INQ000088242
- INQ000069760
- INQ000088242_0004
- INQ000088242_0004
- INQ000062348
- INQ000088242_0006-0007
- INQ000088239_0003 para 5
- INQ000089071_0007-0009
- ‘Prime Minister’s statement to the House on COVID-19: 23 June 2020’, Prime Minister’s Office and Boris Johnson, 23 June 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-to-the-house-on-covid-19-23-june-2020; INQ000106501_0005); INQ000255836_0115-0116 para 421
- The Health Protection (Coronavirus, Wearing of Face Coverings on Public Transport) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/592/contents/made); ‘Face coverings mandatory on public transport from 22 June’, Scottish Government, 18 June 2020 (https://www.gov.scot/news/face-coverings-mandatory-on-public-transport-from-22-june; INQ000651562)
- INQ000184573_0002
- INQ000184573_0002
- INQ000218325
- INQ000120526_0003 para 33
- INQ000235261_0001
- INQ000283296_0002
- INQ000283296_0002
- INQ000088059; INQ000184573_0002
- Simon Case 23 May 2024 106/7-14
- Simon Case 23 May 2024 110/5-7
- INQ000273901_0094
- INQ000120526_0003 para 33
- ‘Review of two metre social distancing guidance’, Cabinet Office, 26 June 2020 (https://www.gov.uk/government/publications/review-of-two-metre-social-distancing-guidance/review-of-two-metre-social-distancing-guidance; INQ000181693_0007 para 5)
- INQ000181693_0007 para 2
- INQ000255836_0114 para 418
- INQ000255836_0114 para 419
- INQ000238826_0111-0112 para 338
- INQ000251645_0171 para 8.135
- INQ000269203_0099 para 7.22
- INQ000065730
- INQ000065730_0011
- INQ000216523_0003; INQ000273747_0034 para 109; Mark
Drakeford 13 March 2024 131/24-133/10 - INQ000371209_0067 para 213
- INQ000371209_0067 para 213
- INQ000362880_0005 para 27(a); INQ000214502_0003 para 12
- INQ000218300; INQ000218299
- COVID-19 – A Framework for Decision Making, Scottish Government, 23 April 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making; INQ000369689); INQ000214408_0003 para 13
- Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072); ‘Coronavirus (COVID-19) update: First Minister’s speech 2 July 2020’, Scottish Government, 2 July 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-2-july-2020; INQ000354193)
- ‘Coronavirus (COVID-19) update: First Minister’s speech 2 July 2020’, Scottish Government, 2 July 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-2-july-2020; INQ000354193)
- ‘Coronavirus (COVID-19) update: First Minister’s speech 26 June 2020’, Scottish Government, 26 June 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-26-june-2020; INQ000235122_0005)
- ‘Why Scotland’s Zero-Covid strategy is the best way forward’, The National, 1 August 2020 (https://www.thenational.scot/news/18622350.scotlands-zero-covid-strategy-best-way-forward; INQ000326388_0002); see also Covid-19: Examining the Effectiveness of Non-pharmaceutical Interventions, The Royal Society, August 2023, p19 (https://royalsociety.org/-/media/policy/projects/impact-non-pharmaceutical-interventions-on-covid-19-transmission/the-royal-society-covid-19-examining-the-effectiveness-of-non-pharmaceutical-interventions-report.pdf;
INQ000250983) - INQ000339033_0105-0106 para 289
- Nicola Sturgeon 31 January 2024 186/16-196/2
- INQ000339039_0006-0007 paras 22, 27; INQ000339033_0105-0106 para 289; INQ000273978_0025
para 108; Gregor Smith 22 January 2024 178/14-20 - INQ000250231_0035 para 194
- Mark Woolhouse 24 January 2024 59/22-25
- INQ000250231_0035 para 195
- INQ000250231_0035 para 196
- INQ000250231_0035 para 196
- INQ000346147_0012 para 33
- INQ000346147_0012 para 33
- INQ000339039_0007 para 27; COVID-19 – A Framework for Decision Making, Scottish Government, 23 April 2020, p6 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making; INQ000369689); Gregor Smith 22 January 2024 178/14-18; ‘Coronavirus (COVID-19) update: First Minister’s speech 26 June 2020’, Scottish Government, 26 June 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-26-june-2020; INQ000235122_0005)
- INQ000237820_0031 para 4.2.7; ‘Scotland “not far away” from eliminating coronavirus’, BBC News, 26 June 2020 (https://www.bbc.co.uk/news/uk-scotland-53195166; INQ000357836_0001)
- Devi Sridhar 23 January 2024 158/21-159/24; see also INQ000370347_0039 para 80
- INQ000237820_0031 para 4.2.8
- INQ000183952_0001
- INQ000255836_0117 para 425
- INQ000088245; INQ000088301_0013 para 27
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 July 2020’, Prime Minister’s Office and Boris Johnson, 3 July 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-3-july-2020; INQ000065412_0003)
- INQ000088251_0005-0006
- INQ000198120_0002; INQ000062371
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 July 2020’, Prime Minister’s Office and Boris Johnson, 3 July 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-3-july-2020; INQ000065412)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 July 2020’, Prime Minister’s Office and Boris Johnson, 3 July 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-3-july-2020; INQ000065412_0003)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 July 2020’, Prime Minister’s Office and Boris Johnson, 3 July 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-3-july-2020; INQ000065412_0005)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 3 July 2020’, Prime Minister’s Office and Boris Johnson, 3 July 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-3-july-2020; INQ000065412_0005)
- INQ000064552_0002
- INQ000064552_0002
- The Health Protection (Coronavirus, Restrictions) (No. 2) (England) Regulations 2020, regulation 5(1) (https://www.legislation.gov.uk/uksi/2020/684/regulation/5/made)
- The Health Protection (Coronavirus, Restrictions) (Leicester) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/685/contents/made)
- INQ000255836_0112 para 413
- INQ000255836_0125 para 447
- INQ000238826_0107 para 325
- INQ000207294_0024 para 3.26; INQ000232194_0102-0103,
0105 paras 419, 426; Rishi Sunak 11 December 2023 101/25-102/6 - INQ000048313_0052; INQ000129422
- INQ000129422
- Simon Case 23 May 2024 134/20-137/23
- INQ000088245_0007
- INQ000198495; INQ000256868
- INQ000214644_0003 para 7(a); INQ000214402_0010 para 41(i)
- ‘Coronavirus (COVID-19): Dumfries and Galloway’, Scottish Government, 2 July 2020 (https://www.gov.scot/news/management-of-local-covid-19-outbreak; INQ000651560)
- Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072); INQ000256709_0019
- INQ000214409_0003 para 11
- INQ000214409_0003 para 11
- Scotland’s Route Map Through and Out of the Crisis, Scottish Government, 21 May 2020 (https://www.gov.scot/publications/coronavirus-covid-19-framework-decision-making-scotlands-route-map-through-out-crisis; INQ000131072); INQ000189592
- INQ000371209_0067 para 213
- INQ000349671_0002 para 7; ‘Written Statement: Review of Lockdown Measures and The Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 3 July 2020 (https://www.gov.wales/written-statement-review-lockdown-measures-and-health-protection-coronavirus-restrictions-wales; INQ000023250); ‘Written Statement: Review of Lockdown Measures and The Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 19 June 2020 (https://www.gov.wales/written-statement-reviewlockdown-measures-and-health-protection-coronavirus-restrictions-wales-0; INQ000023247_0003); INQ000048799_0004 para 1.19
- INQ000022489_0002 para 1.4
- INQ000048852_0003 para 2.2
- ‘Written Statement: Review of the Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 10 July 2020 (https://www.gov.wales/written-statement-review-health-protection-coronavirus-restrictions-wales-regulations-2020; INQ000023251)
- INQ000048852_0002 para 1.6
- ‘Written Statement: Review of the Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 10 July 2020 (https://www.gov.wales/written-statement-review-health-protection-coronavirus-restrictions-wales-regulations-2020; INQ000023251); INQ000048852
- ‘Written Statement: Review of the Health Protection (Coronavirus Restrictions) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 10 July 2020 (https://www.gov.wales/written-statement-review-health-protection-coronavirus-restrictions-wales-regulations-2020; INQ000023251_0004); INQ000320905
- INQ000048829_0011-0012 paras 46-50; ‘Chief Medical Officer statement on 21 day review: 28 May 2020’, Welsh Government, 2 June 2020 (https://www.gov.wales/chief-medical-officer-statement-21-day-review-28-may-2020; INQ000048740_0002); INQ000048799_0002 para 1.6
- Technical Advisory Cell: Circuit Breakers/Early Warning Indicators, Welsh Government, 10 July 2020 (https://www.gov.wales/sites/default/files/publications/2020-07/technical-advisory-cell-circuit-breakers-early-warning-indicators.pdf; INQ000227967_0002). The application of what the Welsh Government called ‘circuit breakers’ required the monitoring of different categories, such as hospital capacity, which, if the data hit a certain threshold, established a trigger point at which further restrictions might be necessary (this use differed from that of the UK government and the other devolved administrations, which used the term circuit breakers to refer to the restrictions themselves). ‘Early warning indicators’ covered a wider range of measures for monitoring prevalence and the impact of the virus and sought to provide evidence of when a circuit breaker might be close to being triggered.
- Technical Advisory Cell: Circuit Breakers/Early Warning Indicators, Welsh Government, 10 July 2020 (https://www.gov.wales/sites/default/files/publications/2020-07/technical-advisory-cell-circuit-breakers-early-warning-indicators.pdf; INQ000227967_0002)
- INQ000048479_0002 para 2
- INQ000048480_0003 para 8
- INQ000414515_0045-0046 para 101
Chapter 6: The second wave (mid-July to early December 2020)
Introduction
| 6.1. | By September 2020, a second wave of Covid-19 had struck the UK. All four nations saw a sharp increase in the number of infections.1 By 23 September, the reproduction number (R) was “almost certainly” above 1 across the UK and, by 30 September 2020, was between 1.3 and 1.6.2 In England, Wales and Northern Ireland, this ultimately led to the imposition of further lockdowns (in England on 5 November 2020; in Northern Ireland on 16 October; and in Wales a 17-day ‘firebreak’ on 23 October). There was no Scotland-wide lockdown during this period, although regional protection levels came into effect on 2 November 2020. |
Figure 17: Daily deaths per 100,000 population by date of death from 6 July to 28 December 2020 across the UK
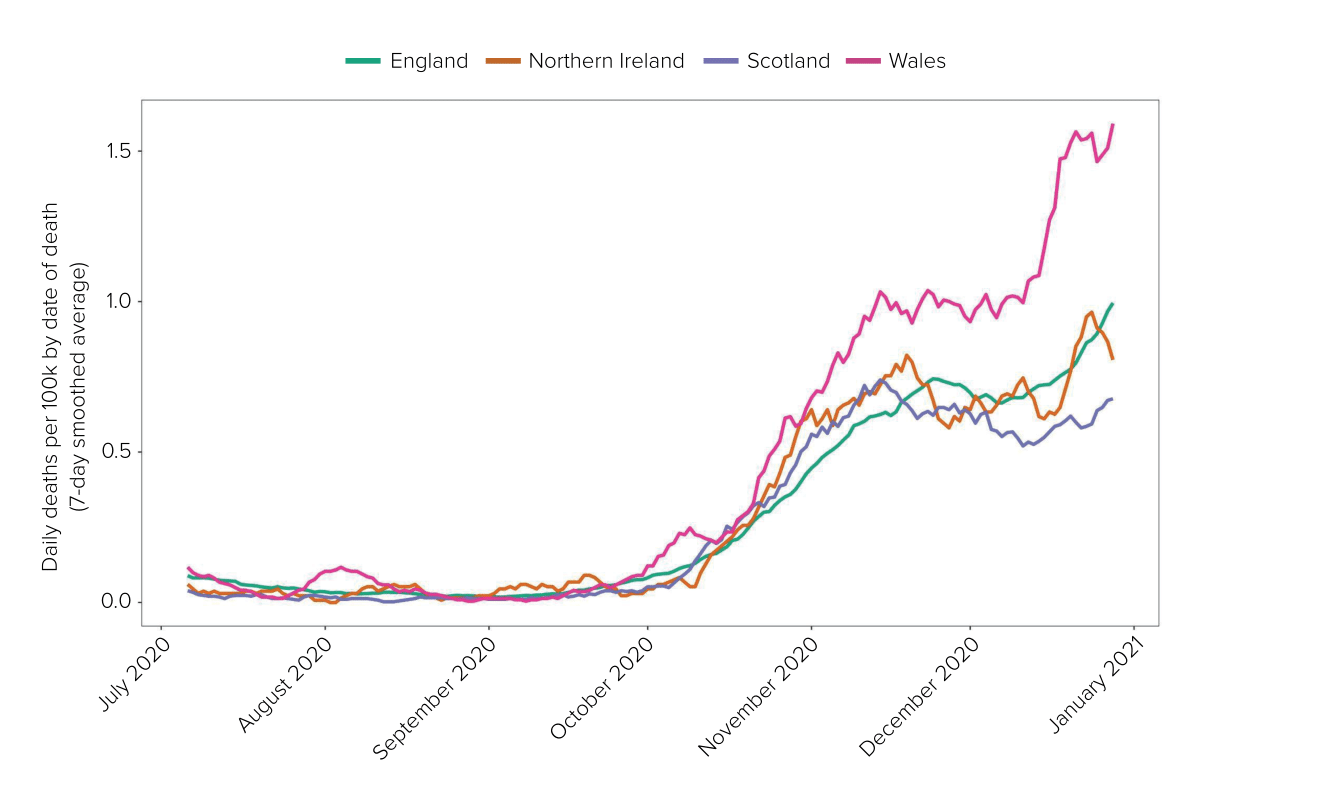
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download). (Note: Scotland joined the Coronavirus (Covid-19) Infection Survey in September 2020, at which point accurate case data became available across the whole of the UK for the first time. Deaths were a lagged indicator of changes in the number of cases prior to this point.)
| 6.2. | The second wave was predicted from early in the Covid-19 pandemic.3 Despite this, it was more deadly than the first wave, with over two-thirds of the UK’s Covid-19-associated deaths reported prior to 1 April 2021 occurring after 1 September 2020.4 |
| 6.3. | The UK should have been well equipped to respond to the developing crisis. All four nations of the UK could draw upon their own and international experience of the first wave to facilitate decision-making. The “fog of uncertainty” that had permeated the early months of the pandemic had lifted.5 Testing and surveillance capacity had been strengthened. Scientific understanding of the virus had matured. Data flows were much improved and, as a result, scientific advisers and decision-makers had access to more and better data. Intensive preparation in July and August 2020 had also been recommended to prepare for the risk of a winter resurgence of Covid-19, in light of concerns that the prevalence of the virus was increasing and would continue to do so into the winter months.6 |
| 6.4. | This chapter examines the decisions made by the UK government and devolved administrations and whether they learned or applied the lessons of the first wave. |
July and August 2020
| 6.5. | Throughout July 2020, there was a focus on relaxing restrictions, with more limited interventions and light-touch measures in place across the four nations. This included extending the mandatory use of face coverings.7 Face coverings became mandatory in shops and supermarkets in England on 24 July.8 From 10 July, a large number of countries were exempted from the travel quarantine requirements (creating ‘travel corridors’). |
| 6.6. | Shielding was paused across the four nations (with limited exceptions), beginning on various dates between 31 July and 16 August 2020.9 In Scotland, it was announced on 30 July that schools would reopen full time from 11 August 2020, after the summer holidays, following scientific evidence and advice that it was safe to do so.10 |
| 6.7. | Work continued on test and trace digital applications. These were launched in Northern Ireland at the end of July 2020, in Scotland on 10 September 2020 and in England and Wales on 24 September.11 During the autumn of 2020, the Scientific Pandemic Insights Group on Behaviours (SPI-B) and the Scientific Advisory Group for Emergencies (SAGE) advised that the effectiveness of the NHS test, trace and isolate system in reducing transmission depended critically upon self-isolation, and raised concerns about adherence to self-isolation and people’s financial ability to self-isolate.12 |
Airborne transmission
| 6.8. | As important as the test, trace and isolate system was, determining the likely routes of transmission remained a vital part of developing plans to respond to the virus. Yet policy-makers paid insufficient attention to one possible route, namely airborne transmission. |
| 6.9. | Professor Catherine Noakes, Professor of Environmental Engineering at the University of Leeds and Chair of the Environmental Modelling Group (a sub-group of SAGE), told the Inquiry that the emerging evidence in about June 2020 suggested a possibility of airborne transmission at distances beyond two metres.13 In her view, insufficient attention had been paid to the possibility of airborne transmission from as early as April 2020.14 The efforts of Professor Noakes and fellow scientists to raise their concerns is to be commended. The evidence was strengthened as more research and analysis of outbreaks was conducted, and, by 22 July 2020, the advice in a paper from the Environmental Modelling Group was clear that airborne transmission was possible in poorly ventilated spaces.15 At its meeting on 23 July 2020, SAGE endorsed this paper, “noting its findings … on the importance of good ventilation“.16 |
| 6.10. | Professor Noakes observed that “there may have been concern that declaring a disease to be airborne could lead to significant public concern“, with the term ‘airborne’ potentially invoking ideas of catastrophic viruses seen in movies.17 Professor Sir Jonathan Van-Tam (Deputy Chief Medical Officer for England from October 2017 to March 2022) stated:
“[I]f we knew then what we know now, there may well have been less emphasis on contact transmission and more emphasis on airborne transmission and ventilation.”18 |
| 6.11. | The Inquiry is considering airborne transmission (and the methods used to combat it) in the context of healthcare in Module 3: Impact of the Covid-19 pandemic on healthcare systems in the four nations of the UK. |
The UK government’s updated roadmap
| 6.12. | As discussed in Chapter 5: Exit from lockdown, in this volume, Step 3 of the UK government’s recovery strategy, laid out in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy (the May 2020 Roadmap), came into force in England on 4 July 2020.19 It did not contain any steps after 4 July.20 |
| 6.13. | Simon Case (later Lord Case), Permanent Secretary at 10 Downing Street from May to September 2020, proposed an additional chapter to include preparations for the winter and any second wave.21 This was agreed by the Covid-19 Strategy Committee (Covid-S) on 2 July 2020 and provided to Boris Johnson MP (Prime Minister from July 2019 to September 2022) in draft on 15 July.22 The draft chapter set out a plan to lift the remaining restrictions in England from 1 August 2020, with an ambition to return to normal by November 2020.23 The Covid-19 Taskforce advised that the current work-from-home messaging should remain in place.24 Mr Johnson, however, wished to provide more discretion to employers.25 Mr Case told Matt Hancock MP (Secretary of State for Health and Social Care from July 2018 to June 2021) that the taskforce’s advice was an attempt to “balance realism with Johnsonian optimism! Chris [Professor (later Sir) Christopher Whitty, Chief Medical Officer for England from October 2019] doesn’t like it.“26 Mr Hancock and the Department of Health and Social Care agreed with the scientific advice and considered the desire to return to normality by November to be “unachievable“.27 Mr Hancock was concerned that the draft chapter “underplayed the scale of risk of a second wave“.28 |
| 6.14. | Mr Johnson explained to Covid-S on 16 July 2020 that the:
“central objective was to get life back to as close to normal as possible with the country as Covid-secure as possible before Christmas“.29 Professor Whitty outlined that the return of schools in September 2020 and the winter would constitute “two significant risk moments“.30 He warned: “Lifting measures … in November would increase risks. Once the winter had ended … it would be a safer moment to take risks.“31 |
| 6.15. | Mr Johnson told the Inquiry that he made this decision having concluded:
“[S]ocial distancing restrictions were having a significant real-world impact and millions were at risk of being made unemployed … there was a sufficient arsenal of countermeasures to seek to contain the virus.”32 |
| 6.16. | The proposed approach was discussed by the UK Cabinet the following day before being publicly announced.33 Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021 and Minister for the Cabinet Office from February 2020 to September 2021, informed the devolved administrations.34 |
| 6.17. | On 17 July 2020, The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, which updated the May 2020 Roadmap, was published. It outlined the UK government’s ambition that a return to normality “may be possible by November at the earliest“.35 It stated that the virus was “in retreat“, the UK government having “opened up the economy and society carefully and cautiously“.36 It explained that the number of new infections was now “stable and low” and, consequently, from 1 August 2020 a number of sectors would be allowed to reopen, including leisure. The decision to work from home would not be subject to government guidance but would be at employers’ discretion.37 Reference was made to the possibility of the resurgence of the virus between November 2020 and March 2021, but assurance was given that plans were in place to deal with this.38 |
| 6.18. | New powers for ministers and local authorities to implement targeted local measures in England, including lockdowns, accompanied the publication of The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, along with the publication of the COVID-19 Contain Framework: A Guide for Local Decision-Makers. This framework set out decision-making for monitoring and controlling local outbreaks,39 with NHS Test and Trace, the Joint Biosecurity Centre, local authorities and Public Health England working together to take action at a local level. Local restrictions were subsequently imposed in areas in the Midlands and the north of England.40 |
| 6.19. | Throughout this period, Mr Johnson considered population segmentation and mass testing to be key to avoiding a further lockdown, as part of a focus on targeted and local interventions. An alternative ‘segmentation and shielding’ proposal had been developed in March and April 2020 by Professor Mark Woolhouse (Professor of Infectious Disease Epidemiology at the University of Edinburgh).41 Professor Woolhouse proposed ‘super-shielding’. This involved the shielding of those vulnerable to severe illness or death from Covid-19, but also targeted interventions for their closest contacts to reduce their risk of becoming infected with Covid-19 and subsequently transmitting the virus to the vulnerable person.42 Regular testing of closest contacts was a key intervention in this approach.43 |
| 6.20. | Professor Whitty had warned that population segmentation could not be relied upon to prevent the spread of Covid-19, given it was highly improbable that Covid-19 could be prevented from spreading between groups.44 SAGE also concluded that mixing between age groups presented a challenge for any population segmentation policy based on age.45 Despite this advice, Mr Johnson continued to seek plans based on population segmentation at a meeting of Covid-S on 22 July and, following a meeting with Rishi Sunak MP (Chancellor of the Exchequer from February 2020 to July 2022) and key advisers, on 29 July 2020.46 |
| 6.21. | On 23 July 2020, SAGE considered a paper from the Scientific Pandemic Influenza Group on Modelling (SPI-M) on population segmentation by age and again concluded that this was “unlikely to be successful“.47 On 6 August 2020, SAGE considered a briefing (and had available a pre-publication paper) from Professor Woolhouse and agreed that work carried out on his views by the Scottish Government advisory groups would be discussed at SAGE once complete.48 Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, and Professor Dame Angela McLean (Chief Scientific Adviser to the Ministry of Defence from 2019 to 2023 and Government Chief Scientific Adviser from April 2023) told the Inquiry that Professor Woolhouse’s proposal was unlikely to have succeeded, since increases in the incidence of Covid-19 in the wider population inevitably spilled over to shielded groups.49 Additionally, there were concerns that Professor Woolhouse’s proposal would:
“place most burden on multigenerational households … and ethnic minorities, where we know multigenerational households are more common“.50 |
| 6.22. | Work was to continue on population segmentation through to September 2020, with more “serious work on segmentation” commissioned from the Covid-19 Taskforce by Mr Johnson and Mr Sunak.51 In advice dated 7 September 2020, the taskforce concluded that segmentation could not be successfully delivered as an alternative to a “full national lockdown“.52 It would not protect public health, nor would it minimise economic harm. Further:
“It would also create a society that divides thousands of families, which would have long term societal and mental health impacts.“53 As a result, the taskforce recommended focusing on a “softer” form of segmentation that involved taking steps to increase protection of the most vulnerable, improving communication about behavioural risk and limiting social contact generally.54 Mr Johnson responded to this advice the following day, stating that “we need soft segmentation and the MOONSHOT“.55 The impact of the Moonshot programme – a same-day mass testing programme – is considered below. |
Wales
| 6.23. | Planning was also taking place in Wales with regard to localised measures. On 27 July 2020, the Welsh Government wrote to local health boards and local authorities asking them to work together on the preparation of local Covid-19 prevention and response plans to consider outbreaks of Covid-19 at a local level.56 The following day, the Welsh Cabinet noted that there was “likely to be a resurgence of the pandemic in the Autumn and Winter“.57 Plans were subsequently submitted to Public Health Wales and reviewed during August 2020. Dr Quentin Sandifer, Executive Director for Public Health Services and Medical Director at Public Health Wales from October 2012 to December 2020, said that “it was quite clear that further work was required“.58 |
| 6.24. | The intention was for the Welsh Government to provide feedback.59 However, on 21 September 2020, the Welsh Government confirmed that it would not be providing formal feedback on the plans.60 This surprised Dr Sandifer, who believed that:
“the health boards had been let off the hook and the opportunity to prepare Wales for the expected increase in case numbers as we approached the autumn had not been fully realised“.61 |
| 6.25. | Dr Sandifer was concerned that the health boards would not be prepared for the winter.62 The request to formalise local plans should have been sent to local authorities and health boards earlier in July 2020. As early as 1 July 2020, the Welsh Government had been considering the prospect of a “local lockdown“.63 Once requested, the Welsh Government should have provided feedback in a timely manner. Reg Kilpatrick (Director in the Welsh Government with responsibility for civil contingencies from 2013) agreed that the Welsh Government should have used the summer months to provide clarity about “what would happen and what should happen and what plans were available“.64 Had such clarity been provided in planning for local measures, this might have avoided the concerns expressed by local authorities with rising case rates in early September.65 |
Early warning signs of a second wave
| 6.26. | By 25 July 2020, there was grave concern in the UK government about the risk of a second wave hitting the UK. As in March 2020, developments across Europe provided an insight into what was to come. Mr Case noted:
“We are on the edge of this virus taking off again in this country – we are probably a week or two behind others in Europe, where numbers are starting to grow again.“66 These concerns were echoed by Mr Johnson in a WhatsApp message on 27 July: “Folks looking at Spain and France and remembering March it is completely obvious we are about to be hit by a second wave.“67 |
| 6.27. | On 29 July 2020, Mr Johnson sent a further WhatsApp message stating that Office for National Statistics data indicated there were 4,200 cases per day, an increase from 2,800 the previous week.68 Mr Case replied, noting a “clear warning” in the data. The growth in London was “especially worrying“. Action was required – there was “now an upward trend we can’t ignore“.69 |
| 6.28. | The following day, SAGE advised that R was likely to be above 1 in England.70 As a consequence, the Covid-19 Operations Committee (Covid-O) decided to postpone for at least two weeks the easing of restrictions proposed in The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy. The requirement to wear face coverings was extended to a wider range of indoor settings, and a decision was taken to put local restrictions in place in north-west England owing to “higher infection rates“.71 Mr Johnson considered that this would “make a material difference to the transmission of the virus and would send a warning to the rest of the country“.72 Notwithstanding the concerns, it was decided that the proposed relaxation to the work-from-home guidance planned for 1 August 2020 should still go ahead. Separately, although not discussed, the Eat Out to Help Out scheme (considered further below) was to proceed from 3 August.73 |
| 6.29. | On 31 July 2020, a telephone call took place between Mr Johnson and the leaders of the devolved nations.74 This was intended to encourage the devolved administrations to act in concert with the UK government, to prevent a disparity in messaging.75 As a consequence of information shared about the increase in infections in north-west England, the Scottish Government warned people against visiting that area.76 |
| 6.30. | Similar steps were taken in Northern Ireland following rapid increases in infection. By 30 July 2020, the Executive Committee was told of a shift in the picture of transmission in Northern Ireland, with a rise in positive cases, although this was not translating into hospital admissions. This appears to have been attributed to instances of younger people becoming infected with Covid-19.77 |
| 6.31. | On 1 August 2020, the Northern Ireland Executive Committee was advised that the seven-day rolling average number of cases per day had increased more than three-fold since the beginning of July 2020.78 On 6 August, the Executive Committee agreed to defer the reopening of non-food-serving pubs and bars, which had been due to take effect on 10 August, on the advice of Professor (later Sir) Michael McBride (Chief Medical Officer for Northern Ireland from September 2006) and Professor Ian Young (Chief Scientific Adviser to the Department of Health (Northern Ireland) from November 2015).79 Part of the rationale for this advice was to ensure that schools could reopen and to prevent a scenario “that puts general lockdown measures back on the agenda“.80 The Executive Committee also decided that the use of face coverings in certain indoor settings, including shops, would be mandatory from 10 August (although children aged under 13, or people who could not wear a mask for health or disability reasons, were exempt).81 By 13 August, there had been a rapid increase in transmission (particularly among young people) and there was a stronger upwards trajectory of case rates in Northern Ireland than there was in Great Britain (England, Wales and Scotland) or the Republic of Ireland.82 |
| 6.32. | On 13 August 2020, SAGE estimated that R was between 0.8 and 1 in England, but said that it might be above 1.83 That same day, the Covid-19 Taskforce advised Mr Johnson that, while the UK government should implement the proposed easing of restrictions on 15 August, this should be balanced with tougher messaging on enforcement and fines of £10,000.84 Mr Johnson agreed and this was announced.85 |
| 6.33. | On 18 August 2020, the Welsh Cabinet also agreed to relax restrictions from 22 August to allow up to four households to meet. Indoor meals with up to 30 people following a wedding, civil partnership or funeral would also be allowed. The Welsh Cabinet noted that the number of new daily cases in Wales was between 15 and 24, although the increase in cases in England was a “cause for concern“.86 |
| 6.34. | On the same day, the Welsh Government published the Coronavirus Control Plan for Wales.87 This noted that, while case rates in Wales were currently low, “we know from experience elsewhere in the world just how quickly the virus can return, and how swiftly it can spread“.88 It outlined the Welsh Government’s plans for management at a local level, with the health boards working closely with local authorities. However, it did not provide sufficient clarity for local authorities.89 By 21 August 2020, modelling for Wales was still at an ‘all-Wales’ level. The Technical Advisory Cell recommended breaking down the modelling at a local level.90 |
| 6.35. | The Northern Ireland Executive was also considering localised measures. However, this was in the context of the higher incidence in Northern Ireland: R was higher in Northern Ireland than in the rest of the UK or the Republic of Ireland.91 On 20 August 2020, the Executive considered the possible need for local restrictions, with proposals for tightening restrictions on public and private indoor and outdoor gatherings.92 Ministers expressed concerns about enforcement, whether hospitality venues were ‘gaming’ the system, and pubs being packed with people.93 They agreed that local restrictions “should not be adopted at this time but this option should be kept open“. They tightened restrictions on gatherings with effect from 25 August.94 |
| 6.36. | On 20 and 27 August 2020, SAGE repeated its advice that R might be above 1 in England.95 |
The Eat Out to Help Out scheme
| 6.37. | The Eat Out to Help Out scheme offered discounts across the four nations on eating out from Monday to Wednesday between 3 and 31 August 2020.96 |
| 6.38. | The scheme was developed by Mr Sunak and the Treasury from May 2020 and was agreed by Mr Johnson before its implementation.97 Mr Sunak explained that he and Mr Johnson “thought that there was a sound policy rationale for introducing the scheme“.98 Both referred to the scheme providing financial support to the hospitality sector, given the impact of the first lockdown.99 There was a second, equally significant objective:
“To incentivise consumers to return to the hospitality industry … by reassuring people that [it] is once again safe to consume and altering social behaviours that have become entrenched.“100 The rationale for creating a month-long scheme rather than a one-off financial incentive was that an ongoing incentive was more likely to achieve the scheme’s policy aim of “breaking entrenched behaviours and encouraging the return to social consumption“.101 It reflected the importance of household consumption “for both the performance of the economy and employment in the near and long-term“, given that this represented “63% of GDP [gross domestic product] … the largest part of the economy“.102 |
| 6.39. | Mr Sunak emphasised that the Eat Out to Help Out scheme was implemented in the context of “the safe lifting” of restrictions and the reopening of pubs, restaurants and hairdressers, as agreed by the UK Cabinet on 23 June 2020 and announced that day.103 He explained that restrictions applied to hospitality venues during the operation of the scheme, such as:
“Covid-secure guidelines … This included placing limits on group sizes … ensuring a safe distancing between different groups, and the maintenance of social distancing measures of ‘one-metre plus’.“104 Specific guidance had also been provided.105 As outlined in Chapter 5: Exit from lockdown, in this volume, social distancing guidance in England had already been reduced by the UK government – contrary to scientific advice – from two metres to one metre, in part in order to enable hospitality venues to open profitably. |
| 6.40. | The Eat Out to Help Out scheme applied UK-wide. However, the devolved administrations were neither consulted nor informed before it was announced.106 Both Mr Sunak and Nicola Sturgeon MSP, First Minister of Scotland from November 2014 to March 2023, told the Inquiry that the UK government had not been obliged to do so under the devolution settlement.107 Even so, consulting the devolved administrations would have been sensible, given the potential public health implications of the scheme. |
| 6.41. | The Inquiry has not seen any evidence that the Treasury took into account the differing epidemiological conditions in the devolved nations when designing the Eat Out to Help Out scheme. It has seen limited evidence that the Treasury considered the different approaches to the response being pursued in each nation. It is difficult to see how the Treasury could adequately have done either, given the lack of consultation. At the time, there was no mandatory requirement to wear face coverings in indoor settings in Wales, despite pubs and restaurants reopening on 3 August 2020.108 Such premises were still required to take all reasonable measures to maintain a two-metre social distance.109 The Scottish Government was focused on the “maximum suppression” of the virus during this period.110 Northern Ireland was facing significantly increased infection rates, and Professors Young and McBride had advised that pubs that did not sell food and were due to reopen should not do so.111 By failing to consult the devolved administrations, the Treasury risked undermining the strategies that the devolved administrations had implemented in order to reduce infections. |
| 6.42. | Mr Johnson, Mr Sunak and the Treasury also failed to consult or inform other UK government decision-makers, including Mr Hancock and senior advisers in the Cabinet Office, the Department of Health and Social Care and the Covid-19 Taskforce, about the Eat Out to Help Out scheme.112 These decision-makers, along with the devolved administrations, were deprived of the opportunity to raise any concerns or to influence the scheme. |
| 6.43. | Mr Johnson initially told the Inquiry that the Eat Out to Help Out scheme was “properly discussed, including with Chris [Whitty] and Patrick [Vallance]”.113 However, he subsequently confirmed that no scientific advisers were present at his meetings with Mr Sunak at which the scheme was discussed.114 The Treasury, Mr Sunak and Mr Johnson failed to seek scientific advice in relation to the potential epidemiological risks of the scheme, despite being advised by Professor Whitty about the risk of indoor hospitality settings.115 Professor Whitty explained:
“I do not think Treasury officials would have needed to consult me to know what I would have said however … I highlighted the risks of hospitality venues from very early in the pandemic multiple times.“116 |
| 6.44. | Whether or not the scheme had a significant impact on the transmission of the virus (which Mr Sunak denied), it presented, at face value, a risk of increased transmission and was devised in the absence of any scientific advice. The scheme was also inconsistent with the UK government’s overarching public health objectives for the response. As a number of witnesses observed, it undermined public health messaging about the importance of social distancing and being cautious in respect of socialising indoors.117 Professor Vallance explained that “up to that point the message had been very clear: … interaction between different households and people … was a high risk activity. That policy completely reversed it.” It also provided financial incentives to engage in such activity. It was “a completely opposite public health message“.118 Lee Cain (Director of Communications at 10 Downing Street from July 2019 to November 2020) agreed, considering that the scheme:
“sent the wrong message to the country at a time when we were also trying to urge caution and keep social interaction limited and the virus under control“.119 |
The situation at the end of August 2020
| 6.45. | The situation in Europe continued to foreshadow what was to come to the UK. By the end of August 2020, the real risk that the UK would be hit by a second wave of Covid-19 was clear to Mr Johnson and other decision-makers. |
| 6.46. | On 28 August 2020, the Covid-19 Taskforce had provided Mr Johnson with advice on strategy for the autumn of 2020.120 It outlined an optimistic plan A for a return to normal in November 2020, an alternative plan B for normality by Christmas 2020 and a contingency plan C for an England-wide response, if needed. While emphasising the importance of testing programmes to avoid another lockdown, Mr Johnson responded:
“We can and must deliver a version of plan A by Xmas … We are about to be HIT by French/Spanish LEVELS of infection. We must not DELUDE ourselves. So we must set out a new vision that does not involve another LOCKDOWN.“121 (emphasis in original) |
| 6.47. | Mr Case complained about Mr Johnson:
“He changes strategic direction every day (Monday we were all about fear of virus returning as per Europe, March etc – today we were in ‘let it rip’ mode cos the UK is pathetic, needs a cold shower etc). He cannot lead and we cannot support him in leading with this approach. The team captain cannot change the call on big plays every day.“122 |
| 6.48. | On 29 August 2020, Mr Johnson noted that the exponential spread of Covid-19 in France “will hit us unless we are insanely lucky“.123 Two days later, he stated: “[W]e have seen the wave coming for miles so we should be ready.“124 Mr Hancock told the Inquiry that “it was clear that a second wave was coming from late-August“.125 |
| 6.49. | The UK government’s focus throughout this period had been on lifting restrictions, with limited planning for a second wave. The use of localised restrictions and targeted interventions, such as ‘smart’ non-pharmaceutical interventions and consideration of population segmentation, had been prioritised. However, the measures that had been taken had not worked. Moreover, although face coverings had become mandatory in a number of settings in England, Mr Johnson described the policy as “totally fucked up“.126 |
September 2020
| 6.50. | The situation continued to worsen in September 2020. In Northern Ireland, on 1 September, R was noted to be “steady at 1.3“, but there was an increase in intensive care and hospital admissions. Certain council areas had concerning case numbers.127 As explained in Chapter 5: Exit from lockdown, in this volume, Professor Young had said that Northern Ireland could just about cope with R of 1.2, but not with anything higher.128 |
| 6.51. | At a UK Cabinet meeting on 1 September 2020, Professor Whitty repeated his earlier advice, while Professor Vallance pointed to France, where younger people were transmitting the virus to the older population, resulting in increasing hospitalisation rates.129 Mr Johnson acknowledged that increasing case rates in France and Spain served as a “warning” to the UK, with “no room for complacency“. He was clear, however, that “a national lockdown should not be reimposed and schools would not be instructed to close again“. Mr Johnson’s preference was to focus on building an effective test and trace system, combined with “strong local lockdowns” as and when required.130 |
| 6.52. | On 3 September 2020, Professor Whitty emailed Mr Case. While acknowledging Mr Johnson’s “strong desire to avoid a national lockdown”, Professor Whitty advised that a scenario in which this intervention was needed should be considered “quite seriously”. He suggested that a “2-3 week partial or full lockdown” would act as a “fire break,” and a “return from a doubling to a halving of the virus“.131 Two days later, Professor Whitty emailed Mr Case again, cautioning that the growing test positivity rates were a “depressingly reliable early indicator of trouble … this is not yet trouble, but is heading for trouble”.132 At this point, the death rate in the UK remained low.133 However, as Professor Whitty explained:
“[T]here was a lag time between infections and deaths … if the Government waited for deaths to increase before it took action, that would inevitably result in a substantial number of deaths.”134 |
| 6.53. | Rising case rates were also being seen in Wales.135 On 8 September 2020, Caerphilly was designated as the first ‘local health protection area’ in Wales, and saw the implementation of targeted local restrictions.136 That same day, it was noted that a number of other local authorities were at the “cusp of reaching threshold” for consideration of more stringent measures.137 Dr Sandifer had earlier outlined his concerns about the likelihood of increasing demands on the NHS, due to a “significant risk of exponential spread of the virus“, and about the ability to control infection rates through Test, Trace, Protect (the Welsh Government’s system of testing and contact tracing).138 He had again raised the need for urgent work on strengthening the local prevention and response plans.139 |
| 6.54. | In Scotland, the Scottish Government Covid-19 Advisory Group raised concerns with Professor (later Sir) Gregor Smith (Interim Chief Medical Officer for Scotland from April to December 2020 and Chief Medical Officer for Scotland from December 2020) in mid-September 2020 that the pandemic was “[c]urrently heading fast in wrong direction” and that a second peak would happen in November 2020.140 Ms Sturgeon concluded, on the advice of Professor Smith, that it would be “vital to go as far as possible” in reducing the R number.141 The Scottish Government would take action across a similar range of areas as the rest of the UK, but with proposed changes to “reflect the Scottish Government’s existing precautionary approach“. This was noted by Ms Sturgeon to be stricter than the approach adopted by the UK government.142 |
| 6.55. | The UK appeared to be following a similar trajectory to its European neighbours. At a UK Cabinet meeting on 8 September 2020, Mr Hancock noted that the death rate in France had just doubled over a three-week period.143 Data from the Joint Biosecurity Centre showed that the evolution of the case rate was consistent with that in France and Spain, which were four weeks ahead of the UK in terms of resurgence.144 This was an ominous forecast of what lay ahead. Mr Johnson told the Cabinet on 8 September:
“[T]he trend was clear … The Government would take action now so that the UK would not suffer the same consequences as those countries.“145 |
The rule of six
| 6.56. | That action was discussed in a meeting of Covid-S the same day, chaired by Mr Johnson. It noted that proposals would be developed to increase compliance with self-isolation, standardise local interventions into tiers and strengthen border control policies.146 |
| 6.57. | In terms of the strategic approach, the Covid-19 Taskforce advised that there were two choices in the short term:
The taskforce’s recommendation was to “double down on the current strategy” (the softer approach) with “more forceful communications, tighter social contact and tougher enforcement“. This included changing the guidance for indoor mixing from a maximum of two households to a “fixed number“, which “may be easier to understand, comply with and enforce“.148 A fixed number of six or eight was raised by Simon Ridley (Director General for Policy and Strategy on the Covid-19 Taskforce from May 2020 to July 2021) and discussed.149 This was to develop into the ‘rule of six’. |
| 6.58. | Professor Vallance advised:
“[I]t was not possible to quantify the impact of a social contact limit of eight as opposed to six, although the lower the number the better from a transmission perspective.”150 He suggested that the UK’s response should be “quick and hard“.151 Professor Whitty warned: “[T]he more steps taken to make it easier to bring households together, the more likely that the brakes would need to be slammed on hard later.”152 |
| 6.59. | Despite this, Mr Johnson agreed to set a single numerical limit of “6 people in all settings including private homes”, without any limit on the number of households.153 This “would be simple and enable tough enforcement”. Any social gathering of more than six people would be against the law, unless it fell within a limited number of exemptions.154 Mr Gove relayed the UK government’s intentions to the leaders of the devolved nations on 9 September 2020.155 |
| 6.60. | The rule of six was implemented in England on 14 September 2020, five days after its announcement.156 During that time, the number of infections had continued to grow.157 In his contemporaneous evening notes from September 2020, Professor Vallance recorded that it felt:
“like Feb/March … strikes me that the delay in introducing the new rules until Monday is exactly what they did in March. Why delay??“158 |
| 6.61. | SAGE had provided “no specific advice” on the rule of six.159 It ought to have been consulted by the UK government. Neither Professors Vallance nor Whitty believed that this measure alone could reduce R below 1. Professor Vallance told the Inquiry that he was “confident” he had communicated this advice to Mr Johnson.160 Their views were reflected in the subsequent SAGE minutes of 10 September 2020, which stated:
“It is highly likely that further national and local measures will be needed to bring R back below 1 in addition to those already announced. An early and comprehensive response would mean that measures have more effect and may be needed for a shorter duration.“161 |
| 6.62. | More significantly, far from the recommended “tighter social contact“, the rule of six in England in fact represented a loosening of the guidance.162 Instead of the previous two-household limit indoors, the new measure permitted mixing across as many as six households, so long as the total number of people meeting did not exceed six. Although the rule of six changed over time, the initial guidance applying the same limits in all settings failed to distinguish between the relatively higher risk of transmission indoors compared with outdoors. Professor Whitty warned Covid-O that “the number of households meeting was one of the biggest determinants of spread”.163 Dominic Cummings, Adviser to the Prime Minister from July 2019 to November 2020, described the rule of six as “a bad decision made under the influence of communication concerns”.164 |
| 6.63. | Fewer households were able to meet under the rule of six in Scotland, Wales and Northern Ireland, although younger children were exempted from the six-person limit.165 |
Table 3: The rule of six by nation, September 2020
| Nation | Implemented | Household limits | Position of children |
|---|---|---|---|
| England | 14 September 2020 | None | Included |
| Scotland | 14 September 2020 | No more than two | Under 12s excluded |
| Wales | 14 September 2020 | Four households per one exclusive 'bubble' | Under 11s excluded |
| Northern Ireland | 25 August 2020 | No more than two | Under 12s excluded from 17 September 2020 |
| 6.64. | The Northern Ireland Executive had previously restricted indoor gatherings in private dwellings to six people from no more than two households from 25 August 2020, in response to rising infection rates.166 On 17 September 2020, this was extended to hospitality settings.167 Scotland, similarly, limited the six people to two households.168 |
| 6.65. | The Welsh Government had already agreed to impose restrictions on the number of households that could meet at its review on 18 August 2020, and agreed on 8 September 2020 that those limits should remain in force.169 On 11 September, Mark Drakeford MS, First Minister of Wales from December 2018 to March 2024, announced the introduction of the rule of six from 14 September 2020. A total of six people from one extended household (comprising a maximum of four households) could meet indoors.170 Mr Drakeford confirmed that Wales had adopted the same number “because of simplicity of messaging“.171 |
| 6.66. | The rule of six was accompanied by an announcement of, in Mr Johnson’s words:
“an alternative plan which could allow life to return closer to normality. And that plan is based on mass testing.“172 This was the Moonshot programme: testing was to be used to identify people who were Covid-19 negative to allow them to return to normal life. The Moonshot programme was distinct from test and trace initiatives. Scientific advice provided in August 2020, prior to the announcement of the policy, was that such mass testing would have minimal effect on the strategic aim to reduce R.173 Furthermore, the effectiveness of mass testing would: “depend on several factors including the proportion of the population tested; the frequency of testing; the ability of a test to identify true positives and negatives; the speed of results; and adherence to isolation“.174 |
| 6.67. | Concerns were raised about the potential negative impact on resourcing NHS Test and Trace, with advice that it needed to be “optimised” and remain a “priority“.175 This was reiterated in advice from Professor Whitty in November 2020, who explained that the evidence that mass testing would have a useful impact was “weak” and that there were “clear and major opportunity costs“.176 Diversions and delays in testing time turnaround “would definitely lead to a net loss for public health“.177 |
| 6.68. | The rule of six was also undertaken alongside other measures across the devolved nations. Each nation was facing an acceleration of Covid-19 cases. The Scottish Government had been considering whether it needed to “put the brakes on” the further lifting of lockdown measures.178 Planned relaxations to some restrictions, scheduled for 14 September 2020, were delayed until 5 October 2020 and amendments were made to face covering requirements.179 The Northern Ireland Executive also deferred proposed hospitality openings.180 |
| 6.69. | Covid-19 infections in Wales had tripled in the four days preceding 8 September 2020, representing “the largest number of daily infections since May“.181 Professor Christopher Jones, Deputy Chief Medical Officer for Wales from June 2010, provided advice on 10 September that supported mandatory face coverings and further restrictions on household gatherings.182 |
| 6.70. | On 10 September 2020, the Northern Ireland Executive agreed to introduce localised restrictions in Greater Belfast, Ballymena and three other postcode areas for an initial period of two weeks (subject to weekly monitoring and review).183 Reflecting the urgency of the situation, Professor McBride said that he was “profoundly concerned” and urged ministers “to take affirmative action … soon. Don’t have days to wait.“184 |
| 6.71. | Professor Young explained to the Inquiry that, while the impact of localised restrictions in the context of rising transmission rates was uncertain, and it was recognised that the impact was likely to be transient, they were worth trying in an effort to reduce transmission.185 Professor McBride described localised restrictions as the “least worst option” when they were considered by the Northern Ireland Executive in September 2020.186 |
| 6.72. | SAGE and Wales’s Technical Advisory Cell both observed on 10 and 11 September 2020 that the situation in the UK was similar to the one in early February 2020 and that early action was required to stall the increase in cases.187 |
| 6.73. | There had been a particularly steep rise in case rates across the north-east of England, West Yorkshire, the Midlands and parts of north-west England. On 18 September 2020, these areas were made subject to local restrictions.188 |
Face coverings
| 6.74. | The Welsh Government was the last of the four nations to mandate the wearing of face coverings in shops and supermarkets, on 14 September 2020. It had also been the last to mandate their use on public transport, on 27 July 2020.189 Dr (later Sir) Frank Atherton, Chief Medical Officer for Wales from August 2016, told the Inquiry that he felt he had been “putting ministers in actually quite a difficult position” by taking a different position from the Chief Medical Officers for the other three nations, but he was:
“trying to make sure that ministers understood that this was their decision but my advice was that the evidence was not robust“.190 |
| 6.75. | Mr Drakeford explained that the Welsh Government did not mandate face coverings sooner because:
“While the Chief Medical Officer for Wales’s advice remained explicitly against making them mandatory, I felt it important to support that position. Not to have done so would have eroded trust between decision-makers and advisers and, more importantly, would have eroded trust amongst the public that the Welsh Government was committed to following best advice, even when that advice was controversial.“191 Mr Drakeford did, however, “absolutely agree” that the Welsh Government had had the choice to go against that advice.192 |
| 6.76. | Looking back, Sir Frank Atherton said that it “would have been better to align” with the position on face coverings in England.193 Mr Drakeford told the Inquiry that, by the time the Welsh Government changed its advice on face coverings, Dr Atherton had “moved away from the argument that [they] would do more harm than good“.194 |
| 6.77. | The concerns raised by Dr Atherton regarding the supply of masks to the NHS, the adoption of risky behaviours and the potential for discrimination could have been addressed through clear communication and guidance in a similar way to the UK government’s advice about the use of face coverings in its May 2020 Roadmap.195 |
| 6.78. | The experience of the Covid-19 pandemic has shown that wearing a face covering has minimal disadvantage for the majority of the population. In any future pandemic where airborne transmission is a risk, the UK government and devolved administrations should give real consideration to mandating face coverings for the public in closed settings. At the very least, they should strongly advise that face coverings are worn by those who are able to do so in settings such as public transport, supermarkets, and health and social care settings. Further, it would be beneficial for governments to align their positions to avoid confusion, particularly if they are in receipt of the same or similar expert advice (such as from SAGE, the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) or the World Health Organization). |
Consideration of a circuit breaker in England
| 6.79. | By mid-September 2020, the situation in England was approaching crisis point. Despite uncertainties in the data, the Operational sub-group of SPI-M (SPI-M-O) stated that there was “complete consensus that the epidemic situation is very serious” and warned:
“[T]he epidemic is close to breaching the agreed Reasonable Worst Case Scenario on which NHS, DHSC [Department of Health and Social Care] and HMG [UK government] contingency plans are based.“196 |
| 6.80. | On 17 September 2020, SAGE advised that a “‘circuit-breaker’ type of approach” with “a 2-week period of restrictions similar to those in force in late May” could have a “significant impact on transmission” and could delay “the epidemic by approximately 4 weeks“. Individual interventions were “highly unlikely” to bring R below 1, and SAGE emphasised that effective operational response measures were “absolutely critical, particularly in care homes, hospitals, workplaces and Test, Trace and Isolate (TTI) systems“.197 |
| 6.81. | R was estimated to be between 1.2 and 1.4 in England, with the caveat that it was believed to be higher given the “recent changes from the last 2 to 3 weeks such as the reopening of schools in England“.198 Critically, SAGE estimated that the growth rate equated to:
“a doubling time for new infections of 10 to 20 days, though currently this doubling time could be as short as 7 days nationally and even shorter in some areas“.199 SAGE therefore agreed to prepare an updated paper for the Cabinet Office by 21 September 2020, noting that “speed of response is key“.200 |
| 6.82. | SPI-M-O advised that a ‘circuit breaker’ (a short-term set of restrictions of pre-determined length) would be most effective when growth of the epidemic was relatively low (ie with R at or below 1.2).201 Professor Graham Medley (Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine and Co-Chair of SPI-M-O from January 2020 to February 2022) explained that a circuit breaker aims to:
“keep prevalence low whilst it is low, in contrast to emergency breaks which aim to reduce prevalence once it becomes high“.202 |
| 6.83. | R in England had already exceeded 1.2. The UK government’s daily cross-departmental Covid-19 Dashboard set out data from the Coronavirus (Covid-19) Infection Survey that showed cases were growing rapidly.203 The conditions in which SPI-M-O considered a circuit breaker would be most effective were already at risk. |
| 6.84. | Following the SAGE meeting, Mr Cummings encouraged Mr Johnson to adopt the approach put forward by SAGE, noting that the “[l]esson of first wave was earlier better when dealing with exponentials“.204 Professor Vallance reiterated the point he had made earlier in September 2020 that the “lesson is go fast, go a bit harder than you think you need, go a bit wider in geography“.205 |
| 6.85. | On 18 September 2020, Mr Case (by now Cabinet Secretary and Head of the Civil Service) told Mr Hancock that “the fire-break idea is gaining traction” with the Prime Minister.206 Later that day, however, he advised:
“PM [Prime Minister] wants to double down on present strategy for now – tougher local lockdown/enforcement, warning messages about what happens if people don’t follow the rules.“207 |
| 6.86. | Sadiq Khan (later Sir Sadiq Khan), Mayor of London from May 2016, wrote to Mr Johnson expressing his:
“firm view that we should not wait for this virus to again spiral out of control before taking action and the best thing for both public health and the economy is new restrictions imposed early, rather than a full lockdown when it’s too late“.208 |
| 6.87. | On 19 September 2020, Professor Vallance recorded in his evening notes:
“He [Mr Johnson] is all over the place and completely inconsistent. You can see why it was so difficult to get agreement to lockdown 1st time.“209 |
| 6.88. | That day, the Covid-19 Taskforce produced its ‘COVID-19: Winter strategy’.210 This presented a stark reality. The seven-day average of confirmed cases had more than tripled from mid-August 2020 and was “on a sharply upward trajectory“. This had translated into a doubling of hospitalisations within the fortnight and the potential for NHS overwhelm within six weeks. SAGE modelling suggested that the first wave’s peak of infections could be surpassed by mid-October 2020, and hospitalisations and deaths by early November 2020.211 |
| 6.89. | However, the Covid-19 Taskforce asked Mr Johnson to consider three potential ‘packages’ of interventions: A, B and C. Package A contained the least stringent measures and Package C the most stringent, including a circuit breaker.212 Within Package C – essentially a lockdown but lighter than the lockdown beginning in March 2020 – non-essential retail, universities and schools would nonetheless remain open. The taskforce recommended Package A, which included a national address by Mr Johnson, a return to guidance that people work from home where they could, and “a codification of our local interventions into tiers, as agreed at the COVID-Ops Committee [Covid-O]”.213 It observed:
“Package A is designed to change behaviour while minimising economic harm. UK GDP is still 11.7% below February levels, after a record fall of 20.4% in Q2 [April to June] 2020. There is a risk that interventions may have a more significant impact than in March, given the weakened position of many firms and individuals, and would compound existing inequalities.“214 However, it also noted: “It is the view of the CMO [Chief Medical Officer] and GCSA [Government Chief Scientific Adviser] that, unless it prompts a significant behavioural response, Package A is very unlikely to drive R below 1.“215 The taskforce further advised that there was a risk that even a combination of Packages A and B, or Package C, would “fail to bend the curve, leaving R above 1“.216 |
| 6.90. | Although both Professors Whitty and Vallance recommended a circuit breaker, this was not the Covid-19 Taskforce’s unequivocal recommendation – hence Mr Johnson’s observation that a circuit breaker had not been pressed hard on him.217 |
| 6.91. | On 20 September 2020, Mr Johnson held a “challenge session” over Zoom to hear arguments from a range of scientists, including “some highly-qualified critics of the Government’s approach to date“.218 Mr Sunak and Professors Whitty and Vallance were invited but Mr Hancock and Mr Gove were not. Mr Johnson said that he was aware of their views and “wanted time to quiz the experts myself“.219 He said that he considered it “important to hear some alternative views“.220 Mr Hancock, however, was “astonished that No10 [10 Downing Street] could organise such a meeting without inviting the Health Secretary“.221 |
| 6.92. | Professor John Edmunds (Professor of Infectious Disease Modelling at the London School of Hygiene & Tropical Medicine) advised Mr Johnson that the UK’s response needed to be “fast and large“.222 He recommended the imposition of “an immediate circuit breaker (two-week lockdown)“, urging that the UK “should not make the same mistake” as it did in March 2020.223 He reminded the meeting that the “key factor for the large number of deaths in the UK was the lateness of our response“.224 Professor McLean cautioned that test and trace would not function effectively in a large second wave.225 She advocated “decisive action” with a circuit breaker, but with schools remaining open.226 |
| 6.93. | Dr Anders Tegnell, Swedish state epidemiologist, was also in favour of further action by the UK government. He told the meeting that “the myth that Sweden did nothing during the pandemic is false“.227 Sweden is frequently cited as a country that did not implement a lockdown but that successfully brought the virus under control. It is true that, rather than imposing mandatory measures, the government issued guidelines recommending social distancing, the avoidance of non-essential travel and working from home where possible. Businesses and primary schools largely remained open. Gatherings of more than 50 people were, however, banned and secondary schools and universities switched to remote learning.228 |
| 6.94. | In a study that Imperial College London undertook comparing the first wave of the pandemic in the UK, Denmark and Sweden, it found that Sweden achieved almost the same level of reduction in contact rates (as reflected in workplace mobility changes and the proportion of people avoiding public spaces) as many other European countries. These included its neighbour, Denmark, which instituted a suite of mandatory policies. However, Swedish control measures took longer to reduce R below 1 than did the measures adopted by both the UK and Denmark, and achieved a lower overall reduction in R. |
| 6.95. | By contrast, Professor Sunetra Gupta (Professor of Theoretical Epidemiology) and Professor Carl Heneghan (Professor of Evidence-Based Medicine), both at the University of Oxford, rejected the concept of a national lockdown.229 They proposed an alternative approach: “focused protection” of those who were most vulnerable to severe disease and death, while allowing the unrestricted spread of infection in the non-vulnerable population.230 This had parallels with Mr Johnson’s interest in population segmentation. Professor Gupta highlighted the social, economic, psychological and developmental harms caused by lockdowns. She asserted that focused protection was “the only humanitarian route out of the crisis“.231 Professor Heneghan argued that the UK government’s response to the crisis was:
“out of proportion to the threat … underpinned by a lack of understanding of the data, the role of community pathogens and an overreliance on predictive modelling“.232 He also said that “there will be more deaths, but there needs to be context … deaths are lower than influenza/pneumonia“.233 |
| 6.96. | There was considerable criticism of the approach advocated by Professors Gupta and Heneghan. Mr Hancock described them as “discredited anti-lockdown proponents” who “did not represent credible scientific thinking“.234 Mr Johnson told the Inquiry that he was “certainly willing to be persuaded” by the views of Professors Gupta and Heneghan. He recalled, however, that they were in fact “reluctant to argue any such case, or not very hard“.235 |
| 6.97. | Professor McLean told the Inquiry:
“Among the more important inaccurate assertions made by Professors Gupta and Heneghan were that: most of the population were immune (‘dark immunity’), we could not measure immunity, we should let everyone acquire immunity by allowing a huge second wave because we could fully shield all the vulnerable, and that Covid-19 was less dangerous than influenza.“236 |
| 6.98. | In advance of an upcoming Covid-S meeting and having considered the Covid-19 Taskforce’s ‘COVID-19: Winter strategy’, Mr Johnson’s view on the evening of 20 September 2020 was to “pursue all of Package A nationally, and some measures from Package B” (greater restrictions, including a curfew for hospitality and weddings).237 |
| 6.99. | On 21 September 2020, Mr Cummings chaired a “hypothetical future meeting” with Mr Johnson and 10 Downing Street officials. He hoped to push Mr Johnson:
“into the mental state the data suggested he would be in at the end of October, and make him realise what he would then do“.238 This followed supplemental advice and projections about infections and deaths from the Covid-19 Taskforce provided on 20 September. Notwithstanding its recommendation of the least restrictive Package A measures the day before, Mr Ridley said that the presentation aimed to “prompt action“.239 |
| 6.100. | Mr Cain recalled that the evidence in favour of a circuit breaker at this meeting was:
“overwhelming, with the data and overwhelming expert opinion being that if the Government did not take action in the form of a circuit breaker, Covid would once again spread rampantly across the UK and leave no other option than a longer and more restrictive lockdown in the months ahead. The PM remained unconvinced, believing it would be better to ‘keep the beaches open’ (a reference to the film Jaws) and not to close down the economy for a second time.“240 Without a circuit breaker, Covid-19 would: “leave no other option than a longer and more restrictive lockdown in the months ahead … The Downing Street team believed it would be better for the economy and for the health of the nation to implement a circuit breaker as this would mean spending less time in lockdown.“241 Mr Johnson was “not persuaded” that a circuit breaker was a “good idea“.242 |
| 6.101. | On 21 September 2020, SAGE repeated its earlier advice “with more urgency“. A package of interventions was needed to reverse the exponential rise in cases. A shortlist of measures “should be considered for immediate introduction“.243 These included: a circuit breaker lockdown; working from home; closure of hospitality settings and personal services; a move to online learning for college and university students; and a ban on socialising with people from outside the household in the home.244 Mr Johnson said that this advice, as well as subsequent advice up to 22 October 2020, was “never … pushed on me very hard“.245 |
| 6.102. | SAGE noted that each intervention had “associated costs in terms of health and wellbeing and many interventions will affect the poorest members of society to a greater extent“. However:
“The more rapidly interventions are put in place, and the more stringent they are, the faster the reduction in incidence and prevalence, and the greater the reduction in COVID-related deaths (high confidence). Both local and national measures are needed; measures should not be applied in too specific a geographical area.“246 |
| 6.103. | In a briefing for Mr Sunak in advance of a meeting of Covid-S on 21 September 2020, the Treasury stated:
“We are reaching the limits of what we can do economically, with further measures likely to be catastrophic. We need a strategy that works over the winter period, rather than tinkering with restrictions week to week.“247 The briefing advised Mr Sunak to “push back strongly on the circuit breaker proposal“, on the basis that its “economic impacts would be severe, making firm failures and redundancies far likelier“.248 In a briefing to the Cabinet and COBR on 22 September, the Treasury emphasised that the UK: “must avoid at all costs returning to national economic restrictions that will devastate sectors that are already extremely vulnerable“.249 |
| 6.104. | Mr Sunak told the Inquiry that he had not supported the use of a circuit breaker in England.250 Mr Johnson feared that the UK would “unlock and then lock down again as the cases rose” after a circuit breaker lockdown, which “might cause even worse disruption to people’s lives and businesses“.251 Mr Hancock expressed similar concerns.252 Both Professors Whitty and Vallance acknowledged that this was likely and that a circuit breaker alone would not avoid a second wave of infections. However, both considered that interventions were needed and would result in shorter, less stringent restrictions later.253 |
| 6.105. | At Covid-S, more stringent measures were rejected in favour of a combination of Package A and some additional measures, including extensions of mandatory requirements for face coverings, restrictions on household mixing and curfews in the hospitality sector.254 Mr Johnson noted that a failure by the public to adhere to the restrictions would result in further action that would be “disruptive“.255 |
| 6.106. | On 22 September 2020, the UK government and devolved administrations discussed and endorsed the measures proposed at COBR, but noted that there would be some variation in the measures put in place in each nation to reflect “local circumstances“.256 The Scottish Government noted media speculation about the circuit breaker lockdown at a Scottish Cabinet meeting that day, but had not formally considered whether such a measure should be implemented.257 |
| 6.107. | Measures were subsequently imposed to take effect in Scotland on 23 September 2020 and in England and Wales on 24 September.258 In a statement to the UK Parliament on 22 September, Mr Johnson set out new restrictions to take effect in England, including: working from home where possible; table service only in pubs, bars and restaurants; closure of hospitality venues at 22:00; extended requirements on face coverings; a maximum of 15 people at wedding ceremonies and receptions; and the rule of six extended to all adult indoor team sports. The 22:00 curfew had been considered by SAGE on 21 September to be “likely to have a marginal impact. Low confidence.“ |
| 6.108. | On 22 September 2020, four more local authorities in Wales were designated as local health protection areas.259 Having met the day prior to consider the need for urgent restrictions in additional areas, due to a “substantial increase in Covid-19” infections, on 22 September the Northern Ireland Executive agreed to extend the current restrictions on household mixing to the whole of Northern Ireland, along with further restrictions on hospitality.260 |
| 6.109. | The rejection of a circuit breaker by the UK government (including COBR and Covid-S) went directly against the clear advice of SAGE. The UK government chose to implement a selection of measures that it had been warned were unlikely to be effective.261 The damaging economic and societal consequences of a circuit breaker were obvious. However, by rejecting harsher restrictions in favour of a ‘softer’ approach, the UK government failed to take the steps necessary to prevent the virus from continuing to spread at pace. This failure paved the way, in turn, for the inevitable outcome: a more deadly spreading of the virus and a lengthier, later lockdown, with greater economic impacts. |
| 6.110. | Mr Johnson told the Inquiry that the scientific advice on this intervention “was not clear“.262 This is incorrect. SAGE delivered robust and forceful expert scientific advice on the merits of a circuit breaker. The advice was unequivocal that, the more stringent the measures taken and the sooner they were implemented, the faster the epidemic would shrink and the shorter the period interventions would need to be in place. As Professor McLean pointed out, a short, intermittent circuit breaker would be less detrimental than allowing infections to “grow until you’re just about to break the NHS, and then you bring in a massive, massive lockdown“.263 |
| 6.111. | It is correct that the scientific advisers “did not believe it [a circuit breaker] was in any sense a silver bullet“.264 However, SAGE made it plain that a circuit breaker was a vital element of a wider package.265 Other scientific experts agreed. Professor Neil Ferguson, Mathematical Epidemiologist at Imperial College London, observed:
“[W]hile the measures announced were certainly better than taking no action, they did not reach the level recommended by SAGE the previous day and would at best slow the rate of growth of the epidemic.“266 |
| 6.112. | Similar scientific advice was provided to the Welsh and Scottish governments and the Northern Ireland Executive at this time. It noted that further measures might be needed if R did not fall below 1, and that such measures would have a greater impact the earlier they were introduced.267 |
The situation at the end of September 2020
| 6.113. | On 23 September 2020, SPI-M-O warned that Covid-19 was “evolving rapidly” and reiterated its support for a circuit breaker.268 SAGE warned that, unless R was reduced below 1, it was possible that infections and hospitalisations would “exceed scenario planning levels“. It reiterated the advice that “the earlier additional measures are introduced the more effective they will be“.269 |
| Nation | R | Growth rate per day |
|---|---|---|
| England | 1.2–1.5 | +4% to +8% |
| Scotland | 1.2–1.6 | +4% to +9% |
| Wales | 1.0–1.4 | +1% to +5% |
| Northern Ireland | 1.0–1.5 | 0% to +7% |
| UK | 1.2–1.5 | +4% to +8% |
| NHS England region | R | Growth rate per day |
|---|---|---|
| East of England | 1.1–1.3 | +1% to +4% |
| London | 1.2–1.5 | +4% to +9% |
| Midlands | 1.2–1.5 | +3% to +7% |
| North East and Yorkshire | 1.2–1.5 | +4% to +8% |
| North West | 1.2–1.5 | +3% to +9% |
| South East | 1.0–1.3 | +1% to +5% |
| South West | 1.1–1.4 | +1% to +6% |
| 6.114. | At an ‘extraordinary’ meeting of the Scottish Government Covid-19 Advisory Group on 27 September 2020, it was noted that the pandemic was “[c]urrently heading fast in wrong direction“, with the expectation of “a second wave in November“.270 The following day, Professor Smith and others advised Jeane Freeman MSP (Cabinet Secretary for Health and Sport in the Scottish Government from June 2018 to May 2021) that a number of measures should be introduced in Scotland from 21 September for six to eight weeks. Most significantly, they also recommended a firebreak, with a “general ‘stay at home’ order for 14 days from 12 October“.271 |
| 6.115. | Professor Smith and his colleagues, however, submitted a further paper later that day “to strengthen our position“, having considered “the emerging data and modelling“.272 They stated that action in the hospitality sector and travel restrictions “may have to be in place for at least 12 weeks“, adding:
“We remain of the view that a ‘fire break’ amounting to a general stay at home order may be required to be implemented quickly if our recommended measures do not have the desired effect. We do not propose at this stage a planned ‘fire break’ during the October school holidays but such a step may be required.“273 The advice given to the Scottish Government therefore changed from a planned firebreak lockdown to a wait and see approach. |
| 6.116. | On 28 September 2020, at a meeting with Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021, and Michelle O’Neill MLA (deputy First Minister of Northern Ireland from January 2020 to February 2022), Professor McBride advised that the Northern Ireland Executive needed to consider circuit breakers. This was because modelling suggested that cases and admissions to hospital would increase rapidly. He warned that there were “6 more difficult months ahead“.274 On 30 September, Professor McBride observed that the position was “deeply concerning” and that time was not on their side.275 |
| 6.117. | On 30 September 2020, SPI-M-O concluded that the epidemic was “likely to breach the agreed reasonable worst case scenario over the next two weeks“.276 At a UK Cabinet meeting that day, Mr Johnson acknowledged that infections were continuing to increase across the country and that deaths had soared to the highest level in three months. However, he resolved that “now was the time to wait with composure and determination for the measures to kick in“.277 |
| 6.118. | The existing measures did not work. By 1 October 2020, SAGE indicated that it was “likely that infection incidence and hospital admissions will exceed scenario planning levels in the next two weeks“.278 The latest estimate of R for the UK was 1.3 to 1.6. In Wales, 17 local health protection areas had been designated by 1 October, covering 15 of the 22 local authorities.279 Within days, the numbers of infections and hospital admissions in England were exceeding reasonable worst-case scenario planning levels.280 On 8 October, SAGE again reiterated its advice.281 |
| 6.119. | COBR met on 12 October 2020. Mr Drakeford asked if there would be a further COBR meeting to discuss the possibility of circuit breakers.282 He told the Inquiry: “The Prime Minister decided to stick with the tiered [local] approach in England.“283 By this point, Mr Drakeford had come to the conclusion that:
“local lockdowns were not enough, and work started within the Welsh Government to plan the firebreak“.284 |
| 6.120. | The Welsh Government and Northern Ireland Executive subsequently moved away from localised responses and imposed short circuit breakers to try to restrict the growth of the epidemic. The UK and Scottish governments continued to seek to control the virus through localised restrictions. |
Local restrictions: England and Scotland
England
| 6.121. | As discussed above, local restrictions, in the form of local lockdowns, were implemented across England from 4 July 2020 in accordance with the COVID-19 Contain Framework: A Guide for Local Decision-Makers. Professor Whitty expressed his view that, on balance, local lockdowns “did more good than harm … but it was a very far from perfect tool“.285 Professor Vallance did “not think the local lockdowns worked well“, as people in the areas in which restrictions were proposed could travel with ease to nearby areas that were not subject to restrictions. This, in turn, led to spread of the virus between geographical regions.286 The other problem was that “lower prevalence areas were usually just at an earlier stage of an exponential curve and would quickly ‘catch up’“. He explained:
“Local lockdowns coupled with better use of effective testing, contact tracing and isolation … in lower prevalence areas that were not locked down might have worked.“287 |
| 6.122. | As Mr Hancock commented, this model of localised action had:
“created a complex patchwork of bespoke regulations and guidance which could be perceived as inconsistent, not readily understood by the public and often hard to enforce“.288 His view was that “the local lockdown system, while working, needed to be strengthened and simplified“.289 |
| 6.123. | Leicester, the first place to enter localised restrictions, exemplifies this complexity. From July 2020 – in contrast to the rest of the country – the “protected area” of the City of Leicester and the surrounding area (as defined by a list of postcode districts) was subject to a range of restrictions. Non-essential businesses (with a few exceptions) had to remain closed; most leisure and recreational facilities had to remain closed; food and drink establishments were not permitted to make sales for consumption on the premises; and places of worship could open for individual private prayer only. There were also restrictions on households mixing. After 14 days, two areas were removed from the protected area.290 Six days later, non-essential retail was permitted to reopen.291 After a further eight days, another borough was removed from the protected area, limiting it solely to the City of Leicester.292 Two days later, on 3 August 2020, all Leicester regulations were repealed and replaced by restrictions on gatherings in private dwellings, which were followed by further amendments during August and September 2020.293 |
| 6.124. | The system for local lockdowns in England was subsequently codified into a tiers-based approach. On 21 September 2020, Covid-O endorsed a “three tiered approach, with interventions increasing in severity going up the tiers“.294 This proposal was not, however, implemented until 12 October 2020.295 The three tiers were as follows:
Local areas could “request to go further than this baseline by, for example, imposing restrictions on the leisure, entertainment or personal care sectors“.297 However, they would not be permitted to close non-essential retail, schools or universities. Nor would they be able to reinstate the two-metre social distancing rule.298 |
| 6.125. | On 9 October 2020, the UK government began to negotiate Tier 3 restrictions with the areas with the highest prevalence of Covid-19.299 Mr Hancock considered it to be “vanishingly unlikely” that local leaders would impose the full set of measures within Tier 3.300 In a meeting with Mr Johnson the following day, Mr Hancock voiced his doubt that local leaders would take responsibility for severe economic measures. He argued that the package “needed to be tougher and geographically wider to bring infection rates down“.301 Mr Gove expressed similar concerns.302 |
| 6.126. | Following negotiations with Steve Rotheram, Mayor of the Liverpool City Region from May 2017, Liverpool was immediately placed under Tier 3 restrictions when the system came into effect on 14 October 2020.303 |
| 6.127. | In contrast, discussions concerning Greater Manchester were particularly acrimonious. Andy Burnham, Mayor of Greater Manchester from May 2017, described “2 weeks of meetings and intense disagreement with Ministers“. He made multiple requests for additional funding to support those in the area who were most affected by the measures. Those requests were denied and the UK government unilaterally moved Greater Manchester into Tier 3 on 23 October 2020. Mr Burnham stated:
“In our view, Ministers were asking us to gamble our resident’s [sic] jobs, homes, businesses, and a large chunk of our economy on a strategy that their own experts were telling them might not work.“304 |
| 6.128. | Sir Edward Udny-Lister (later Lord Udny-Lister), Chief Strategic Adviser to the Prime Minister from July 2019 to November 2020 and Chief of Staff to the Prime Minister from November 2020 to February 2021, referred to the protracted nature of the negotiation process. He observed that negotiators:
“had to engage with local political leaders, then local officials and then again with local political leaders in over twenty local authorities“.305 Lord Udny-Lister described the Tier 3 negotiations to the Inquiry as: “tense … the local authorities did not want to close their hospitality industry down. It had only just started to get back on its feet.“306 |
| 6.129. | Negotiations contributed to significant delays in implementation. On 27 October 2020, Professor Van-Tam informed Covid-O that the process of moving areas into Tier 3 was taking too long. Despite Nottingham having been “epidemiologically ready” for Tier 3 for the previous 10 days, the move had not yet been implemented. Given that the number of daily infections was doubling every 10 to 15 days, this delay was “disastrous” in public health terms.307 |
| 6.130. | SAGE was not consulted on the tiers policy before it was implemented, but Professors Vallance and Whitty had repeatedly alerted core decision-makers to its flaws:308
|
| 6.131. | Professor Vallance had “no doubt” that this advice was understood within government.315 In his personal evening notes on 11 October 2020, he recorded his frustration at:
“[b]eing asked to ‘approve the measures knowing that it is not enough’ … This is a massive abrogation of responsibility.“316 |
| 6.132. | Mr Johnson told the Inquiry that, although he could “see the force” of the scientific arguments, he remained of the view that tiering was “worth a try“.317 The UK government’s decision to implement the tier proposals, as drafted by the Covid-19 Taskforce, had gone directly against the advice of its most senior scientific advisers. |
| 6.133. | As predicted, incidence continued to grow rapidly across England.318 On 17 October 2020, Professor Vallance recorded in his contemporaneous evening notes that he had received a WhatsApp message from Mr Cummings “a few days back“, which read:
“This is a shitshow. We should have gone a month ago as we said.“319 |
| 6.134. | On 21 October 2020, SPI-M-O noted that prevalence in most regions of England was now too high for a circuit breaker to be effective.320 By 29 October, Mr Hancock had “come to the view that the tiers system, as introduced, had failed“.321 |
| 6.135. | The tiers framework was an attempt by the UK government to simplify the previous local approach and to find a balance between a full England-wide lockdown and an unconstrained epidemic. However, the system suffered from a number of significant flaws:
|
| 6.136. | SPI-M-O subsequently analysed the impact of the tiers framework on viral transmission in England. It confirmed that Tier 1 measures alone were not sufficient to prevent the epidemic from growing rapidly. If R in a particular area was slightly above 1 and Tier 2 restrictions were implemented, these could “theoretically be just enough” to drive R below 1. If R was 1.1 or greater, the imposition of Tier 2 measures was “barely adequate” to stop epidemic growth and was “unlikely to turn epidemic growth rates negative“. It was unclear whether baseline Tier 3 restrictions alone were sufficient at a regional or national level to reduce R below 1.325 |
| 6.137. | As Professor Whitty summarised, the tiers:
“were often a bit too late, not quite stringent enough to get R below 1, and too geographically circumscribed to have the effect needed“.326 Had the tiers framework been implemented more robustly in early September 2020 – when incidence was lower – it would have stood a greater chance of success. In turn, it might have been possible to avert a second England-wide lockdown. By mid-October 2020, however, it was too late. |
| 6.138. | Mr Johnson told the Inquiry that, with hindsight, he did not think local measures were the correct approach and that restrictions should have been introduced either UK-wide or not at all. He explained that the system involved a myriad of different rules, which people found confusing. He stated: “[I]f I have one ‘takeaway’ to offer from the pandemic, it is that I think the best approach is a UK-wide one.“327 |
Scotland
| 6.139. | In late September 2020, the Scottish Government’s advisers were also considering the introduction of a tiers system. On 27 September, a briefing noted that a ‘levels’ system could reduce the complexity of decision-making and communication. It recommended a five-levels approach – a baseline plus four levels of restrictions.328 |
| 6.140. | On 5 October 2020, the Scottish Government Covid-19 Advisory Group met to discuss proposals for additional measures in the context of rising case and hospitalisation rates.329 As within the UK government, there were concerns about circuit breaker measures, including the absence of an exit strategy that would ensure such circuit breakers were not needed repeatedly:
“Unless something changes we will … simply yo-yo in and out of restrictions. Frequent changing of restrictions is likely to lead to increased public confusion and may burn up public goodwill.“330 |
| 6.141. | The Scottish Cabinet met on 6 and 7 October 2020 to discuss possible new measures, including the possibility of a two-week circuit breaker to stem the escalation of cases.331 The Cabinet noted that, in contrast to the position in March 2020, any measures would need to be considered against “the backdrop of seven months of damage to the economy” and the need to “ensure that non-COVID health harms were also tackled” in accordance with the four harms framework (see Chapter 11: Government decision-making, in Volume II).332 The Cabinet decided to introduce a new package of measures that was “not intended to be seen as a new ‘lockdown’ of the type seen across the UK from March 2020“.333 This included further restrictions on the hospitality sector, but the rules on a maximum of six people from two households being able to meet would continue.334 |
| 6.142. | On 12 October 2020, the Scottish Government announced plans to draw up a tiered restrictions system similar to the one that had been announced for England.335 Ms Sturgeon said that the Scottish Government was seeking to “align as closely as possible with other UK nations on a strategic level“, although she stressed that the ultimate decision would be taken by the Scottish Government.336 |
| 6.143. | On 23 October 2020, Ms Sturgeon unveiled Scotland’s new five-level Covid-19 management system to allow a more flexible response to localised outbreaks. The plan came into effect from 2 November 2020.337 Baseline and Level 1 were akin to “the closest we can get to normality, without a vaccine“; Levels 2 and 3 involved more restrictions “focusing on key areas of risk – broadly, indoor settings where household mixing takes place“; and Level 4 involved “measures close to a return to full lockdown” to prevent overwhelming NHS capacity.338 |
| 6.144. | On 29 October 2020, it was confirmed that North and South Lanarkshire, Dundee and the Central Belt would be placed in Level 3 restrictions, while most of the rest of Scotland would be placed in Level 2. The Highlands, Orkney, Shetland, the Western Isles and Moray, where Covid-19 cases were relatively low, would be placed in Level 1.339 |
| 6.145. | Some local authorities identified practical difficulties arising from the operation of a five-level system in Scotland and a three-tier system in England. Moray Council said:
“Changes of levels and having different levels across LA [local authority] boundaries caused some confusion – as did it being called ‘levels’ in Scotland and ‘tiers’ in England. This caused outbreaks of arguments on our social media channels, which we worked hard to contain as there were often contributors giving conflicting information depending on whether they were personally choosing to follow UKG [UK government] or SG [Scottish Government] guidance.“340 East Lothian Council agreed, stating that the: “confusion arose due to the UK Government and Scottish Government issuing separate Guidance/Regulation and imposing differing COVID-19 Regulations, constraints and effective dates. As a county bordering England, this led to much confusion for local residents, visitors and businesses.“341 |
| 6.146. | Furthermore, individual local authorities identified two broad criticisms of the Scottish Government’s operation of the levels system:
As Angus Council noted: “The main causes of confusion resulted from the council hearing of new rules/ |
Circuit breakers in Wales and Northern Ireland
Wales
| 6.147. | Mr Drakeford told the Inquiry that “things got worse much more quickly in September than we had anticipated“.343 At a review of restrictions on 1 October 2020, Dr Atherton confirmed a significant increase in new cases, with 398 cases reported the previous day.344 However, infection rates in Newport, one of the local health protection areas, were “stabilising“. It was agreed that, from 3 October, single adult households in local health protection areas could form a bubble with another household.345 In advice shared with ministers on 5 October, the Technical Advisory Cell observed that, unless the current measures brought R below 1, it was:
“possible that infection incidence and hospital admissions may exceed scenario planning levels“.346 |
| 6.148. | On 5 October 2020, Felicity Bennée, Co-Chair of the Technical Advisory Group, emailed Mr Drakeford’s office and other Welsh Government officials to:
“suggest that the First Minister may wish to ask CDL [Chancellor of the Duchy of Lancaster] whether they are willing to provide economic support for a firebreak/circuit breaker around half term“.347 |
| 6.149. | Hospital admissions for Covid-19 in Wales soon doubled in a two-week period and, on 9 October 2020, the Technical Advisory Cell advised that there remained exponential growth.348 As Mr Drakeford explained:
“By the time we get halfway through October, though, we have got local lockdowns over almost half or more of Wales, and every week we’re having to add more local areas to – in other words, it just hasn’t worked.“349 |
| 6.150. | Specific modelling for a two or three-week firebreak was not sought until 11 October 2020.350 On 12 October, Public Health Wales advised that further restrictions should be implemented in the next two weeks and should last for at least three weeks.351 A combination of at least three restrictions was needed to bring R below 1, of which a short lockdown was one possibility. |
| 6.151. | Ms Bennée emailed a number of officials in the Welsh Government, stating that, while a short firebreak would be expensive, it would be “far cheaper than going to meltdown and needing to do it for 3 months. Cost is relative!“352 |
| 6.152. | Dr Atherton also outlined to Welsh ministers the growing view of the Chief Medical Officers for the four nations that “some sort of circuit breaker will be needed“.353 Mr Drakeford summarised the main options: strengthening local measures; introducing Wales-wide measures; or a short lockdown. Mr Drakeford confirmed that the aim of circuit breaker restrictions would be to “buy time and prevent the overwhelming of the Health Service“. Subsequently, a firebreak implementation group of senior policy officials across the Welsh Government was convened.354 |
| 6.153. | Mr Drakeford also repeated his request to Mr Johnson for an urgent COBR meeting on circuit breaker measures.355 Mr Johnson responded on 15 October 2020, stating that he would ask Mr Gove to “urgently convene a meeting” with the devolved administrations. However, by then, the position in Wales had already escalated.356 Within the previous 24 hours, 90 people had been admitted to hospital and all 150 intensive care unit beds in Wales were occupied.357 |
| 6.154. | Dr Rob Orford, Chief Scientific Adviser (Health) for Wales from January 2017, emailed Mr Drakeford, Dr Atherton and Dr Andrew Goodall (Director General of Health and Social Services in the Welsh Government and Chief Executive of NHS Wales from June 2014 to November 2021) on 15 October 2020. He attached modelling which illustrated that acting by the end of the week, and for three weeks rather than two, would have a greater impact in reducing deaths.358 |
| 6.155. | The Welsh Cabinet met later that day. They discussed a paper that concluded: “[T]he balance of contributions to this paper appear to prioritise a shorter firebreak, even if this meant more widespread closures.“359 The strategy outlined was:
“1. A time-limited firebreak to attempt to bring Rt below 1 and address capacity constraints in healthcare infrastructure. 2. A subsequent revision of national rules and encouraging behaviour change in order to maintain Rt at around 1.1 over the winter.“360 |
| 6.156. | The timing of the firebreak to include the school half-term holidays was intended to mitigate the impact on education and childcare.361 The Welsh Cabinet therefore agreed in principle to introduce a firebreak from 23 October to 9 November 2020, subject to discussion the following week “to allow further work to take place“.362 |
| 6.157. | On 16 October 2020, Mr Drakeford informed Mr Johnson that the Welsh Government had begun to consider the imposition of a firebreak in Wales, to start on 23 October.363 That same day, regulations came into force preventing people living in areas of high prevalence in the rest of the UK from travelling to Wales.364 Mr Drakeford also wrote to Mr Sunak asking the UK government to bring forward the operational date of an expanded Job Support Scheme (which was due to replace the Coronavirus Job Retention Scheme, known as ‘furlough’) to 23 October from 1 November.365 |
| 6.158. | On 18 October 2020, the Welsh Cabinet discussed the Technical Advisory Cell’s advice, which recommended a two to three-week firebreak consistent with the earlier SAGE advice of 21 September.366 Wales was in “material breach” of several of the triggers that might require further action, including intensive care unit occupancy.367 The Technical Advisory Cell recommended a two-phase approach: (i) a short firebreak; and (ii) a new, simpler, Wales-wide approach to restrictions following the firebreak. Economic advice to Cabinet was that the loss from closing businesses was estimated at approximately £100 million a week, and that a firebreak might reduce GDP by around 5%.368 Ministers were advised through the Technical Advisory Cell:
“[T]here is a reasonable likelihood that if we do not act now, we will need to take further, more expensive and longer action in the future to achieve a similar reduction.“369 |
| 6.159. | By 19 October 2020, the rate of infection in people aged over 60 was close to the rates seen in March.370 That day, the Welsh Cabinet formally agreed to the implementation of the firebreak from 23 October to 9 November 2020.371 The firebreak reintroduced the requirement to stay at home, and the closure of non-essential retail, hospitality venues, close-contact services (such as hairdressers), hotels and holiday accommodation. It also reiterated that people should work from home wherever possible. The first week of the firebreak covered the school half-term holidays for most schools in Wales, with schools in three local authorities open for both the first and second weeks.372 Primary, special and secondary schools (for Years 7 and 8) would reopen as originally planned in the second week. |
| 6.160. | Mr Sunak confirmed later that day that, for operational reasons, the Job Support Scheme could not be brought forward, but that the existing Coronavirus Job Retention Scheme would remain in place until 31 October 2020.373 |
| 6.161. | A number of Welsh Government witnesses, including Mr Drakeford, said that the provision of funding from the UK government had affected the Welsh Government’s decisions on the timing and length of the firebreak.374 On 9 October 2020, Mr Drakeford had been informed of the expanded Job Support Scheme and its commencement date of 1 November 2020. However, he did not raise the question of additional economic support for a Wales-only lockdown, and it was not until 16 October that Mr Drakeford asked Mr Sunak to bring forward the Job Support Scheme. Mr Sunak had not replied to Mr Drakeford’s request by the time the Welsh Cabinet formally agreed to the firebreak’s timing and duration on 19 October. |
| 6.162. | The Welsh Government had to weigh up a number of factors in determining the timing and length of the firebreak. A longer, three-week firebreak, as advised, would have reduced transmission further and put Wales in a better position in December 2020.375 Opting for a shorter firebreak was, however, within the reasonable range of responses from the Welsh Government. The Inquiry does not consider that the Welsh Government’s decisions on timing or length were in fact impacted by UK government funding decisions. |
| 6.163. | Any lockdown or circuit breaker, even a local one, has substantial repercussions. Opinions vary as to whether they are effective in the long term. As Mr Kilpatrick explained:
“Ministers were acutely aware of the range of social and economic impacts that a return to a strict universal lockdown across Wales would bring … It was considered that dealing with outbreaks at a local level would help to reduce the risk of individuals contracting the virus, while limiting the number of people subject to restrictions.“376 |
| 6.164. | Mr Drakeford reflected in his evidence to the Inquiry that local restrictions had been a “failed experiment“.377 It was reasonable for the Welsh Government to try to contain the virus with local measures targeted at those areas that were experiencing a steep rise in infections, while other areas remained stable. This was a “textbook public health response to an outbreak“.378 However, more work should have been undertaken over the summer months to provide a clear process for the timely implementation of local restrictions. By the time of the firebreak, “more of Wales geographically was in a state of local intervention than not“.379 |
| 6.165. | There was also a lack of timely planning for the firebreak in Wales. The Welsh Government had received advice from SAGE on 17 and 21 September 2020 and, by 5 October 2020, Technical Advisory Cell advice and Ms Bennée’s warnings. However, it did not seek specific modelling until 11 October, with work on planning the firebreak beginning on 12 October to then be implemented on 23 October.380 Both modelling and planning should have been in train prior to 12 October. The Inquiry appreciates that the decision to impose the firebreak over the school half-term holidays was intended to mitigate the length of time lost in face-to-face education. However, the same aim would have been achieved had it been imposed a week earlier, with half-term holidays for most schools then falling in the second and not the first week of the firebreak. |
| 6.166. | The post-firebreak regime was discussed by the Welsh Cabinet on 27 and 29 October 2020.381 At the time, there was a worsening situation in Wales, with over 1,000 new cases each day of the previous week. Dr Atherton advised that it would take “some time” to see the impact of the firebreak, and he felt it was premature at that stage to make decisions on post-firebreak restrictions.382 Ministers agreed some specific measures, such as restrictions on indoor hospitality, but other areas, such as household mixing, would require further advice. Areas of Wales were deteriorating quicker than expected.383 |
| 6.167. | There were concerns about the ability of Test, Trace, Protect to cope and about the firebreak being for the minimum recommended period. Dr Atherton advised a gradual easing of restrictions. Nonetheless, Mr Drakeford made a public statement in the Welsh Parliament on 3 November 2020 announcing the restrictions that would apply on an all-Wales basis after the firebreak.384 Among other measures, schools, non-essential retail, leisure facilities for up to 60 people and hospitality settings would reopen. Groups of up to four people (from four different households) could meet, subject to limitations. Organised activities of up to 15 people indoors and 30 people outdoors would be permitted. Households could form an ‘extended household’ with one other household. Travel to and from England – which was, by this point, in lockdown – was prohibited and restrictions were placed on people entering and leaving Wales, given the high rates of Covid-19 present in Wales. |
| 6.168. | The firebreak ended on 12 November 2020. By 20 November, the Technical Advisory Cell advised that, while cases had decreased following the firebreak, “pushing back the epidemic by around 3 weeks“, it was “likely” that its positive effects had largely been lost as cases were beginning to increase.385 The Welsh Cabinet noted on 23 November 2020 that “there had been an increase in the spread of the virus amongst young people“.386 Advice on NHS capacity discussed by ministers on 24 November suggested that, unless further measures were implemented, demand on the NHS would rise unsustainably ahead of the Christmas period.387 On 25 November, Dr Atherton advised ministers that case rates were increasing and the situation was “fragile“.388 Dr Orford advised that “early mixing data suggests R is now at 1.4” and there was a risk that the prevalence of the virus might double over Christmas. There was the potential for 1,600 additional avoidable deaths without further interventions.389 The Technical Advisory Cell reiterated:
“[I]t is better to intervene early than late; short and sharp interventions work; compliance wanes over time; and firebreaks and harder restrictions (e.g. tier 3+) can reduce levels of transmission in the community. Rules must be simple, understandable and achievable – with an agreed beginning and end.“390 |
| 6.169. | The Welsh Cabinet met on 26, 27 and 29 November 2020 to consider whether further restrictions should be implemented to “guarantee that families could meet for up to five days over the Christmas period“.391 A Cabinet paper outlined:
“Evidence from SAGE has suggested that Level 3 in Scotland could be effective at preventing growth of coronavirus and that Tier 3 (very high alert level) in England appears to have had a measurable effect in most areas.“392 The Cabinet agreed to adopt a tiered system of restrictions on an all-Wales basis to commence on 4 December 2020, based initially on the interventions for Level 3 in Scotland. Pubs, bars, cafes and restaurants would be required to close at 18:00 and would not be permitted to sell alcohol.393 |
| 6.170. | However, by 2 December 2020, the Technical Advisory Cell confirmed that both case numbers and hospital admissions were “nearly reaching levels seen at the beginning of the firebreak“.394 Dr Orford told the Inquiry that “‘the science’ did not align with important decisions“, with the Technical Advisory Cell and Technical Advisory Group advocating for control measures that would keep infection rates lower – advice that he said was not followed.395 The Inquiry understands the need to reopen the economy but it finds that the decision to allow up to four people from four different households to meet was misguided. The Welsh Cabinet could have reopened hospitality settings and restricted this to members of the same extended household only, or to fewer than four different households, thereby reducing household mixing. The Welsh Government relaxed restrictions too quickly following the firebreak.396 This quickly led to the benefits of the firebreak being lost and to the need for the reintroduction of stricter restrictions at the beginning of December. |
| 6.171. | From August to December 2020, Wales had the highest age-standardised mortality rate of the four nations.397 It is likely that a combination of failed local restrictions, a firebreak that was too late and the decision to relax measures too quickly all contributed to the higher mortality rate.398 |
Northern Ireland
| 6.172. | At a meeting of the Northern Ireland Executive on 1 October 2020, Ms Foster advised that a point had been reached to consider and implement a “reset” of the approach to the management of the pandemic.399 This, at least in part, seems to have emerged in response to concerns about compliance.400 By this point, the number of Covid-19 hospital patients in Northern Ireland had risen to close to 25% of the peak levels seen during the first wave. The Executive Committee agreed to introduce additional restrictions for Derry City and Strabane Local Government District Area.401 |
Figure 18: Increase in infections in Northern Ireland from 1 September to 1 October 2020
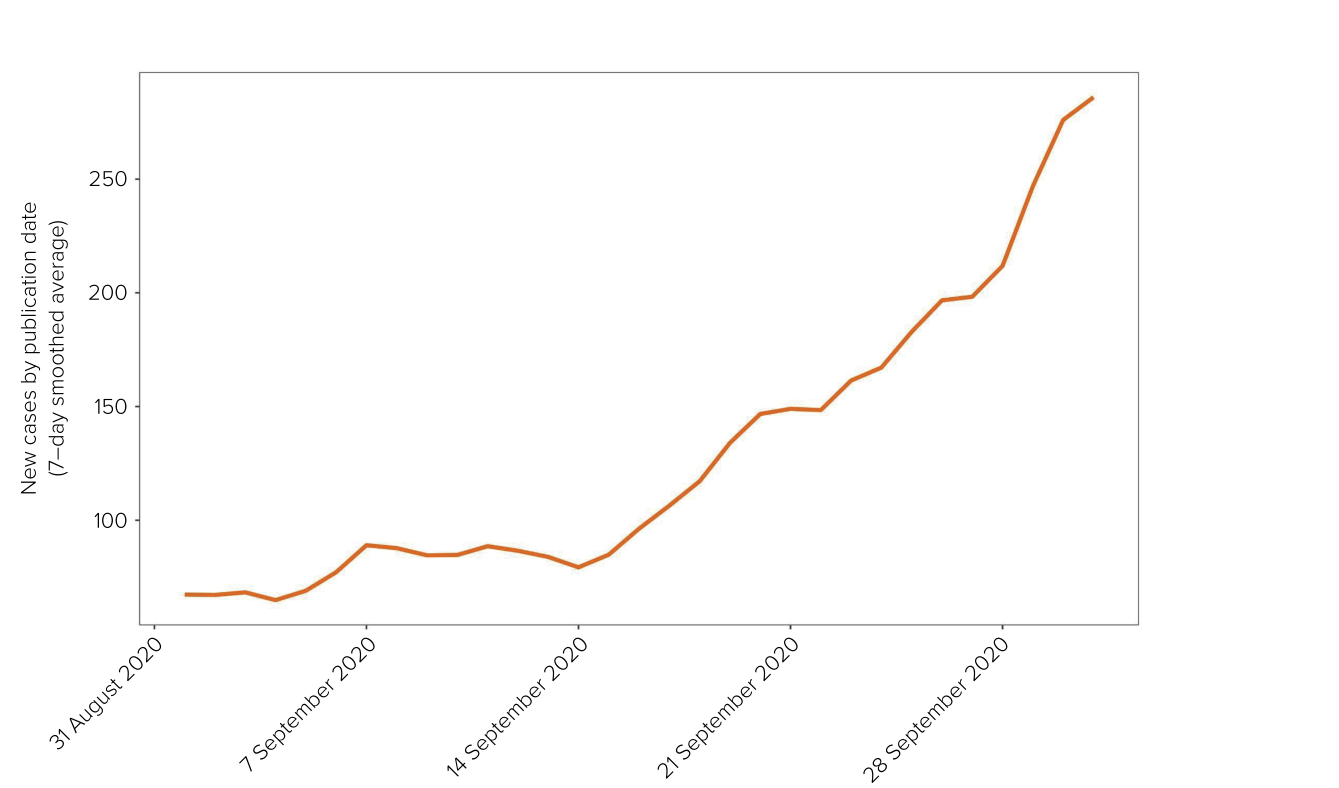
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 6.173. | Baroness Foster told the Inquiry that the reset was intended “to try to get the public to sit up and take notice of the seriousness of the situation“.402 It was:
“critical to get a clear, fresh message across to the public about the need for compliance with the restrictions in place, in order, hopefully, to avoid the need for more stringent restrictions. The reset was primarily around renewed messaging … but there was also emphasis placed on ensuring that the Regulations were being properly enforced.“403 In practical terms, the reset focused on the decision-making process and greater transparency in communications.404 Baroness Foster acknowledged: “[I]t was not as successful as we might have hoped as further restrictions did become necessary.“405 In short, the reset did not amount to the Executive Committee getting a grip on the situation that was fast developing. |
| 6.174. | In a report dated 8 October 2020, Professor Young set out the pressures that were already facing the health and social care system in Northern Ireland:
“Most hospitals are running at more than 85% capacity, with some over 90%. There are already trolley waits … and ambulances queuing outside. This level of pressure does not usually manifest until later in the year. There is therefore a concern around how the system will deal with rising pressures over the winter period alongside increasing numbers of Covid+ patients.“406 |
| 6.175. | Professor McBride warned the Executive Committee that day that he had “never [been] more concerned” and that there should be “intervention now to avoid situation in 2/3 weeks“.407 In the same meeting, the situation was characterised as “apocalyptic“.408 The Executive Committee ultimately agreed that ministers would, over the coming days, meet individually or in small groups with Robin Swann MLA (Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024) and Professors McBride and Young “to consider and discuss … future measures“.409 |
| 6.176. | On 11 October 2020, Professor McBride advised Ms Foster and Ms O’Neill that Northern Ireland was 10 days away from the health service being overwhelmed. He stated that they were “[r]apidly running out of time“.410 An email recorded his view that the situation was much more serious than in March 2020 and “beyond discussion and nuance“.411 Professor Young warned that “every day makes a real difference“.412 Mr Swann had indicated that a six-week intervention was required.413 |
| 6.177. | By 12 October 2020, Northern Ireland had a higher level of incidence than anywhere in the rest of Europe apart from the Czech Republic.414 Covid-19 had “reached a phase of exponential growth” in Northern Ireland.415 |
| 6.178. | An Executive Committee meeting the following day considered the further progression and current state of the pandemic, noting the following:
|
| 6.179. | The Executive Committee agreed to revoke the specific restrictions on Derry City and Strabane Local Government District Area. It also agreed to impose a four-week period of interventions across Northern Ireland, to take effect from 16 October 2020 and to expire at midnight on 13 November 2020.423 These restrictions involved, for example, the closure of the hospitality sector, apart from takeaway and delivery of food, but did not entail the closure of retail or the closure of schools (save for the extended school break).424 The half-term holiday for schools was also extended from 19 to 30 October, with schools reopening on 2 November.425 |
| 6.180. | Ms O’Neill emphasised that this was a compromise. Her preference was that schools would close for a four-week period.426 Baroness Foster explained that “six weeks was simply considered too long for a circuit breaker lockdown at that time“.427 The scientific advice at this time was that interventions were required in order to preserve hospital capacity, failing which there would be an impact on non-Covid-19 hospital beds and patients.428 Baroness Foster said:
“[W]e wouldn’t just look at the health advice, we would take into consideration other issues as well, and that’s what we were trying to do.“429 |
| 6.181. | By 15 October 2020, on the eve of the circuit breaker, R was 1.6, the Nightingale facility at Belfast City Hospital was in operation and there were confirmed outbreaks in care homes.430 By 29 October, hospital inpatient numbers in Northern Ireland had reached a higher level than in the peak of the first wave of the pandemic.431 |
| 6.182. | During the initial two weeks of the restrictions, R was reduced to slightly above 0.7.432 However, the value of R was expected to increase slightly upon the return of schools after the extended half-term holidays.433 |
| 6.183. | On 5 November 2020, the Department of Health (Northern Ireland) advised the Executive Committee to extend restrictions for a further two weeks after 12 November, to avoid the health service becoming overwhelmed and potentially to avoid the need for further intervention before Christmas.434 This was due to be discussed at a meeting of the Executive Committee the same day, but substantive discussion and decision-making were deferred as a result of leaking and concern about the public response.435 |
| 6.184. | The Executive Committee met again on 9 November 2020 to make a decision on the proposed two-week extension. By this time, the numbers in intensive care units were the “highest figures yet“. Numbers in hospitals were not decreasing, and capacity was currently near 100% and had been exceeded on a number of recent days.436 Professor Young warned:
“Deaths will continue to increase in January and numbers will be significantly greater without further intervention.“437 |
| 6.185. | Despite the seriousness of the position, Baroness Foster told the Inquiry:
“My DUP [Democratic Unionist Party] colleagues felt this was a breach of trust, and that extending the circuit breaker would not only be damaging for businesses (particularly for small business such as close contact services), and those on low incomes, but would also erode public confidence in the Executive.“438 |
| 6.186. | This Executive Committee meeting was adjourned and reconvened several times over the next few days, and involved two cross-community votes on 9 and 11 November 2020. The deployment of the cross-community vote mechanism (see Chapter 11: Government decision-making, in Volume II) was instigated by Ms Foster, but it was Edwin Poots MLA (Minister for Agriculture, Environment and Rural Affairs in Northern Ireland from January 2020 to October 2022) and Peter Weir (later Lord Weir of Ballyholme), Minister for Education in Northern Ireland from May 2016 to March 2017 and from January 2020 to June 2021, who ultimately called the votes.439 Ministers also discussed a compromise to extend the restrictions by one week to avoid “everything falling” the next day.440 |
| 6.187. | The content of the discussions was leaked throughout. This was described by a number of witnesses as marking a low point in politics in Northern Ireland – not just during the pandemic but generally.441 |
| 6.188. | The use of the cross-community vote mechanism in this context was inappropriate. The Inquiry is not persuaded by the suggestion that its deployment was intended to achieve consensus.442 Those responsible for deploying it appear to have politicised the debate. There was no minority issue at stake. There were people, across the community, who would have been better protected by timely and measured interventions by the government of Northern Ireland. This is discussed further in Chapter 11: Government decision-making, in Volume II. |
| 6.189. | On 12 November 2020, the Executive Committee agreed – albeit not unanimously – to a number of easements, including the reopening of close-contact services by appointment and the reopening of some hospitality settings with restricted opening hours from 20 November. The remaining restrictions were extended until 26 November, with all settings able to reopen from 27 November.443 |
| 6.190. | The Executive Committee met again on 19 November 2020, with a number of services being due to reopen the following day. Ministers were made aware that the numbers of cases, admissions, hospital inpatients and deaths, as well as intensive care unit occupancy rates, remained higher than during the peak of the first wave. They were also informed that the planned relaxations would result in R rising significantly above 1.444 Mr Swann did not offer any recommendations, as he was:
“of the opinion that specific recommendations would again result in a cross-community vote without proper consideration being given to the contents of the paper, such was the political tension at that time“.445 Mr Swann did advocate for a further two weeks of restrictions, “to protect hospitals” and “to keep [the] health service on its feet“.446 The Executive Committee agreed to introduce restrictions (albeit that schools and childcare were to remain open) from 27 November for a period of two weeks, following a one-week relaxation.447 Close-contact services, hospitality settings, pubs and bars therefore reopened with mitigations in the intervening days. Professor Young told the Inquiry that there was a correlation between this relaxation and a 25% increase in cases.448 |
| 6.191. | As a result of the decision on 12 November 2020, there was a week-long extension to the four-week period of restrictions, with a range of restrictions due to be lifted.449 In effect, unlike in the period leading up to the first UK-wide lockdown in March 2020, the Executive Committee had greater control over the response to the pandemic in Northern Ireland. It had agency over its response and could use the knowledge it had acquired to manage rising transmission rates after July 2020. It was clearly warned that there would be a second wave once restrictions were lifted, and it was given clear advice that the best chance of meaningful intervention was an initial response by way of longer and more strenuous restrictions. However, the advice given for the purposes of the meeting on 13 October 2020 (namely that there should be restrictions from 16 October for a period of six weeks) was rejected, albeit that some ministers favoured more severe restrictions during this period. |
| 6.192. | On 19 November 2020, the Northern Ireland Executive subsequently agreed to introduce a two-week circuit breaker, but this was not to come into effect until 27 November.450 There was, therefore, a week-long period during this precarious stage of the pandemic when restrictions were relaxed in advance of the circuit breaker. By 8 December 2020, it was understood that the two-week circuit breaker had not had the impact hoped for, but, nonetheless, restrictions were eased in the two weeks leading up to Christmas.451 It is difficult to discern any rationale for the approach taken. As discussed in Chapter 7: Further lockdowns, in this volume, the death rate reached its peak in Northern Ireland in January 2021. The starting point for that trajectory was this period from October 2020 onwards. |
A second lockdown in England
| 6.193. | Covid-19 infections continued to rise in every region of England. The Office for National Statistics estimated that an average of 568,100 people had the virus by 28 October 2020, compared with 336,500 people from 2 to 8 October.452 |
| 6.194. | On 25 October 2020, Mr Johnson held a strategy session. Professors Vallance and Whitty were present, along with various 10 Downing Street officials. The Covid-19 Taskforce advised that hospital admissions and deaths were beginning to rise in low prevalence areas of England. Over the previous fortnight, the number of patients in hospital had approximately doubled in all regions.453 The current approach was “highly unlikely” to drive R below 1 across England.454 |
| 6.195. | Mr Johnson was recorded as asserting that he was “not going to be stampeded into a national lockdown“.455 He remained “deeply sceptical” about the need for this intervention, which he said the public would regard as a “massive failure“.456 In his evening notes, Professor Vallance recorded that, in the meeting, Mr Johnson had begun to “argue for letting it all rip“, while others had advocated that the government’s primary obligation was to save lives.457 Professor Vallance also recorded that Mr Johnson had acknowledged that the situation was a “total shambles“.458 He was told that, if he went down the route of “letting it go“, he needed to tell the public that he was “going to allow people to die“.459 |
| 6.196. | A note submitted to Mr Johnson on 28 October 2020 warned that the situation was deteriorating. Although the north of England continued to be the most heavily affected by Covid-19, the infection rate was growing in every region of England and the wave was “sweeping south“.460 Mr Johnson set out his thoughts and concerns on the paper with a number of questions for his advisers. He questioned, among other issues, the assumption underpinning the advice that things would get better in the spring of 2021; the impacts of restrictions on mental health and the economy; what would be achieved by “smashing up the economy” without knowing how many times restrictions would need to be implemented; the utility of the test and trace and tiers systems; and whether localised or nationwide restrictions were necessary.461 |
| 6.197. | On 29 October 2020, Covid-O noted that hospital occupancy would surpass the peak of the first wave by about 11 November 2020.462 Professor Van-Tam remarked that England was “now in a very bad place and would be in an extremely bad place by the end of November“. He stressed that the UK government “had to do more“.463 |
| 6.198. | On 30 October 2020, the Covid-19 Taskforce set out the deteriorating situation at a meeting of Covid-S.464 Later that day, the taskforce informed Covid-O that R was growing as quickly – if not more so – in areas with lower case rates. The taskforce proposed a four-week nationwide intervention, with a regional approach to de-escalation.465 The decision was taken to announce a second England-wide lockdown. |
| 6.199. | At a UK Cabinet meeting the following day, Mr Sunak warned that this would cause “significant economic damage“, but agreed that it was a “reasonable and right decision to do these things to save lives and the NHS“.466 Mr Johnson had earlier commissioned the Covid-19 Taskforce and the Treasury to advise on the economic impact of the different options.467 |
| 6.200. | That evening, 31 October 2020, Mr Johnson publicly announced that England would enter a second lockdown on 5 November 2020. He emphasised the importance of not “overrunning” the NHS.468 Unlike the first lockdown, schools and universities would remain open, with an emphasis on people being encouraged to go to work if they could not work from home. This lockdown was limited to a four-week period ending on 2 December 2020, after which the UK would return to a tiered system of local restrictions.469 |
| 6.201. | Mr Johnson told the Inquiry:
“It was clear at this stage that local measures were insufficient and that we had to consider measures at a national level, rather than engaging with local leaders.“470 The dire epidemiological situation in England meant that policy-makers had “run out of road“.471 |
| 6.202. | Mr Case described 31 October 2020 as “a very dark day“.472 He shared his frustrations about the decision-making process with Helen MacNamara, Deputy Cabinet Secretary from January 2019 to February 2021:
“It is horrid. We are back here because the state has failed. We have some massive questions to ask ourselves.“473 Mr Johnson explained to the Inquiry: “[W]e wanted to try the tiered approach, we wanted to try the local approach. That was gradually running out of road and we had to go for national measures. But I always knew that we were – that was on the cards.“474 |
| 6.203. | The UK government immediately began to consider potential exit strategies from the second lockdown. On 3 November 2020, senior officials in the Department of Health and Social Care met to discuss potential measures. Professor Whitty advised that the exit strategy should be informed by data on the effectiveness of the tiers system, which would not be available for several weeks.475 |
| 6.204. | However, at a UK Cabinet meeting, Mr Johnson said that 2 December 2020 was “a hard deadline” to end the lockdown in England. The end of lockdown was to be date driven and not data driven. The UK government “would use every second to get mass testing working to avoid further lockdowns and find a way out of coronavirus“. Mr Johnson emphasised that he “did not want to go back to a set of national measures after 2 December, at almost any cost“.476 |
| 6.205. | SPI-M-O advised the same day that, if England returned to the original tiering system in December 2020, the epidemic would continue to grow and a third lockdown might be needed in January 2021.477 As discussed in Chapter 7: Further lockdowns, in this volume, this was prophetic. |
| 6.206. | On 17 November 2020, Covid-O confirmed that England would exit the lockdown on 2 December 2020. The Covid-19 Taskforce proposed to strengthen the existing tiers framework by:
This would be a “standardised tier, imposed rather than negotiated, to ensure optimal effect and rapid deployment“.478 Professor Vallance informed Covid-O that Tier 1 had done nothing to contain the virus, even in areas with low prevalence. For this reason, any area in Tier 1 would be likely to move into Tier 2 immediately. He advised that the UK government should wait for more data about the impact of the lockdown before making a final decision, so as to minimise the chance of unnecessary harm.479 |
| 6.207. | On 19 November 2020, SAGE advised that the relaxation of restrictions over the festive period carried a “significant risk of increased transmission and increased prevalence, potentially by a large amount“. Keeping prevalence low before the festive season would reduce transmission when measures were eased.480 |
| 6.208. | On 22 November 2020, the UK Cabinet approved the return to a localised tiers system, describing it as a “sensible and balanced approach“.481 The COVID-19 Winter Plan (published the following day) permitted the opening of non-essential retail, personal care services, indoor leisure settings and places of worship – as well as schools, colleges, universities and childcare facilities – in all three tiers. Everyone was to work from home where possible. Entertainment venues, hotels and other accommodation could open in Tiers 1 and 2, and up to 15 guests would be permitted at weddings, civil partnerships, wedding receptions and wakes. Up to 30 people were able to attend funerals.482 |
| 6.209. | By 25 November 2020, the epidemic was shrinking in the north-west, north-east and Yorkshire. Only two NHS England regions (London and the South East) had R estimates at or above 1.483 The purpose of the second lockdown was to bring R below 1 and thereby reduce the pressure on the NHS. As Professors Vallance, Whitty and Van-Tam all agreed, this objective was achieved.484 |
Alternatives to the second lockdown
| 6.210. | The Great Barrington Declaration (published on 4 October 2020) was an open letter authored and signed by three public health experts, including Professor Gupta. The declaration essentially called for the lifting of lockdown restrictions, so as to allow infection to spread through the community and thereby lead to population immunity (or ‘herd immunity’). In tandem, focused measures for the protection of vulnerable people would be put in place. It stated:
“As immunity builds in the population, the risk of infection to all – including the vulnerable – falls. We know that all populations will eventually reach herd immunity – i.e. the point at which the rate of new infections is stable – and that this can be assisted by (but is not dependent upon) a vaccine. Our goal should therefore be to minimise mortality and social harm until we reach herd immunity.“485 The declaration endorsed the “focused protection” approach that Professor Gupta had described previously in her arguments to Mr Johnson. It suggested that such a strategy would: “allow those who are at minimal risk of death to live their lives normally to build up immunity to the virus through natural infection, while better protecting those who are at highest risk“.486 |
| 6.211. | The open letter was intended for a global audience and was not specific to the UK. It did, however, provide an alternative approach for the UK government to consider. As set out in Chapter 9: Scientific and technical advice, in Volume II, it will always be important for decision-makers to have access to alternative perspectives and advice. |
| 6.212. | Professor Whitty, however, considered the Great Barrington school of thought to be “scientifically weak, operationally impractical and ethically difficult“.487 He described it as “flawed at multiple levels“.488 |
| 6.213. | The “focused protection” approach chimed with Mr Johnson’s wish to pursue population segmentation. However, this approach was unlikely to have been a viable strategy for the UK government for a number of reasons:
|
The second lockdown decision-making process in England
| 6.214. | As in March 2020, events in Europe in September and October 2020 provided an early warning of what was to come. Moreover, in the autumn of 2020, the UK was no longer facing an acute crisis. In contrast to the initial months of the pandemic, when decision-makers were “building the train tracks as the train was moving“, they now had the benefit of experience.493 The first wave had demonstrated the need to implement extensive interventions as soon as it became clear that they were required. As Professor Vallance explained, it was generally understood that it was necessary to “put in place measures in advance (the ‘rules of the road’) to allow a quicker implementation of interventions when needed“.494 |
| 6.215. | However, the lessons from the failure in March 2020 to act quickly enough were not learned.495 This failure was appreciated by advisers. Mr Cain explained that most of the advisory team in 10 Downing Street “knew” by early September 2020 that a second lockdown was “an inevitability“:496
“[B]y the time we moved into this later period, I think the rump of Number 10 felt that, okay, we’ve learned all these lessons from the first period of lockdown, why are we now trying to ignore them again and repeat the exact same mistakes.“497 |
| 6.216. | As Mr Hancock rightly observed, there were “no excuses second time round“.498 Professor Edmunds concluded:
“The failure to act quickly to control this wave was not because of a lack of situational awareness or knowledge of how to control it. We let this second wave happen.“499 |
| 6.217. | Professor McLean described this as the “worst period” of the pandemic for this reason:
“We could see what was coming and could not understand why the government did not act upon the science advice by introducing effective interventions.“500 |
| 6.218. | The scientific advice was clear. By late September 2020, scientific advisers to the UK government had firmly advised that a circuit breaker was required. Hospitals faced being overwhelmed within weeks, with the numbers of infections, hospitalisations and deaths potentially surpassing the peak of the first wave by early November 2020. A “quick and hard” response was more effective than relying on softer measures and waiting for infection rates, hospital occupancy and death rates to rise. |
| 6.219. | However, the UK government resisted the expert advice of SAGE, SPI-M-O, its Chief Scientific Adviser, the Chief Medical Officer and other scientific advisers. Instead, it relied on a series of milder interventions that lacked scientific support and were unlikely to be effective, even if they had some slowing effect on the spread of the virus. Indeed, on 15 October 2020, a social contact study found that the impact of the rule of six, encouragement to work from home, the 22:00 curfew on hospitality settings and the imposition of local restrictions was limited.501 |
| 6.220. | The tiers system failed and, in doing so, led inexorably to the need for a further lockdown. Professor Whitty characterised the UK government’s response as:
“bunny-hopping … we would accelerate into a bend unnecessarily and then have to slam on the brakes“.502 |
| 6.221. | The decision to introduce a second lockdown was taken more than six weeks after SAGE had first advised in favour of a circuit breaker. There was a further delay of five days between the decision being made to impose a lockdown and it being given full legal effect. Unlike the circuit breakers in Wales and Northern Ireland, the second England-wide lockdown was not timed to coincide with the school half-term holidays. Schools did, however, remain open. |
| 6.222. | Some of those around Mr Johnson attributed a failure to act earlier to his inadequate leadership. Throughout September and October 2020, Mr Johnson continuously vacillated between policy options. The rule of six was described by Mr Cummings as:
“the product of the chaos around the PM at the time … it seemed the only practical way to get him to agree that was simple enough he might stick to for more than 5 minutes“.503 (emphasis in original) |
| 6.223. | Two days after deciding on the rule of six, Mr Johnson was described in WhatsApp messages as being “in full trolley mode” (see Chapter 11: Government decision-making, in Volume II). Mr Case noted: “Spectacular today. We want to open up the economy ASAP, forget the bloody virus.“504 Similarly, in October 2020, Mr Johnson stated that he had:
“been slightly rocked by some of the data on Covid fatalities. The median age is 82 – 81 for men 85 for women. That is above life expectancy. So get Covid and live longer … it shows we don’t go for nationwide lockdown.“505 |
| 6.224. | In his evening notes following a meeting on 25 October 2020, Professor Vallance observed that Mr Johnson had begun:
“to argue for letting it all rip. Saying yes, there will be more casualties but so be it – ‘they have had a good innings’ … PM then back on to ‘Most people who die have reached their time anyway’ … This all feels like a complete lack of leadership.“506 |
| 6.225. | The following day, Professor Vallance recorded in his evening notes that Mr Johnson was in a:
“different mood … ‘terrible, terrible, terrible numbers’ … says ‘we need to do local lockdowns fast, foot to the throttle, accelerate, we need action.’ He is inconsistent.“507 (emphasis in original) |
| 6.226. | In his evidence to the Inquiry, Mr Johnson stated that Professor Vallance’s notes reflected instead:
“the deep anxiety of a group of people doing their level best who cannot see an easy solution and are naturally self-critical and critical of others“.508 |
| 6.227. | Mr Johnson’s evident reluctance to impose another lockdown, accompanied by his wish to explore all other solutions first, was understandable. He was rightly concerned about the economic and societal harm that would ensue. However, this meant that the opportunity to regain control over transmission rates when incidence of the virus was lower was lost. |
| 6.228. | The decision-making process was made more difficult by a lack of alignment within the UK government. As case numbers climbed, competing voices clamoured to be heard. Some were calling for the UK to relax its response, while others were advocating a more stringent approach to the crisis.509 The Department of Health and Social Care was primarily motivated by the need to mitigate the public health effects of Covid-19, whereas the Treasury was driven by its concern about the economic impact of restrictions.510 While these differing priorities were to be expected, the “tug-of-war” and jostling for influence undoubtedly placed Mr Johnson in a conflicted position.511 Professor Vallance’s evening notes provide an insight into the debilitating effect of these pressures on decision-making:
“What [Mr Johnson] wants to achieve is a series of mutually incompatible options … he owns the reality for a day and then is buffeted by a discussion with [Mr Sunak].”512 |
| 6.229. | There was also growing resistance in the media and in the UK Parliament to the prospect of a second England-wide lockdown, or indeed any form of circuit breaker.513 Mr Cain said that Mr Johnson was the “focus of a robust campaign from within his own base” and the “Tory backbenches“, adding: “The term ‘lockdown’ had become political.“514 That there was opposition to a lockdown is not at all surprising, given the very significant social, economic and educational damage of the first lockdown. |
| 6.230. | It is clear that Mr Johnson felt he was being backed into a corner. Mr Cummings described Mr Johnson as “enraged“. Mr Cummings alleged that, on 30 October 2020, Mr Johnson said:
“‘[N]o more fucking lockdowns – let the bodies pile high in their thousands’ … my impression at the time was that it was a mix of rage, frustration and fear.“515 Lord Udny-Lister also recalled Mr Johnson making this remark, possibly in September 2020, although he was uncertain as to when it occurred or to whom it was directed.516 Mr Johnson denied saying these words at any time. His position was “that we had to save human life at all ages, and that was the objective of the strategy“.517 |
| 6.231. | A number of scientific experts stated that, had a circuit breaker been utilised in September 2020, the second England-wide lockdown could have been reduced in both length and severity.518 |
| 6.232. | Some witnesses disagreed with the position of SAGE, which was that the UK had reached that stage by September 2020. Professor Woolhouse explained that, in September, R was not as high as it had been in March 2020:
“This immediately indicated that we did not need such a drastic response as was felt necessary in March to bring the epidemic under control again; in other words, we did not need another lockdown.“519 Professor Woolhouse was critical of Professor Vallance’s opinion that the UK’s response should be “quick and hard“.520 He expressed a different view, that “earlier action can be less drastic action“.521 |
| 6.233. | Mr Hancock considered that an earlier implementation of the tiers system might have avoided both the need for a second England-wide lockdown and the subsequent closure of schools in January 2021.522 |
| 6.234. | As for when the second lockdown, once required, should have been imposed, Professors Vallance, Whitty and McLean all believed that it should have been imposed at an earlier date.523 Other witnesses expressed similar views, including Sir Christopher Wormald (Permanent Secretary to the Department of Health and Social Care from May 2016 to December 2024), Mr Gove and Mr Cain.524 |
| 6.235. | For his part, Mr Johnson told the Inquiry:
“I felt at the time – and still feel today – that the decision to impose a second lockdown was timely. If a government is to enforce such enormous restrictions on individual liberty, it must first try all other solutions.“525 |
| 6.236. | The Inquiry accepts that a second lockdown was to be avoided at all costs. Unfortunately, the failure to take timely action had made one inevitable. Once the second lockdown had become inevitable, the sooner it was imposed the better. The Inquiry’s view is that Mr Johnson should have ordered the imposition of a circuit breaker lockdown in late September or early October 2020. |
| 6.237. | Failure to take early and decisive public health action is likely to have dire implications in the context of a viral pandemic where the virus is spreading exponentially. Concern over the economic and societal damage ensuing from a circuit breaker had to give way to the greater imperative of saving lives. The failure to get a grip on the second wave sooner contributed to greater mortality and the inevitability of a second lockdown – one that was longer and, thus, more damaging. |
November and early December 2020
| 6.238. | Three of the four nations were in a form of lockdown in early November 2020. Unlike the rest of the UK, Scotland did not have a lockdown or other circuit breaker during this period. Although the test positivity rate and the number of deaths rose in Scotland, it did so at a more gradual rate than in England and Wales. The number of cases in Scotland never reached the peaks experienced in the rest of the UK around this time. Scotland continued to rely on local restrictions through the five-levels system. |
| 6.239. | On 17 November 2020, Ms Sturgeon announced Level 4 restrictions in 11 local authorities in Central Scotland and the West of Scotland, to give the “best possible chance” of being able to ease the restrictions for all of Scotland over the Christmas season.526 Some 2.3 million people were placed under the highest level of restrictions, under which non-essential shops, pubs and restaurants would close, but schools would remain open. People were not permitted to meet indoors, but up to six people from two households could still meet outdoors.527 These restrictions came into force on 20 November, creating a public expectation that the stringent measures would result in fewer restrictions over the Christmas period. A few days later, East Lothian and Midlothian moved from Level 3 to Level 2 restrictions.528 The Scottish Government also announced travel regulations preventing people who lived in a Level 3 or Level 4 area from travelling outside their local authority area, except for an essential purpose.529 |
| 6.240. | This targeted approach appears to have successfully avoided the need for a second nationwide lockdown in Scotland at this time for a number of reasons. These included: the NHS in Scotland having “sufficient reserve capacity“;530 the restrictions in October 2020 leading to a more gradual increase in cases than in England and Wales; strict Level 4 restrictions being implemented in good time and targeted to respond to local areas of significant concern; and the Level 4 restrictions covering a significant proportion of Scotland’s population. |
The rollout of the vaccine and mass testing
| 6.241. | It was at this point that there was transformative news concerning the development of a vaccine. On 9 November 2020, Pfizer and BioNTech announced that their vaccine appeared to be over 90% effective at preventing infection with Covid-19.531 The following day, Mr Johnson told the UK Cabinet that the UK had secured 40 million doses of the Pfizer/BioNTech vaccine.532 By early December 2020, temporary authorisation had been granted by the Medicines and Healthcare products Regulatory Agency.533 Rollout commenced shortly afterwards and authorisation for the Oxford/AstraZeneca and the Moderna vaccines followed in late December 2020 and early January 2021 respectively.534 |
| 6.242. | SAGE noted in mid-December 2020 that emerging data showed the vaccines could offer good protection against the disease, but the degree of protection conferred against infection and potential infectiousness remained unknown. It was:
“critical to get extremely high vaccine coverage in the most vulnerable groups … in order to limit the number of hospitalisations and deaths“.535 |
| 6.243. | In the event that the vaccines were not highly effective against infection and transmission, “the epidemic would continue to spread“.536 The advice of SAGE was that vaccines would:
“prevent more COVID-19 deaths if prevalence [was] kept low until a late stage of the vaccine rollout through maintenance of and adherence to NPIs [non-pharmaceutical interventions]”.537 |
| 6.244. | In Liverpool, the first mass testing pilot (part of the Moonshot programme) was rolled out in November.538 On 30 November 2020, mass testing was also announced for Scotland’s university students and residents of five areas of Scotland, including Glasgow, Ayrshire, Clackmannanshire and Renfrewshire.539 |
| 6.245. | Mr Johnson was optimistic that these developments would allow life to return to normal, telling the Cabinet in mid-November 2020 that “the cavalry was coming over the hill in the form of mass testing and vaccines“.540 There was, however, concern about the weight that was being placed on mass testing and vaccines by the UK government. Professor Whitty warned Mr Ridley in mid-November that he did not expect the vaccine to have “any measurable effect” until January 2021, and that any effect before April 2021 would be “modest“. He also cautioned against:
“stoking an excessive belief that testing alone, even if done well, is our salvation. It is not. It is a helpful adjunct, if it leads to isolation.“541 Professors Whitty and Vallance both considered that mass testing would not enable the widespread relaxation of measures, unless it was repeated frequently over time.542 Professor Whitty explained that mass testing: “would not identify those who might have been exposed prior to this point who would test negative but then go on to develop the disease in the following days. Nor could mass testing feasibly identify everyone with Covid-19 on that date, on the basis that some sections of the population would not come forward to be tested and of those who did, there would be a portion of false negative results.“543 |
| 6.246. | These limitations were reflected in the pilots. As Professor Whitty explained:
“[M]ass testing resulted in us identifying more of those who were positive (a good thing). There was however limited evidence that it had in and of itself contributed to a sustained slowing in rates of transmission.“544 |
| 6.247. | As predicted, implementation was also difficult.545 Professor Whitty considered the hope expressed by some that mass testing could be used to control the pandemic as “optimistic“.546 |
The challenges ahead
| 6.248. | The second wave was far from over. As Professor Whitty said: “The end was in sight but it was still quite a long way off.“547 The experience in the USA following social mixing at Thanksgiving (a shorter holiday period than Christmas) was cautionary, with Professor Whitty warning:
“The situation could still go badly wrong between now and the start of March, despite the fact that this was predictable, preventable and the end was in sight.“548 |
| 6.249. | In addition, although unknown at that time, the significantly more transmissible Alpha variant was well established in Kent by December 2020. It could not be restrained by the measures that were in place in England. Even without the Alpha variant, the situation was, in Professor Whitty’s view, “problematic: the emergence of Alpha made a subsequent lockdown virtually inevitable“.549 |
| 6.250. | Had lessons been learned from the first wave and timely and effective action taken to respond to the virus, a subsequent lockdown might have been avoided. |
-
- INQ000048867_0002 para 1.4; INQ000088262_0002; INQ000375628. Scotland recorded an increase of 101 cases on 3 September 2020, followed by a further 146 cases on 7 September (INQ000214504_0002; INQ000214284_0002).
- INQ000213284_0001 para 1; INQ000213274_0001 para 1
- INQ000088245
- INQ000249526_0099 para 306
- INQ000232194_0008 para 31
- Preparing for a Challenging Winter 2020/21, The Academy of Medical Sciences, 14 July 2020, p3 (https://acmedsci.ac.uk/file-download/51353957; INQ000440246); Patrick Vallance 20 November 2023 194/17-195/14
- INQ000090598_0002-0003; see also The Health Protection (Coronavirus, Wearing of Face Coverings in a Relevant Place) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/791/contents); INQ000048482_0004-0005; INQ000065578; INQ000137373; INQ000350825; INQ000023258
- The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, July 2020, p10 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000137239)
- ‘Plans to ease guidance for over 2 million shielding’, Department of Health and Social Care and Ministry of Housing, Communities and Local Government, 22 June 2020 (https://www.gov.uk/government/news/plans-to-ease-guidance-for-over-2-million-shielding;
INQ000237302); ‘Shielding to be paused’, Scottish Government, 23 July 2020 (https://www.gov.scot/news/shielding-to-be-paused; INQ000369739); INQ000414515_0094 para 250; INQ000048475_0004 para 11; INQ000391115_0058 para 226 - ‘Schools to re-open full-time’, Scottish Government, 30 July 2020 (https://www.gov.scot/news/schools-to-re-open-full-time; INQ000585000)
- INQ000411550_0078-0079 para 232; ‘NHS COVID-19 app launches across England and Wales’, Department of Health and Social Care, 24 September 2020 (https://www.gov.uk/government/news/nhs-covid-19-app-launches-across-england-and-wales; INQ000237570)
- INQ000231034_0001; INQ000183867
- INQ000236261_0041-0042 para 9.28; INQ000192101
- INQ000236261_0049 paras 10.6-10.7
- INQ000192133_0003
- INQ000119954_0001
- INQ000236261_0050-0051 para 10.11
- INQ000269203_0140 para 13.8
- Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892)
- INQ000137228; INQ000207294_0020 para 3.19.6
- INQ000137228; INQ000207294_0020 para 3.19.6
- INQ000088245_0007
- INQ000207294_0028-0029 paras 3.35-3.36; INQ000119899
- INQ000137238_0002
- INQ000207294_0028-0029 para 3.35
- INQ000129427_0002
- INQ000232194_0116 para 467
- INQ000232194_0116 para 467
- INQ000088249_0004-0005
- INQ000088249_0005
- INQ000088249_0005
- INQ000255836_0120-0121 para 434
- INQ000089026
- INQ000199148
- The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, July 2020, p15 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000137239)
- The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, July 2020, p7 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000137239)
- The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, July 2020, pp7, 14-15 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000137239)
- The Next Chapter in Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, July 2020, pp9-10 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000086693)
- COVID-19 Contain Framework: A Guide for Local Decision-Makers, UK Health Security Agency, 17 July 2020 (https://www.gov.uk/government/publications/containing-and-managing-local-coronavirus-covid-19-outbreaks/covid-19-contain-framework-a-guide-for-local-decision-makers; INQ000593862); INQ000234406; see also INQ000233883; INQ000088861_0002
- The Health Protection (Coronavirus, Restrictions) (Blackburn with Darwen and Luton) Regulations 2020 on 25 July 2020 (https://www.legislation.gov.uk/uksi/2020/800/contents/made); The Health Protection (Coronavirus, Restrictions on Gatherings) (North of England) Regulations 2020 on 5 August 2020 (https://www.legislation.gov.uk/uksi/2020/828/contents/made); The Health Protection (Coronavirus, Restrictions) (Blackburn with Darwen and Bradford) (Amendment) (No. 3) Regulations 2020 on 3 September 2020 (https://www.legislation.gov.uk/uksi/2020/935/contents/made); The Health Protection (Coronavirus, Restrictions) (Bolton) Regulations 2020 on 10 September 2020 (https://www.legislation.gov.uk/uksi/2020/974/contents/made); The Health Protection (Coronavirus, Restrictions) (Birmingham, Sandwell and Solihull) Regulations 2020 on 15 September 2020 (https://www.legislation.gov.uk/uksi/2020/988/contents/made); The Health Protection (Coronavirus, Restrictions) (North East of England) Regulations 2020 on 18 September 2020 (https://www.legislation.gov.uk/uksi/2020/1010/contents/made)
- INQ000250231_0040 para 222; Patrick Vallance 20 November 2023 122/21-123/3
- INQ000250231_0040 para 223
- INQ000250231_0040 para 223
- INQ000088249_0008
- INQ000061555_0002 para 1
- INQ000088251_0005-0006; INQ000252914_0053-0054 paras 225-226
- INQ000061556_0003 para 18
- ‘Segmentation and shielding of the most vulnerable members of the population as elements of an exit strategy from Covid-19 lockdown’, B. van Bunnik, A. Morgan, P. Bessell, G. Calder-Gerver, F. Zhang, S. Haynes, et al., Philosophical Transactions of the Royal Society B: Biological Sciences (2021), 376(1829) (https://doi.org/10.1098/rstb.2020.0275; INQ000220376); INQ000351892; INQ000213073_0003. This work was later discussed by SAGE in October 2020: see INQ000061570_0003-0004 paras 18-22; see also INQ000250231_0040 para 222
- INQ000309529_0031-0032 paras 102-103; Patrick Vallance 20 November 2023 121/10-25
- Patrick Vallance 20 November 2023 123/4-8
- INQ000252914_0054 para 226
- INQ000070579_0001
- INQ000070579_0001 para 3
- INQ000070579_0001 para 1
- INQ000252856_0001
- INQ000191780; INQ000147255
- INQ000048857_0003 para 2.3
- Quentin Sandifer 6 March 2024 65/1-8; INQ000191782_0005-0007
- INQ000191782_0007; INQ000191780; INQ000220655_0008
- INQ000147256; Quentin Sandifer 6 March 2024 65/1-11; INQ000232439_0003 para 8
- INQ000267867_0027 para 112
- Quentin Sandifer 6 March 2024 66/3-12
- INQ000349671_0002 para 7
- Reg Kilpatrick 6 March 2024 182/13-184/2
- INQ000320919_0001
- INQ000137244_0001
- INQ000048399_0025
- INQ000102205_0001
- INQ000048399_0025
- INQ000061557_0002 para 7
- INQ000088797_0006, 0009; INQ000106553_0002 para 4; INQ000062459_0002
- INQ000088797_0009
- A Plan for Jobs, HM Treasury, 8 July 2020 (https://www.gov.uk/government/publications/a-plan-for-jobs-documents/a-plan-for-jobs-2020; INQ000235047)
- INQ000327611_0004-0005; INQ000273747_0036 para 119; INQ000539015_0045
- INQ000088797_0009
- ‘Coronavirus: Scots warned to avoid Covid hotspots in England’, BBC News, 31 July 2020 (https://www.bbc.co.uk/news/uk-scotland-53608460; INQ000357462); ‘Travel to North West of England’, Scottish Government, 31 July 2020 (https://www.gov.scot/news/travel-to-north-west-of-england; INQ000585003)
- INQ000065789_0001
- INQ000353624_0001
- INQ000048484_0002 para 5
- INQ000353624_0001
- INQ000414515_0046 para 102
- INQ000048485_0002 para 2
- INQ000120551_0001
- INQ000137249_0002-0003; see also The Health Protection (Coronavirus) (Restrictions on Holding of Gatherings and Amendment) (England) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/907/contents/made); The Health Protection (Coronavirus, Wearing of Face Coverings in a Relevant Place and on Public Transport)(England) (Amendment) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/906/contents/made)
- INQ000137249_0004; ‘Prime Minister announces stronger enforcement measures as easements resume’, Prime Minister’s Office and Department for Digital, Culture, Media and Sport, 13 August 2020 (https://www.gov.uk/government/news/prime-minister-announces-stronger-enforcement-measures-as-easements-resume; INQ000053686)
- INQ000048862_0003 para 1.9
- Coronavirus Control Plan for Wales, Welsh Government, August 2020 (https://www.gov.wales/sites/default/files/publications/2020-08/coronavirus-control-plan-for-wales.pdf; INQ000349794)
- Coronavirus Control Plan for Wales, Welsh Government, August 2020, p2 (https://www.gov.wales/sites/default/files/publications/2020-08/coronavirus-control-plan-for-wales.pdf; INQ000349794)
- INQ000320919_0001; Reg Kilpatrick 6 March 2024 182/13-184/2
- INQ000116015_0002
- Arlene Foster 15 May 2024 95/9-14
- INQ000276510_0017 para 74(iv)
- INQ000065790_0002
- INQ000048486_0003 para 10(iv)
- INQ000061560_0002 para 2; INQ000120552_0001 para 1
- A Plan for Jobs, HM Treasury, 8 July 2020, p17 (https://www.gov.uk/government/publications/a-plan-for-jobs-documents/a-plan-for-jobs-2020; INQ000235047); INQ000235019
- INQ000263374_0082 para 290; INQ000232086_0002; Stuart Glassborow 6 November 2023 80/3-12
- INQ000255836_0119 para 430
- INQ000255836_0118-0119 para 429; INQ000263374_0067 paras 237-238; Rishi Sunak 11 December 2023 117/3-16
- INQ000235019_0001
- INQ000088069_0004 para 21
- INQ000215049_0053 para 157
- INQ000263374_0075-0076 para 269; Rishi Sunak 11 December 2023 115/7-23
- INQ000263374_0076 para 271
- INQ000263374_0076 para 271; ‘Pubs, restaurants and hairdressers to reopen from 4 July’, Department for Business, Energy and Industrial Strategy and Alok Sharma, 24 June 2020 (https://www.gov.uk/government/news/pubs-restaurants-and-hairdressers-to-reopen-from-4-july; INQ000065410)
- INQ000339033_0115 para 320; INQ000391237_0076 paras 294-295; INQ000409589_0031 para 85; INQ000421704_0175-176 para 386; INQ000436641_0036 para 133; Rishi Sunak 11 December 2023 125/10-19
- INQ000339033_0115 para 320; Rishi Sunak 11 December 2023 125/10-19
- INQ000371209_0056 para 182
- INQ000080969_0004
- Nicola Sturgeon 31 January 2024 187/2-10
- INQ000353624; Ian Young 7 May 2024 163/20-164/4
- Matt Hancock 30 November 2023 208/8-12; Simon Case 23 May 2024 130/13-14; Simon Ridley 7 November 2023 59/3-5; INQ000280628 para 126
- INQ000255836_0119 para 430
- Boris Johnson 7 December 2023 8/2-13
- INQ000235261_0001; INQ000088242_0004
- INQ000251645_0125 para 8.32; see also INQ000238826_0115 para 346
- Patrick Vallance 20 November 2023 93/14-23; Matt Hancock 30 November 2023 210/1-3; INQ000252711_0027 para 121(b); Lee Cain 31 October 2023 63/1-11
- Patrick Vallance 20 November 2023 93/14-23
- INQ000252711_0027 para 121(b)
- INQ000137251
- INQ000218343
- INQ000273872_0061-0062 para 282
- INQ000283296_0025
- INQ000048399_0032
- INQ000232194_0008 para 31
- INQ000283369_0041
- INQ000304290_0001
- INQ000065729_0003
- INQ000088930_0008. See also the minutes from a meeting of Covid-S on 16 July 2020 (INQ000088249_0005).
- INQ000088930_0007
- INQ000070554_0001
- INQ000070569_0001
- SAGE estimated R for the UK to be between 0.9 and 1.1 (INQ000061563_0002 para 1).
- INQ000088964_0005
- INQ000320919
- The Health Protection (Coronavirus Restrictions) (No. 2) (Wales) (Amendment) (No. 8) (Caerphilly) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/961/made)
- INQ000220655_0004
- INQ000385533_0003
- Dr Sandifer had previously raised this on 24 August 2020 (Quentin Sandifer 6 March 2024 64/2-65/11).
- INQ000217906
- INQ000214448_0010 para 40
- INQ000214448_0010, 0014-0015 paras 41, 57(a), 57(b)
- INQ000088964_0005
- INQ000088262_0006
- INQ000088964_0004
- INQ000088297_0003 para 8
- INQ000088297_0001-0002 paras 1, 3
- INQ000088297_0003-0004 para 8
- INQ000088263_0004-0005
- INQ000088263_0008
- INQ000088263_0008
- INQ000088263_0008
- INQ000233982_0001; INQ000088263_0009; INQ000088297_0004
- INQ000086845_0004; The Health Protection (Coronavirus, Restrictions) (No. 2) (England) (Amendment) (No. 4) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/986/contents)
- INQ000361620
- ‘Rule of six comes into effect to tackle coronavirus’, Home Office and Priti Patel, 14 September 2020
(https://www.gov.uk/government/news/rule-of-six-comes-into-effect-to-tackle-coronavirus; INQ000212110); INQ000086845 - INQ000049748_0020; INQ000061565_0002 paras 1-5; INQ000120554_0001 para 1
- INQ000273901_0176
- INQ000238826_0118 para 354
- INQ000238826_0118 para 355; INQ000251645_0136 para 8.48
- INQ000120554_0001 para 3
- INQ000233982_0001; INQ000088297_0003 para 8
- INQ000251645_0136 para 8.48
- INQ000273872_0093 para 468
- INQ000023258; INQ000048489_0004 paras 13-14; ‘Coronavirus: Maximum size of gatherings in Scotland cut to six’, BBC News, 10 September 2020 (https://www.bbc.co.uk/news/uk-scotland-54093110; INQ000357427)
- INQ000065565_0002 para 4; INQ000048486_0005 para 18(iii); INQ000425623_0003-0004 para 12; INQ000421704_0177 para 389
- INQ000048489_0004 para 13
- ‘Coronavirus: Maximum size of gatherings in Scotland cut to six’, BBC News, 10 September 2020 (https://www.bbc.co.uk/news/uk-scotland-54093110; INQ000357427)
- INQ000048867_0003 para 2.1; INQ000048862_0003 para 2.1
- INQ000023258; The Health Protection (Coronavirus Restrictions) (No. 2) (Wales) (Amendment) (No. 9) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/985/contents/made)
- INQ000090607_0001; INQ000349851_0001; INQ000145504_0008 para 44; INQ000361620
- INQ000086845_0005
- INQ000371699
- INQ000061561_0002 para 2
- INQ000120552_0001 para 5
- INQ000071531
- INQ000071531
- ‘Coronavirus (COVID-19) update: First Minister’s speech 7 September 2020’, Scottish Government, 7 September 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-7-september-2020; INQ000354272_0005)
- ‘Coronavirus: Maximum size of gatherings in Scotland cut to six’, BBC News, 10 September 2020 (https://www.bbc.co.uk/news/uk-scotland-54093110;
INQ000357427) - INQ000048489_0004 para 13
- INQ000048867_0002 para 1.4
- INQ000281839
- INQ000048488_0004 para 11; INQ000208760_0002, 0004-0005 paras 6, 12, 13
- INQ000065769_0017
- Ian Young 7 May 2024 169/1-5
- INQ000065769_0017
- INQ000120554_0001 para 1; INQ000066383_0002
- INQ000090165; INQ000233995_0001
- INQ000391115_0025-0026 paras 103, 106
- Frank Atherton 4 March 2024 48/18-50/8
- INQ000371209_0065 para 209
- Mark Drakeford 13 March 2024 137/12-138/3
- Frank Atherton 4 March 2024 53/11-19
- Mark Drakeford 13 March 2024 140/5-17
- See INQ000349411_0002; INQ000391115_0024-0025 paras 99, 102; Our Plan to Rebuild: The UK Government’s COVID-19 Recovery Strategy, HM Government, May 2020, pp31, 54 (https://www.gov.uk/government/publications/our-plan-to-rebuild-the-uk-governments-covid-19-recovery-strategy; INQ000198892)
- INQ000213284_0001 para 2; INQ000223534
- INQ000061565_0002-0004 paras 1-5, 15, 17, 23
- INQ000061565_0002-0003 paras 10, 17
- INQ000061565_0002-0003 para 10
- INQ000061565_0004
- INQ000213284 para 6
- INQ000260643_0062 para 6.29
- INQ000283722_0004
- INQ000102265_0002
- INQ000102265_0002
- INQ000129483
- INQ000129483
- INQ000118973
- INQ000273901_0188
- INQ000137293
- INQ000137293_0001 paras 1, 3
- INQ000137293_0003-0006
- INQ000137293_0003 para 6
- INQ000137293_0004 para 10
- INQ000137293_0003 para 7
- INQ000137293_0003, 0006 paras 7, 18
- INQ000273872_0095-0096 para 486; INQ000255836_0133-0134 para 476
- INQ000255836_0129-0130 paras 460-461; see also INQ000183965; INQ000238826_0125 para 372
- INQ000255836_0129 para 460
- INQ000255836_0128 para 457
- INQ000232194_0132 para 523
- INQ000146605
- INQ000146605
- INQ000146605
- INQ000146609
- INQ000309529_0043 para 143
- INQ000146608_0001
- INQ000249526_0090 para 274
- Professor Gupta was among the signatories to the Great Barrington Declaration, which called for the lifting of lockdown restrictions (and is discussed further below). Both Professors Gupta and Heneghan were on the scientific advisory board of ‘Collateral Global’, which campaigns against the imposition of mandated interventions.
- INQ000248853_0093-0094 para 6.24; INQ000146606; INQ000146607
- INQ000252725_0008-0009 para 30
- INQ000146607
- INQ000146607
- INQ000232194_0132 para 523
- INQ000255836_0131 para 464
- INQ000309529_0044 para 145
- INQ000215035_0031 para 119
- INQ000273872_0096-0097 paras 490, 492; INQ000146611_0002
- Simon Ridley 7 November 2023 83/8-12, 84/4
- INQ000252711_0029 paras 127-128
- INQ000252711_0029 paras 127-128
- INQ000255836_0132 para 470
- INQ000238826_0119-0120para 359
- INQ000061566_0002 para 2
- INQ000255836_0133-0134 para 476
- INQ000061566_0002 para 6
- INQ000184589_0001
- INQ000184589_0002
- INQ000232100_0001
- Rishi Sunak 11 December 2023 156/13-18
- INQ000255836_0134 para 478
- INQ000232194_0131 para 519
- INQ000238826_0119 para 358; INQ000251645_0140 para 8.52
- INQ000088271_0005-0009; INQ000232194_0133-0134 paras 525-526
- INQ000088299_0002 para 4; INQ000088271_006; see also INQ000065358
- INQ000091388_0001; INQ000083849
- INQ000214448_0011 para 51
- INQ000232100_0001; INQ000065358; INQ000023259
- The Health Protection (Coronavirus Restrictions) (No. 2) (Wales) (Amendment) (No. 11) (Blaenau Gwent, Bridgend, Merthyr Tydfil and Newport etc.) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/1022/contents)
- INQ000213664_0001 para 1; INQ000022457_0001-0002 paras 1, 3
- INQ000137293_0003-0004; INQ000251645_0141 para 8.54
- Boris Johnson 7 December 2023 30/12-13; INQ000255836_0133-0134 para 476
- Angela McLean 23 November 2023 80/20-81/1
- INQ000255836_0133-0134 para 476
- INQ000238826_0124 para 370; INQ000061565_0002 para 2; INQ000061566_0002 para 2
- INQ000249526_0101 para 312; see also INQ000309529_0043 para 143
- INQ000066391; INQ000233568; INQ000022457; INQ000065777
- INQ000213284_0001, 0004 paras 3, 25; INQ000061567_0001-0002
- INQ000061567_0002 para 15
- INQ000217906_0001
- INQ000326427_0004-0005 paras 21-22
- INQ000326426_0001 para 1
- INQ000326426_0001 para 6
- INQ000304276_0002
- INQ000304274_0002
- INQ000213274_0001 para 2
- INQ000089096_0004-0005
- INQ000120560_0001 paras 1-2
- INQ000346272_0037 para 124
- INQ000231036_0001, 0003
- INQ000061569_0002-0003 paras 2, 19
- INQ000083851_0007 para 11
- INQ000371209_0067-0068 para 217
- INQ000371209_0067-0068 para 217
- INQ000251645_0125 para 8.31
- INQ000238826_0112-0113 para 340
- INQ000238826_0112-0113 para 340
- INQ000232194_0131-0132 para 521
- INQ000232194_0127, 0131-0132 paras 508, 521
- The Health Protection (Coronavirus, Restrictions) (Leicester) (Amendment) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/754)
- The Health Protection (Coronavirus, Restrictions) (Leicester) (Amendment) (No. 2) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/787/made)
- The Health Protection (Coronavirus, Restrictions) (Leicester) (Amendment) (No. 3) Regulations 2020
(https://www.legislation.gov.uk/uksi/2020/823/contents) - The Health Protection (Coronavirus, Restrictions) (Leicester) (No. 2) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/824/contents); see also, for example, The Health Protection (Coronavirus, Restrictions) (Blackburn with Darwen and Bradford, Leicester, and North of England) (Amendment) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/954/contents); The Health Protection (Coronavirus, Restrictions) (Leicester) (No. 2) (Amendment) (No. 2) Regulations 2020 (https://www.legislation.gov.uk/uksi/2020/987/contents)
- INQ000090177_0008-0009
- ‘Prime Minister’s statement on coronavirus (COVID-19): 12 October 2020’, Prime Minister’s Office and Boris Johnson, 12 October 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-12-october-2020; INQ000075749_0001-0003)
- INQ000234082_0003
- INQ000234082_0003 para 9
- INQ000234082_0003
- INQ000237819_0017 para 33
- INQ000232194_0137-0138 para 538
- INQ000252869_0001
- INQ000259848_0053 para 101
- INQ000249818_0004 para 11
- INQ000216991_0028-0029 paras 93, 96
- INQ000090266_0006
- Edward Udny-Lister 7 November 2023 197/10-13
- INQ000090164_0004-0005; INQ000075012_0002
- INQ000238826_0128 para 382
- INQ000229676_0002
- INQ000229676
- INQ000090163_0005
- INQ000062726
- INQ000083851_0005, 0008
- INQ000236412_0003
- INQ000238826_0128-0129 para 383
- INQ000273901_0220
- INQ000255836_0155 para 549
- INQ000087467_0001; INQ000061572_0003; INQ000183990_0012; INQ000090298_0001
- INQ000273901_0233
- INQ000213277_0006 para 25
- INQ000232194_0142 para 554
- INQ000273553_0068 para 10.23
- INQ000269203_0104 para 7.35
- INQ000216991_0032 para 107; INQ000232194_0140 para 545
- INQ000071722_0001-0003 paras 2, 4, 9
- INQ000251645_0142 para 8.61
- INQ000255836_0148 para 529
- INQ000429240
- ‘Coronavirus (COVID-19) update: First Minister’s speech 5 October 2020’, Scottish Government, 5 October 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-5-october-2020; INQ000354262)
- INQ000217915_0006
- ‘Covid in Scotland: Sturgeon to meet advisers over further restrictions’, BBC News, 5 October 2020 (https://www.bbc.co.uk/news/uk-scotland-54415973; INQ000360171)
- INQ000214451_0003 para 9
- INQ000232743_0003-0004 para 9
- INQ000232743_0003-0004 para 9; ‘New moves to stop COVID-19 spread’, Scottish Government, 7 October 2020 (https://www.gov.scot/news/new-moves-to-stop-covid-19-spread; INQ000369721)
- ‘Covid in Scotland: Sturgeon to draw up “three-tier” lockdown system’, BBC News, 12 October 2020 (https://www.bbc.co.uk/news/uk-scotland-54509401; INQ000360170)
- ‘Covid in Scotland: Sturgeon to draw up “three-tier” lockdown system’, BBC News, 12 October 2020 (https://www.bbc.co.uk/news/uk-scotland-54509401; INQ000360170)
- ‘Coronavirus (COVID-19) update: First Minister’s speech 23 October’, Scottish Government, 23 October
2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-23-october; INQ000354218) - COVID-19: Scotland’s Strategic Framework, Scottish Government, October 2020, p9 (https://www.gov.scot/publications/covid-19-scotlands-strategic-framework; INQ000245551)
- ‘Covid-19: Nicola Sturgeon unveils Scotland’s restriction levels’, BBC News, 29 October 2020 (https://www.bbc.co.uk/news/uk-scotland-54731245;
INQ000357730) - INQ000183806
- INQ000183797
- INQ000183790_0012
- Mark Drakeford 13 March 2024 143/15-144/2
- INQ000048785
- INQ000048785
- Technical Advisory Cell: Summary of Advice, Welsh Government, 2 October 2020, p2 (https://www.gov.wales/technical-advisory-cell-summary-advice-2-october-2020; INQ000066408); INQ000412103
- INQ000395839
- INQ000222714_0002 para 2.8. Incidence had reached more than 100 cases per 100,000 people (INQ000066397_0002-0003). See also Rob Orford 4 March 2024 135/1-16
- Mark Drakeford 13 March 2024 144/15-18
- INQ000374391
- INQ000056301
- INQ000349942_0001
- INQ000198496
- INQ000320989
- INQ000198495
- INQ000198504_0002
- INQ000048796 para 1.7
- INQ000385731
- INQ000048876_0005
- INQ000048876_0001
- INQ000048876_0006
- INQ000048796 para 1.3; INQ000216548
- INQ000256872
- ‘Wales to introduce travel restrictions to prevent the spread of coronavirus’, Welsh Government, 14 October 2020 (https://www.gov.wales/wales-to-introduce-travel-restrictions-to-prevent-the-spread-of-coronavirus; INQ000585006); INQ000023265
- INQ000216554
- INQ000048801; INQ000048877
- INQ000048801_0002 para 1.4. Triggers (what the Welsh Government called ‘circuit breakers’) two and three (transmission) and six (hospital occupancy) had in fact been breached since 17, 27 and 30 September respectively (INQ000048887_0003).
- INQ000048887
- INQ000048877_0005
- INQ000048802_0002 para 1.3
- INQ000048802
- INQ000362237_0068-0069 paras 237-239
- INQ000216555
- INQ000371209_0070 para 227; INQ000274156_0048-0049 para 154; INQ000389184_0020 para 72
- Michael Gravenor 1 March 2024 175/20-176/3
- INQ000274156_0042 para 136
- INQ000371209_0067 paras 215-216
- Mark Drakeford 13 March 2024 143/24-144/24
- Vaughan Gething 11 March 2024 163/3-164/23
- INQ000061565_0002-0004 paras 1-5, 15, 17, 23; INQ000238826_0119-0120 para 359; INQ000061566_0002 para 2; INQ000395839; INQ000374391; INQ000371209_0067-0068 para 217; ‘National coronavirus firebreak to be introduced in Wales on Friday’, Welsh Government, 19
October 2020 (https://www.gov.wales/national-coronavirus-fire-break-to-be-introduced-in-wales-on-friday; INQ000651705) - INQ000022503; INQ000227863
- INQ000022503_0003 para 1.8; INQ000391115_0044 para 172
- ‘Chief Medical Officer advice on post-firebreak arrangements’, Welsh Government, 3 November 2020 (https://www.gov.wales/chief-medical-officer-advice-post-firebreak-arrangements; INQ000048755)
- INQ000584995_0063-0069
- INQ000066436_0002
- INQ000129860_0008
- INQ000281964
- INQ000350028
- INQ000350028
- INQ000048899
- INQ000048927_0002; see also INQ000048925; INQ000048930
- INQ000376546
- INQ000048927; INQ000048930
- INQ000350039_0003
- INQ000356177_0064 para 248
- INQ000390618_0050 para 152; Vaughan Gething 11 March 2024 180/9-11
- Ian Diamond 29 February 2024 80/10-12; INQ000271436_0045-0046
- INQ000066291_0002-0003; INQ000390618_0051 para 154
- INQ000048491 para 3
- INQ000418976_0034 para 109
- INQ000065632_0001 paras 1-2
- INQ000418976_0034 para 109
- INQ000418976_0034 para 109
- INQ000048491 para 3
- INQ000418976_0034 para 109
- INQ000276520_0005; see also Arlene Foster 15 May 2024 104/5-11
- INQ000065756_0017
- INQ000065756_0016
- INQ000048492_0003 para 7
- INQ000286275_0002-0003
- INQ000439242_0001
- INQ000286275_0002
- INQ000286275_0003; INQ000212923
- INQ000347375_0003
- INQ000212923_0001 para 1
- INQ000212923_0003 para 12
- INQ000212923_0009 para 35
- INQ000212923_0010 para 37
- INQ000065652_0011
- INQ000065652_0012
- INQ000065652_0013
- INQ000208778_0005 para 11
- INQ000065753; INQ000022458
- INQ000022458_0004 paras 17, 19(iv); INQ000208778_0001-0003 para 4
- INQ000022458_0003-0004 para 15
- INQ000022458_0004 para 16
- INQ000418976_0037 para 118
- Arlene Foster 15 May 2024 105/17-25, 106/1-8
- Arlene Foster 15 May 2024 121/20-24; see also Arlene Foster 15 May 2024 121/7-17
- INQ000065686_0001
- INQ000065702_0002
- INQ000065589_0001
- INQ000065589_0002
- INQ000065589_0007
- INQ000065757_0009, 0011-0012
- INQ000213652_0001; INQ000276538_0002
- INQ000276538_0002
- INQ000418976_0037 para 118
- INQ000356174_0053; Arlene Foster 15 May 2024 120/4-8, 20-24; INQ000048497_0003, 0007 paras 14, 45
- INQ000213652_0077; INQ000048497_0006; INQ000458927
- INQ000421759_0040-0041 para 127; INQ000452485_0028 para 97; Robin Swann 13 May 2024 173/16-25
- Peter Weir 8 May 2024 98/6-8; Arlene Foster 15 May 2024 125/13-17
- INQ000048497_0010-11 para 71
- INQ000137370
- INQ000412903_0054 para 162; see also INQ000048498
- INQ000065739_0010, 0012, 0018; see also INQ000065739_0035
- INQ000276547
- INQ000286272; Ian Young 7 May 2024 194/6-9
- INQ000048497_0010-0011 para 71. This included the reopening of close-contact services and the reopening of hospitality settings on a graduated basis (with unlicensed premises such as cafes and coffee shops opening on 20 November 2020 with restricted opening hours).
- INQ000276547
- INQ000065728_0002
- INQ000146617_0001; INQ000061570_0002
- INQ000217005
- INQ000217007
- INQ000273901_0608
- INQ000146633_0007
- INQ000273901_0245
- INQ000146633_0007
- INQ000273901_0608
- INQ000146617_0001-0002 paras 2, 4, 7
- INQ000146617_0007-0008
- INQ000090176_0004
- INQ000090176_0005
- INQ000136682; INQ000136686; INQ000136687
- INQ000090156; INQ000136684
- INQ000089102_0005-0006; ‘Prime Minister’s statement on coronavirus (COVID-19): 31 October 2020’, Prime Minister’s Office and Boris Johnson, 31 October 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-31-october-2020; INQ000086830)
- INQ000136672_0001
- ‘Prime Minister’s statement on coronavirus (COVID-19): 31 October 2020’, Prime Minister’s Office and Boris Johnson, 31 October 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-31-october-2020; INQ000086830)
- ‘Prime Minister’s statement on coronavirus (COVID-19): 31 October 2020’, Prime Minister’s Office and Boris Johnson, 31 October 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-31-october-2020; INQ000086830)
- INQ000255836_0151 para 536
- INQ000273872_0097-0098 para 496
- Simon Case 23 May 2024 153/25, 154/1
- INQ000303253_0050
- Boris Johnson 7 December 2023 56/24-57/2
- INQ000234141_0002. The effect was expected to be seen in approximately two to three weeks (INQ000061574_0002).
- INQ000088940_0005-0007
- INQ000253921_0001-0006; INQ000148865
- INQ000184006_0004
- INQ000090928_0010-0011
- INQ000061577_0001-0002, 0005
- INQ000089062_0006
- COVID-19 Winter Plan, HM Government, November 2020, pp26-30 (https://www.gov.uk/government/publications/covid-19-winter-plan; INQ000137262)
- INQ000253897_0002
- INQ000238826_0132 para 395; INQ000251645_0149 para 8.77; INQ000269203_0106 para 7.42
- INQ000250981_0003
- INQ000250981_0002-0003
- INQ000248853_0093 para 6.22
- Christopher Whitty 22 November 2023
- INQ000220154_0006 para 2.19
- INQ000250231_0032 para 176
- INQ000251645_0110 para 7.157
- INQ000061570_0004
- Lee Cain 31 October 2023 65/18-19
- INQ000238826_0131 para 391
- INQ000238826_0097-0098 para 299
- Lee Cain 31 October 2023 65/13-15
- Lee Cain 31 October 2023 65/22-25, 66/1-10
- INQ000232194_0008 para 31
- INQ000273553_0069-0070 para 10.28
- INQ000309529_0043-0044 para 144
- INQ000061570_0003 paras 15-17. CoMix, which commenced in March 2020, surveyed a sample of the UK adult population to identify social contact trends.
- Christopher Whitty 22 November 2023 66/24-25, 67/1-3
- INQ000273872_0093 para 468
- INQ000048313_0054
- INQ000267902_0001
- INQ000273901_0245
- INQ000273901_0247
- Boris Johnson 6 December 2023 41/4-8
- INQ000250981; INQ000146605
- INQ000236243_0025-0026 para 81
- INQ000236243_0030 para 98
- INQ000273901_0597
- ‘Lockdown failed. We must follow the Swedish model and learn to live with Covid’, Professor Mark Woolhouse, Daily Telegraph, 19 September 2020 (https://www.telegraph.co.uk/news/2020/09/19/uk-needs-follow-swedish-model-learn-live-covid; INQ000103523)
- INQ000252711_0028 para 125
- INQ000273872_0098 para 497
- INQ000237819_0017 para 32; Edward Udny-Lister 7 November 2023 192/23-193/6
- Boris Johnson 7 December 2023 41/17-21
- INQ000260643_0062-0063 para 6.30; INQ000233631_0001
- INQ000250231_0036 para 200
- INQ000088263_0008
- INQ000250231_0036 para 201
- Matt Hancock 1 December 2023 3/17-21; INQ000232194_0144 para 558
- INQ000238826_0131 para 390; Christopher Whitty 22 November 2023 65/16-25; INQ000309529_0045 para 147
- INQ000280628_0067-0068. para 125; Michael Gove 28 November 2023 143/7-14; INQ000252711_0028 para 123
- INQ000255836_0155 para 549
- ‘Coronavirus (COVID-19) update: First Minister’s statement Tuesday 17 November 2020’, Scottish Government, 17 November 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-tuesday-17-november-2020; INQ000354350); ‘Covid in Scotland: Level 4 move “could help ease rules at Christmas”, BBC News, 16 November 2020 (https://www.bbc.co.uk/news/uk-scotland-54960028; INQ000357587)
- COVID-19: Scotland’s Strategic Framework, Scottish Government, October 2020, pp58-69 (https://www.gov.scot/publications/covid-19-scotlands-strategic-framework; INQ000245551)
- INQ000214796_0007
- ‘Updated COVID-19 protection levels supported’, Scottish Government, 19 November 2020 (https://www.gov.scot/news/updated-covid-19-protection-levels-supported; INQ000369748)
- INQ000078524_0004, 0012, 0013 para 15
- ‘Pfizer and BioNTech announce vaccine candidate against COVID-19 achieved success in first interim analysis from Phase 3 study’, Pfizer, 9 November 2020 (https://www.pfizer.com/news/press-release/press-release-detail/pfizer-and-biontech-announce-vaccine-candidate-against; INQ000421407)
- INQ000088986_0005-0006
- ‘COVID-19 vaccine authorised by medicines regulator’, Department of Health and Social Care, Department for Business, Energy and Industrial Strategy and Alok Sharma, 2 December 2020 (https://www.gov.uk/government/news/covid-19-vaccine-authorised-by-medicines-regulator;
INQ000479077) - ‘Landmark moment as first NHS patient receives COVID-19 vaccination’, NHS England, 8 December 2020 (https://www.england.nhs.uk/2020/12/landmark-moment-as-first-nhs-patient-receives-covid-19-vaccination; INQ000237370)
- INQ000120576_0003 para 21
- INQ000061580
- INQ000061580
- INQ000251645_0194 para 10.6; ; ‘Liverpool to be regularly tested for coronavirus in first whole city testing pilot’, Department of Health and Social Care, 3 November 2020 (https://www.gov.uk/government/news/liverpool-to-beregularly-tested-for-coronavirus-in-first-whole-city-testing-pilot; INQ000086810)
- ‘Covid in Scotland: Students and “hotspot” areas targeted in testing’, BBC News, 30 November 2020 (https://www.bbc.co.uk/news/uk-scotland-55101155; INQ000357678)
- INQ000089030_0005; see also INQ000280061_0242
- INQ000236416_0001
- INQ000251645_0195 para 10.8; Patrick Vallance 20 November 2023 135/1-13
- INQ000251645_0195 para 10.7
- INQ000251645_0195 para 10.9; INQ000071945
- INQ000238826_0165-0166 para 501
- INQ000251645_0195 para 10.7
- INQ000088967_0005
- INQ000072078_0001
- INQ000251645_0156-0157 para 8.98
Chapter 7: Further lockdowns (December 2020 to April 2021)
Introduction
| 7.1. | In December 2020, the first vaccine was approved in the UK and the subsequent rollout of vaccines began in all four nations. This was rightly described as “a decisive turning point in the battle against the virus”.1 The decisions taken by the UK government and devolved administrations for the remainder of the pandemic must be viewed in this context. |
| 7.2. | The arrival of a vaccine coincided with a rapid rise in infections in south-east England. This was driven by a new variant of Covid-19 – known as Alpha – which emerged in Kent during the autumn of 2020. As explained by Professor Sir Christopher Whitty, Chief Medical Officer for England from October 2019, “all viruses mutate over time”.2 A mutation with “significant characteristics” such as increased transmissibility or severity will be designated as a “Variant of Concern”.3 The Alpha variant was designated by the World Health Organization as a variant of concern on 18 December 2020. On the same day, the New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) advised that the Alpha variant was 71% more transmissible than the original strain and that it increased the reproduction number (R) by between 0.39 and 0.93.4 |
| 7.3. | This chapter considers the key events from early December 2020 to the end of April 2021, including the peak in early January 2021 of the ‘second wave’ of Covid-19, in light of these two developments. It will consider whether earlier lessons were learned sufficiently well by the four governments of the UK. These lessons included the need to react swiftly and decisively to rising infection rates, to protect the vulnerable and those ‘at risk’ from both the effects of the virus and the restrictions, and the need for governments to work effectively together. |
December 2020 to early January 2021
| 7.4. | The development of a vaccine was a remarkable achievement. The UK was the first country in the world to approve a vaccine and commence a vaccination programme. On 2 December 2020, temporary authorisation was granted by the Medicines and Healthcare products Regulatory Agency for the Pfizer/BioNTech vaccine.5 This was announced by Boris Johnson MP, Prime Minister from July 2019 to September 2022, as the second lockdown in England lifted. Rollout commenced on 8 December 2020, with the first NHS England patient, a 90 year old, vaccinated in accordance with advice on prioritisation from the Joint Committee on Vaccination and Immunisation.6 The Scottish Government announced that the first vaccinations against Covid-19 had been given in Scotland to those who would be carrying out the vaccination programme.7 Both the Welsh Government and the Department of Health (Northern Ireland) adopted the Joint Committee on Vaccination and Immunisation prioritisation structure, beginning with care home residents and staff.8 Authorisation for the Oxford/AstraZeneca vaccine followed swiftly on 30 December 2020 and for the Moderna vaccine on 8 January 2021. Vaccines and therapeutics are explored in detail in Module 4: Vaccines and therapeutics. |
| 7.5. | However, it would take a considerable amount of time for the vaccine rollout to begin to have a significant effect on transmission and on mortality rates. With infections still rising, trying to stop the spread of the disease remained imperative. |
| 7.6. | By 1 December 2020, R had risen to 1, and might have been as high as 1.1 in Northern Ireland. A modelling paper from the Department of Health (Northern Ireland) noted that this likely reflected behaviours and interactions in the preceding week, when cafes and close-contact services had been open.9 The number of hospital inpatients had fallen more slowly than admissions and remained at a relatively high level. The number of Covid-19-positive intensive care unit patients in Northern Ireland stood at 38.10 There remained a risk that hospitals would come under severe pressure in the period after Christmas when staff availability would normally be lower.11 |
| 7.7. | The same day, Michelle O’Neill MLA, deputy First Minister from January 2020 to February 2022, confirmed that the “Strategic Objective is R below 1 and protect the Health Service”.12 Professor (later Sir) Michael McBride, Chief Medical Officer for Northern Ireland from September 2006, advised:
“[F]rom a narrow health perspective the way to maintain R being low is to maintain all current restrictions. Series of policy choices for the Executive relaxations which they can then advise on. Clear priority in relation to schools which causes difficulties in keeping both them and hospitality open.”13 As subsequent events were to demonstrate, this did not translate into a collective ministerial aim. |
| 7.8. | On 1 December 2020, the Scottish Cabinet considered rising cases in both Aberdeen City and Aberdeenshire. It had been recommended that these areas be put into Level 3 of Scotland’s Covid-19 management system, which would mean that no non-essential travel would be allowed out of that area and all leisure and entertainment venues would be closed.14 The ultimate decision as to whether the level should be changed was delegated to Nicola Sturgeon MSP, First Minister of Scotland from November 2014 to March 2023. |
| 7.9. | At the conclusion of the second lockdown on 2 December 2020, England returned to a three-tier system of local restrictions. Mr Johnson told the Cabinet that the tiers “would be reviewed after 14 days with areas being moved into a lower tier if the numbers justified that”.15 The first review was to take place on 16 December 2020, with Mr Johnson expressing optimism tempered by circumspection that, by then, there might be the potential to move areas to lower tiers.16 However, by 4 December 2020, Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, recorded in his evening notes that Mr Johnson reached the conclusion that “most people” were “going to be moved up a Tier in January” 2021.17 The weekend of 5 to 6 December saw the first Saturday and Sunday of Christmas shopping after the easing of the second lockdown. Scenes of crowds were reported across the national media. These scenes were to be repeated the following weekend, causing significant concern.18 |
| 7.10. | On 2 December 2020, the Welsh Cabinet agreed to prohibit travel to and from areas in Tier 3 in England and Level 3 and above in Scotland and to advise against the same for Tier 2 and Level 2.19 Travel was also prohibited to and from Northern Ireland, which had imposed a nationwide ‘circuit breaker’ (the stringent restrictions imposed for two weeks from 27 November 2020).20 |
| 7.11. | By the same date in Wales, positive test results for Covid-19 and the number of people both in hospital and in intensive care with Covid-19 were above what the Welsh Government called the “red circuit breaker“.21 By this, it meant headline indicators covering key information, including transmission of the virus and NHS capacity, with red representing a breach.22 A few days later, the Welsh Cabinet noted: “Wales was the only part of the UK where cases of Covid-19 were increasing.” 23 Public Health Wales recommended that “urgent additional action before Christmas is required”.24 It also advised that additional measures should be introduced similar to those implemented during the ‘firebreak’ (the stringent restrictions imposed in Wales for 17 days from 23 October 2020).25 |
| 7.12. | In an Executive Paper on 3 December 2020, Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021, and Ms O’Neill set out proposals for arrangements that might be made once the circuit breaker restrictions ended on 10 December.26 They also tabled a further paper on Christmas ‘bubbling’ arrangements, which noted that a decision had been made that up to three houses could form a Christmas ‘bubble’ over the period from 23 to 27 December 2020. An outstanding key issue to be considered was whether existing bubbles counted as part of a household.27 Both papers, together with one from the Department for the Economy (Northern Ireland) on the economic implications of the restrictions, were considered at the Executive meeting on 3 December. Ministers were also provided with a paper on R, which estimated that it was around 1.28 Professor McBride and Professor Ian Young (Chief Scientific Adviser to the Department of Health (Northern Ireland) from November 2015) advised that, if the Executive Committee wanted (as per its policy position) to keep R below 1, there should be no relaxation of the restrictions.29 |
| 7.13. | Despite that advice, a package of measures to take effect at the end of the two-week circuit breaker restrictions was agreed. This included the reopening of shops, hairdressers, restaurants, places of worship and hotels (among others).30 The paper estimated that infection rates would begin to rise again before Christmas. The decision was made to allow up to three households to form one bubble over Christmas (from 23 to 27 December 2020).31 |
| 7.14. | By 8 December 2020, it was understood that the two weeks of circuit breaker restrictions had not had the impact that had been hoped for. Consistent with Professor Young’s previous warning that “mid-December could be the ‘big risk period’”, Professor McBride advised the First Minister and deputy First Minister that he was “most concerned now” – the position was “fragile” and that should inform the messaging.32 Professor Young indicated that R was expected to move to 1.4 to 1.8 for two weeks.33 The Executive Committee nonetheless decided to ease restrictions in the two weeks leading up to Christmas. Acknowledging a desire to have as “normal a Christmas as possible”, Robin Swann MLA, Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024, confirmed that the messaging highlighted that restrictions before Christmas would mean a greater chance of Christmas gatherings.34 Similarly, Baroness Foster told the Inquiry that she had considered it important to “protect” Christmas to give people hope and something to look forward to.35 |
| 7.15. | In Wales, on 7 December 2020, Vaughan Gething MS (Minister for Health and Social Services in the Welsh Government from May 2016 to May 2021) made an entry in a notebook that Dr (later Sir) Frank Atherton (Chief Medical Officer for Wales from August 2016) had advised him and Mark Drakeford MS (First Minister of Wales from December 2018 to March 2024) that the “position is dire; visibly worse than the other UK nations”.36 On 8 December 2020, Dr Atherton advised the Welsh Government to “consider the need to adopt further national measures“, as recommended by Public Health Wales.”37 The following day marked the highest number of confirmed Covid-19 patients in hospitals in Wales on record.38 |
| 7.16. | Estimates from the Scientific Pandemic Influenza Group on Modelling, Operational sub-group (SPI-M-O) using data up to 8 December 2020 suggested that there were between 34,000 and 50,000 new infections per day in England.39 Over 2,000 new infections were reported in Wales on 8 December and the infection rate per 100,000 people in Wales was significantly higher than in both Scotland and England.40 The number of Covid-19 patients in hospital beds in Wales was “more than 500 higher than the peak of 1398 experienced in the first wave”.41 |
| 7.17. | At the outset of a discussion in the UK Cabinet on 8 December 2020, Mr Johnson also noted that “the numbers, especially in London, were going in the wrong direction”.42 Professor Whitty advised Cabinet that prevalence remained high, stating:
“Common sense and scientific modelling showed that the second wave of coronavirus in the UK was not yet over.“43 He reiterated that science would only rescue the “nation from the hole it was in by the spring, but not before then“.44 |
| 7.18. | On the same day, following a Scottish Cabinet discussion, it was announced that from 11 December 2020 the 11 areas in Scotland under Level 4 restrictions would be moved down to Level 3.45 On 10 December 2020, although the Scientific Advisory Group for Emergencies (SAGE) noted that there was a lag in the data, it stated:
“The latest estimate of R for the UK is 0.9 to 1.0 and 0.8 to 1.0 for England … Estimates of R for Scotland, Wales and Northern Ireland are 0.7 to 0.9, 0.9 to 1.2 and 0.8 to 1.1, respectively. SPI-M is not confident that R is less than 1 in Wales, or in some regions of England. There is a marked increase in the rate of infection for those aged 12-16 in London.”46 There had been “small increases in R” in some regions of England, including the East, the Midlands and the south-west.47 SAGE also reiterated that, where infection rates were increasing: “As previously noted, evidence shows that the earlier and more rapidly interventions are put in place, and the more stringent they are, the faster the observed reduction in incidence and prevalence.”48 |
| 7.19. | That same day, Covid-19 infection rates in Wales exceeded 370 in every 100,000 people.49 On the advice of Dr Atherton, Mr Drakeford and Kirsty Williams MS, Minister for Education in the Welsh Government from May 2016 to May 2021, jointly decided to move secondary schools and colleges to online learning from 14 December 2020.50 The Welsh Government had also decided the previous day to introduce four alert levels which would dictate the level of restrictions in Wales.51 There were clear warnings from the Chief Medical Officer for Wales and Public Health Wales about the need for urgent action. However, the Welsh Cabinet decided that Wales should only enter Level 4 restrictions from 28 December if transmission rates had not improved.52 |
The identification of the Alpha variant
| 7.20. | On the evening of 10 December 2020, Public Health England alerted Professor Whitty and Professor (later Sir) Jonathan Van-Tam, Deputy Chief Medical Officer for England from October 2017 to March 2022, to a “substantial genomic cluster of a variant of SARS-CoV-2” in Kent and north-east London.53 The following day, NERVTAG advised that the emergence of this new variant was a “matter for concern”.54 If it were more transmissible than the original variant, then controlling the epidemic would be much harder. There was also the possibility of reinfection, that the new variant would not be detected by diagnostic tests or that it would escape the vaccine.55 Professor Neil Ferguson, Mathematical Epidemiologist at Imperial College London, warned Professor Vallance that the new variant was “potentially rather worrying”.56 |
| 7.21. | The Scottish Government published COVID-19: Framework for Decision Making – Assessing the Four Harms of the Crisis on 11 December 2020.57 This set out the four harms and the process for assessment used to establish when coronavirus restrictions could be safely lifted after lockdown and the scientific evidence underpinning the decisions. |
| 7.22. | On 11 December 2020, Public Health Wales reiterated its 7 December advice to the Chief Medical Officer for Wales recommending urgent additional action before Christmas.58 Its estimate was that the:
“current weekly incidence in the community is around 400 per 100,000 … This compares to 153 per 100,000 in England … and 101.2 per 100,000 in Scotland.”59 |
| 7.23. | Advice from the Technical Advisory Cell dated 11 December 2020, which was shared with ministers on 15 December, confirmed that the number of people with confirmed Covid-19 in hospital had increased by 9% since the previous week.60 Professor Michael Gravenor, Professor of Biostatistics and Epidemiology at Swansea University, agreed that it was obvious by 11 December that Alert Level 4 restrictions were required. He said that, in retrospect, the third lockdown should have been implemented earlier and the Alpha variant had created a “perfect storm”.61 Restrictions in Wales had also been relaxed too quickly in the weeks following the end of the firebreak. By 2 December, case numbers and hospital admissions were already “nearly reaching levels seen at the beginning of the firebreak”.62 |
| 7.24. | On 11 December 2020 in Northern Ireland, as had been agreed by the Executive Committee on 3 December 2020, a number of sectors were permitted to reopen. These included non-essential businesses in retail and close-contact services, restaurants and cafes, hostels and guesthouses, places of worship, museums, galleries and libraries. So-called ‘wet pubs’ (drink-only public houses that do not serve food), theatres and nightclubs were to remain closed.63 |
| 7.25. | On 12 December 2020, Professor Whitty discussed the new variant in Kent with Mr Johnson.64 He and Professor Van-Tam advised Matt Hancock MP, Secretary of State for Health and Social Care from July 2018 to June 2021, that the number of Covid-19 cases was rising quickly in London and the south-east of England. It was unclear whether the new variant was responsible for this increase.65 |
| 7.26. | Mr Johnson subsequently chaired a UK government emergency meeting of the Cabinet’s Covid-19 Operations Committee (Covid-O) on 14 December.66 A presentation by the Joint Biosecurity Centre set out the exponential growth in infection rates in London and the south-east/east, at a rate that had not been seen since mid-March 2020. It forecast, on the trajectory observed, that there would be an eight-fold increase by Christmas 2020. It noted that the planned relaxation of household mixing restrictions at Christmas would inevitably accelerate transmission further. Case rates had continued to increase rapidly during Tier 3 restrictions in December, and Tier 3 was not containing the virus in Kent.67 |
| 7.27. | The consensus was that schools should remain open, with the Department for Education working up plans for a delayed return in January 2021 to enable testing to be put in place. Professors Whitty and Vallance urged caution about becoming obsessed with the new variant, reflecting their view that it was the epidemiological picture that was important. The lesson was that, if restrictions were “relaxed too early, infection rates came back quickly” and the virus would “take-off fast”.68 Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021, the sole voice arguing for placing London into Tier 3 on an earlier occasion, was recorded in Professor Vallance’s evening notes as advising that “measures from last year show we have been ‘too lenient & too late’ & we cannot make the same mistakes yet again”.69 The Covid-O meeting agreed that London and the areas of most concern in the south-east were to be placed into Tier 3 from 16 December 2020. Christmas plans remained in place and, alongside education and testing, were to be considered later that week. |
| 7.28. | The self-isolation requirement was reduced from 14 to 10 days on 14 December 2020, having been announced jointly by the Chief Medical Officers for the four nations of the UK a few days earlier.70 The Welsh Government also published its updated Coronavirus Control Plan: Alert Levels in Wales – A Guide to Restrictions, which explained “in more detail how national measures … will be introduced in a more predictable way“.71 |
Figure 19: Alert levels in Wales, December 2020
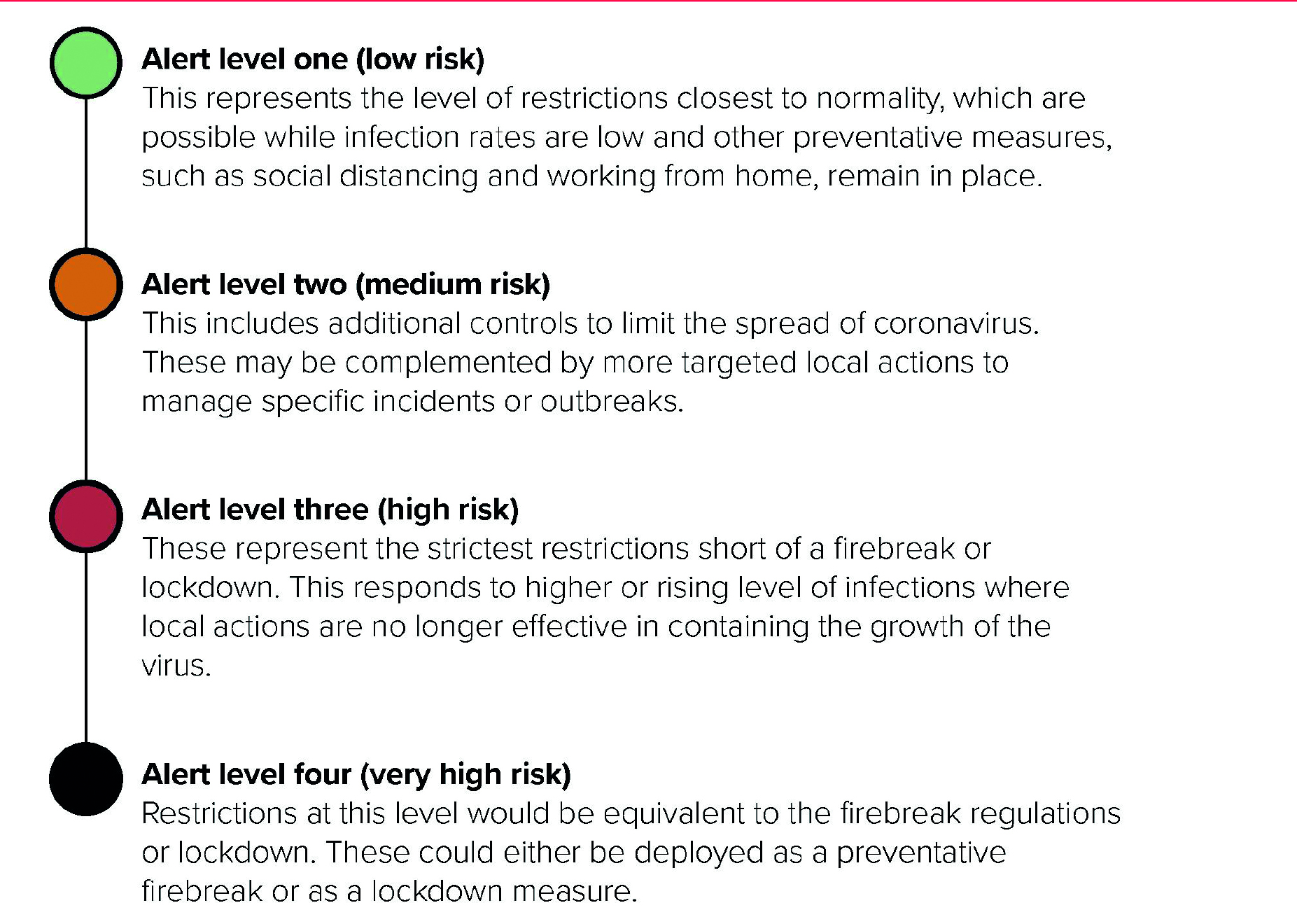
Source: Coronavirus Control Plan: Alert Levels in Wales. A Guide to Restrictions, Welsh Government, December 2020,
p3(https://www.gov.wales/sites/default/files/publications/2020-12/coronavirus-control-plan-alert-levels-in-wales.pdf; INQ000227576)
| 7.29. | The following day the Welsh Government was advised that the need to move to Alert Level 4 in Wales “appears to be clear” without waiting for further data.72 Dr Andrew Goodall, Director General of Health and Social Services in the Welsh Government and Chief Executive of NHS Wales from June 2014 to November 2021, continued to warn ministers of the worsening situation in NHS Wales.73 Public Health Wales advised Dr Atherton that “urgent additional action is required, as soon as practicable, before the Christmas period. Actions taken should be consistent with those described for alert level 4″.74 It also recommended a review of the Christmas relaxations.75 Mr Gething told the Inquiry that, by 15 December 2020, “we had a clear rationale to move ahead of the agreement the First Minister had reached with the other nations of the UK”.76 |
| 7.30. | At a meeting on 15 December 2020, the Scottish Cabinet discussed a proposal for a planned, pre-emptive escalation to Level 4 nationwide on 28 December for a period of three weeks.77 The Cabinet concluded that it:
“ran contrary to the levels-based approach: it could undermine the principles of the Strategic Framework by causing restrictions to be imposed in areas where such a response would be disproportionate”.78 |
The first change to Christmas plans
| 7.31. | On 15 and 16 December 2020, the four nations met to discuss Christmas restrictions, having agreed in late November that up to three households could form an exclusive bubble to meet at home between 23 and 27 December.79 Following those meetings, the legal position on the number of households that could meet remained unchanged in England, Scotland and Wales. This would later change in Wales. |
| 7.32. | On 15 December 2020, Mr Drakeford outlined the Welsh Government’s preference to “reduce the three households that can form a bubble to two”, but he and Ms Sturgeon confirmed their commitment to a four-nations approach if that could be achieved.80 Mr Gove suggested that the “UK Government should share a draft statement which would take account of the particular rules of each jurisdiction”.81 |
| 7.33. | In a four-nations call the following morning, Ms Sturgeon agreed that the substance of the joint statement was “broadly acceptable”.82 Mr Drakeford explained that, while he remained committed to a four-nations approach as far as possible, the Welsh Government would outline its preference for only two households to meet through its public messaging.83 Ms O’Neill highlighted that the Northern Ireland Executive Committee would probably need to discuss the approach on 17 December 2020 and, while there remained a desire to be aligned, this might not prove possible.84 It was agreed that the devolved nations would try to provide feedback on the joint statement by noon that day.85 |
| 7.34. | By lunchtime on 16 December 2020, both Mr Drakeford and Ms Sturgeon announced guidance in Wales and Scotland respectively that was more restrictive than the legal restrictions. Ms Sturgeon recommended to the Scottish public:
“[I]f you do form a bubble, you should not meet up with people in it any more than on one day over that period if possible … Three households is a maximum … But two would be better … In Scotland we already advise an overall limit of 8 people.”86 |
| 7.35. | Mr Drakeford gave a press conference in which he announced that the “position is that only two households should come together to form an exclusive Christmas bubble during the five-day period”.87 He also announced: “[W]e must move to alert level four.”88 Therefore, non-essential retail and places of leisure would close on Christmas Eve, hospitality would close at 18:00 on Christmas Day and a full move to Alert Level 4 would come into force on 28 December.89 Mr Drakeford told the Inquiry that he was also concerned about the other harms arising from restrictions, including harm to businesses and the economy and the impact on children. However, he concluded:
“[I]n the end they will get Christmas back another year and we can do things to restore their education. I cannot give them back their nan.”90 |
| 7.36. | The joint statement was issued on behalf of the UK, Scottish and Welsh governments on the afternoon of 16 December 2020. It stated that a “smaller Christmas is a safer Christmas and a shorter Christmas is a safer Christmas”.91 Ultimately, the Northern Ireland Executive did not sign the joint statement but published its own statement on 21 December, although this was very similar in substance.92 There was a suggestion that Ms O’Neill had “refused to sign at the last minute for political reasons“.93 She denied this, stating that “we were perhaps in a different space”94 |
| 7.37. | At a press conference at about 15:30 that afternoon, Mr Johnson stated that it had been agreed across the UK that the “laws” about Christmas would be the same – three households being able to meet on five days – but that “these are maximums, not targets to aim for”.95 He said that it would be “inhuman” to cancel Christmas but that “people really should think very very hard about coming in under those limits” of three households and five days.96 |
| 7.38. | By 16:28 that afternoon Mr Drakeford had announced that the guidance of a two-household limit would become law in Wales.97 A single adult household would also be permitted to join. Three households could therefore potentially come together. This followed earlier discussions of the Welsh ministers, at which “the balance of views were in favour of making changes to the regulations to align with guidance”.98 |
| 7.39. | Both the Welsh and Scottish governments were entitled to make decisions and present public messaging that they felt was in the best interests of their respective nations. However, the messaging on 16 December 2020 regarding the number of households that could come together over the Christmas period is likely to have caused confusion. |
| 7.40. | Moreover, given the data and advice regarding the rapid growth in case numbers in Wales and parts of England, Professor McBride’s concerns in Northern Ireland on 8 December 2020 and the consideration of a planned move to Level 4 in Scotland from 28 December, the decision in all four nations to proceed with Christmas plans and the messaging that accompanied them was overly optimistic and provided false hope. |
| 7.41. | On 16 December 2020, Mr Johnson also chaired Covid-O for the first of the fortnightly tier reviews.99 New daily infections across the UK had risen further to 25,000 and numbers of hospital inpatients were approaching the levels of the peak of the first wave. Professors Whitty and Vallance advised “extreme caution” – “[t]hings were moving fast in the wrong direction” and R was between 1.1 and 1.2 and potentially above 1.4 in some areas.100 Although two areas were moved to a lower tier, London and parts of the south-east (amounting to 70% of England) were moved into Tier 3.101 |
| 7.42. | On 17 December 2020, SAGE confirmed an increase in R with estimates of 1.1 to 1.2 for the UK and 1.1 to 1.3 for England. It said that “the East of England, London, and the South East now have R estimates well above 1″ with “a unique geographical cluster in the South East around Kent”.102 It warned:
“[T]he models are indicating increased transmission in England since the changes on the 2 December 2020. The marked increase in R following these changes may indicate that the November restrictions did not interrupt transmission chains to the same extent as measures taken in the first wave.”103 SAGE noted its concern that cases were continuing to rise in Tier 3 and advised that additional interventions might need to be considered in order to keep R below 1. It advised: “[E]ven a short period of epidemic growth could lead to the number of new hospital admissions in early January 2021 exceeding the peak of the first wave.”104 As discussed below in paragraphs 7.78 to 7.88, the January 2021 peak would in fact be significantly higher. |
| 7.43. | On 17 December 2020, the Northern Ireland Executive Committee considered post-Christmas restrictions in light of the strain on hospital bed capacity in Northern Ireland.105 Since 21 October 2020, bed occupancy had only been lower than 95% on five days and some hospital sites had been operating consistently above 100% capacity. Despite the restrictions, this exceeded the peak in the first wave.106 Transmission rates indicated a “disappointing response to the two weeks of restrictions” introduced on 27 November 2020.107 The Executive Committee considered whether to: (i) take no action; (ii) introduce restrictions from 2 January 2021; (iii) introduce restrictions from 26 December 2020; or (iv) introduce restrictions from 19 December 2020. Mr Swann cautioned his colleagues:
“[L]eaving the current relaxations in place until 26 December carries significant risk that the measures will be too late to prevent hospital capacity becoming overwhelmed … if the figures illustrated in figure 3 were to come to pass, they are at the very margin of what the health and social care system could cope with. Any unanticipated increase in demand … would push demand beyond capacity.”108 |
| 7.44. | Professors McBride and Young considered that the introduction of restrictions from 19 December 2020 was the optimum approach but that, ultimately, this called for a political judgement by ministers:
“[T]he arguments for 19th v 26th are finely balanced from their professional perspectives, and the key differentiating considerations are wider issues for the Executive to conclude on.”109 |
| 7.45. | The Executive Committee decided to introduce restrictions (in effect, a lockdown) from 26 December for a period of six weeks.110 As Mr Swann observed subsequently, these measures were “more stringent than Tier 4 England”.111 |
| 7.46. | Mr Swann further advised his Executive Committee colleagues that he had not considered any additional closures of schools or made recommendations for education, as the Executive Committee had decided that the continuation of education was a priority.112 However, he did recommend that “measures to limit school opening should be considered” and that Department of Education (Northern Ireland) and Department of Health (Northern Ireland) officials should liaise to:
“develop a package of interventions which will minimise the disruptive impact on educational provision … while also maximising, as far as possible, the impact on the transmission”.113 |
| 7.47. | Ultimately, schools in Northern Ireland closed in the week before Christmas 2020, as usual. The expectation at that point was that schools would reopen in January 2021. |
The response to the Alpha variant
Figure 20a: Tiers in England from 20 December 2020
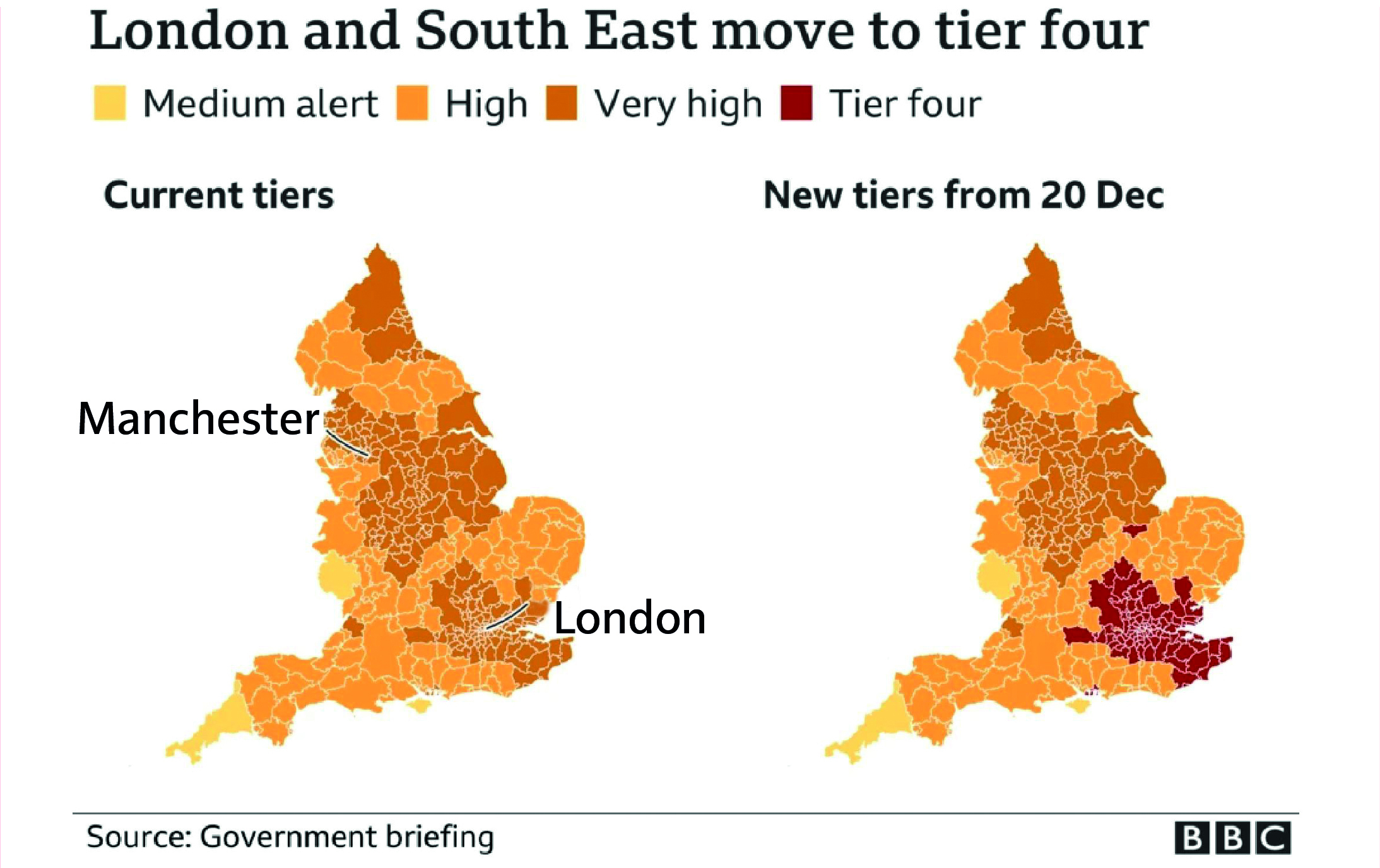
Source: Covid: Christmas Tier-4 heartbreak for Londoners, BBC News, 19 December 2020 (https://www.bbc.co.uk/news/uk-england-london-55380644; INQ000584973)
Figure 20b: Tiers in England from 26 December 2020
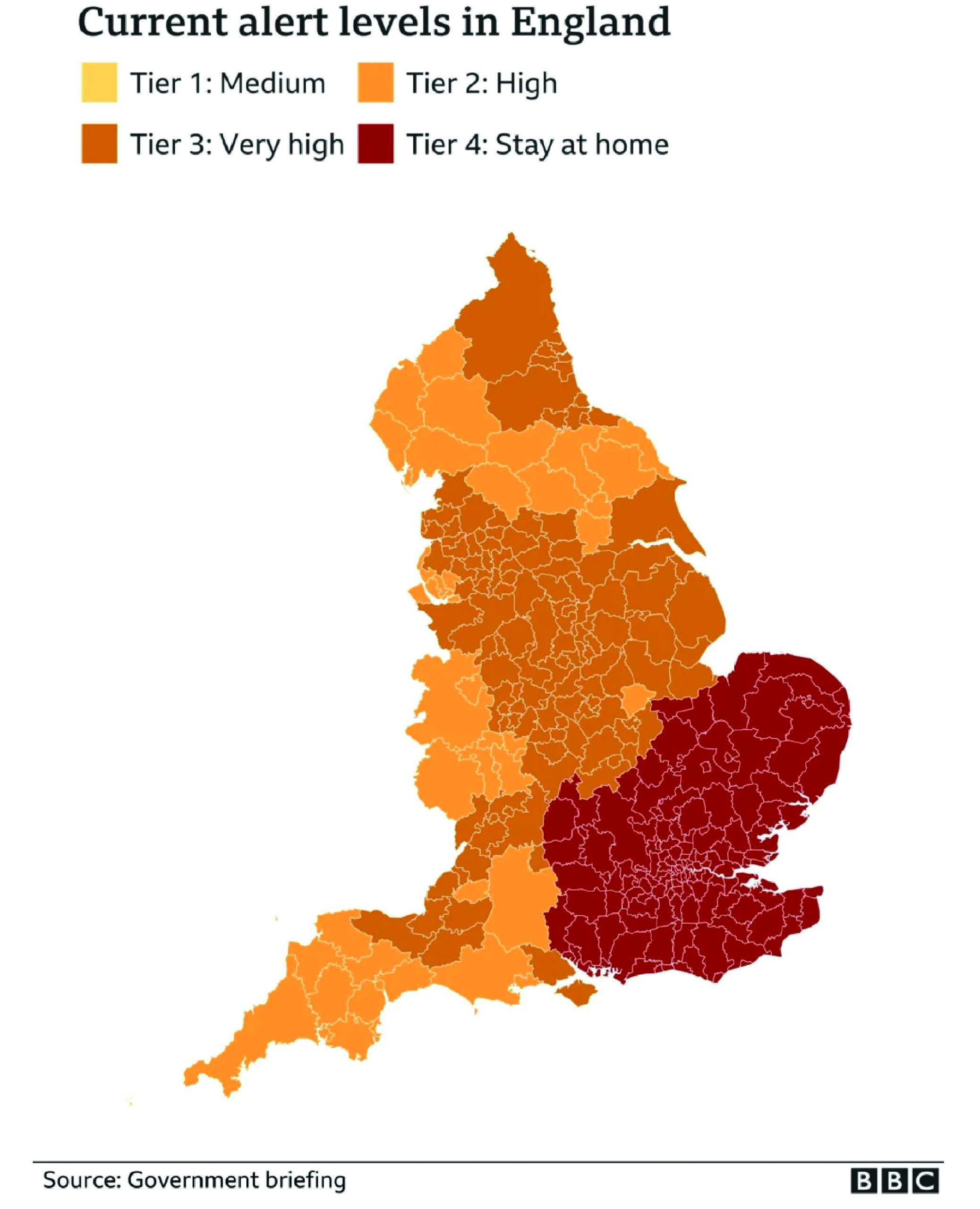
Source: Covid-19: Tougher Covid rules begin for millions in UK, BBC News, 26 December 2020 (https://www.bbc.co.uk/news/uk-55449596; INQ000584969)
Figure 20c: Tiers in England from 31 December 2020
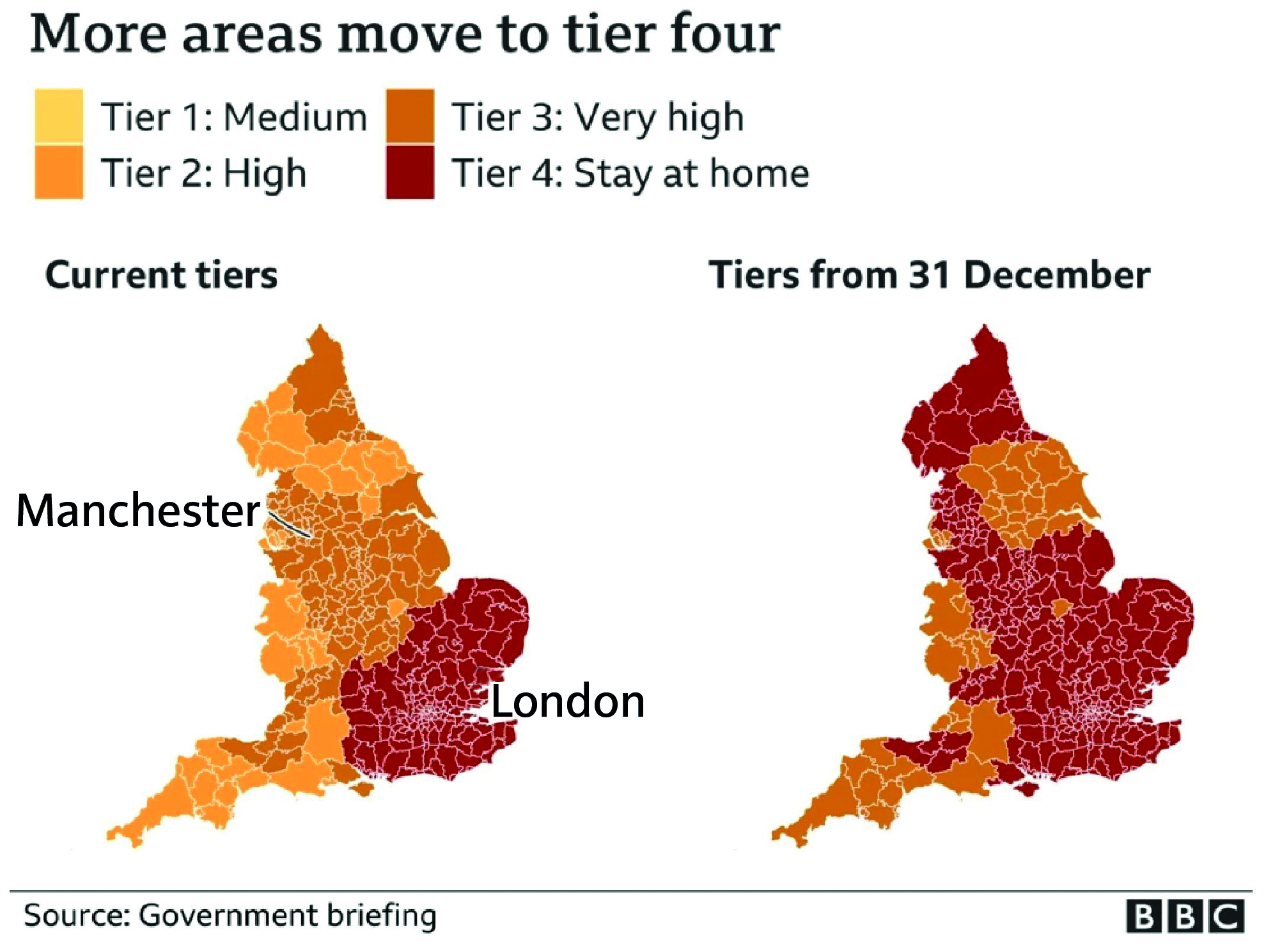
Source: Covid-19: Twenty million in England added to toughest tier of restrictions, BBC News, 30 December 2020 (https://www.bbc.co.uk/news/uk-55489932; INQ000584970)
| 7.48. | On 17 December 2020, UK-wide daily recorded infections had increased to 35,383 – an increase of 69% from 10 December.114 The following day, NERVTAG advised (with “moderate confidence”) that the Alpha variant was substantially more transmissible than other variants, although it was unclear at that stage whether there was any difference in severity.115 |
| 7.49. | Covid-O met on 18 December 2020 and, following overnight reflection, again on 19 December to consider the rising rates of infections, a proposal for new localised Tier 4 restrictions and arrangements for Christmas in England.116 This followed an earlier briefing to Mr Johnson by Professor Whitty and a data update from the Covid-19 Taskforce.117 The factors driving the increase in infections remained unclear, with allocation of tiers, compliance, seasonal impacts and the Alpha variant in the south-east as potential contributors. Covid-O decided to introduce a new Tier 4. |
| 7.50. | Tier 4 was announced publicly by Mr Johnson later on 19 December 2020, to come into effect the following day.118 It applied to a number of areas in southern, eastern and south-eastern England, including London. The restrictions were comparable – with the exception of schools remaining open – to those in the four-week second England-wide lockdown that had ended only a fortnight earlier (see Chapter 6: The second wave, in this volume). Places of communal worship and outdoor sporting activities also remained open. |
| 7.51. | Mr Johnson also stated that there would be:
“total cancellation of the Christmas bubble plans in tier four areas, and in other parts of the country, three households would only be allowed to meet on Christmas Day”.119 This was a significant reversal of the decision made only a few days earlier. |
| 7.52. | The devolved administrations were updated by Mr Gove following the Covid-O meeting and prior to the public announcement.120 |
| 7.53. | The Welsh Government received advice based on modelling on 18 December 2020, which stated:
“[T]he most efficient way to reduce harm from covid-19 and pressure on the NHS is to remove the Christmas relaxation policy and move to alert level 4 restrictions as soon as practically possible (high confidence).”121 The Welsh Government decided on 19 December 2020 to bring forward the implementation of Alert Level 4 restrictions to midnight on that day.122 Its public statement said that the latest evidence about the new variant of coronavirus suggested it was present throughout Wales, and this “new information has required an immediate response”.123 Wales entered a lockdown similar to that of March 2020. Two households could meet on Christmas Day only.124 |
| 7.54. | Mr Drakeford reflected that Christmas 2020 was “the most difficult period of decision-making in the whole of the pandemic for the Welsh Government”.125 The Welsh Government had adopted a similar strategy to the rest of the UK of trying to preserve some prospect of relaxation of the rules for a number of days over the Christmas period. However, Dr Tracey Cooper, Chief Executive of Public Health Wales from June 2014, suggested that the Welsh Government should have acted earlier on the advice from Public Health Wales.126 The Welsh Government had clear, unambiguous evidence by 15 December 2020 – including the advice of Public Health Wales and advice on NHS capacity – that a full and immediate move to Alert Level 4 was required. These measures should have been implemented immediately. |
| 7.55. | An emergency Scottish Cabinet meeting took place on 19 December 2020. A briefing paper noted that the current situation in Scotland was less difficult than in the rest of the UK. This created the opportunity to act early to prevent or reduce importation and transmission of the new strain to prevent a “very serious” situation in January.127 During the Cabinet discussion, Ms Sturgeon noted:
“[T]he single most important lesson since the initial outbreak in February 2020 had been that waiting for more data (and therefore delaying action) could have highly negative consequences. It was essential to act quickly, decisively and preventatively.”128 Subsequently, Ms Sturgeon announced that relaxation of restrictions would be limited to Christmas Day, with the whole of mainland Scotland placed under Level 4 rules from Boxing Day. Travel between Scotland and the rest of the UK would “not be legal”.129 She also announced that schools in Scotland would remain open until the Christmas holidays. She said that there would be an extended holiday period for the majority of pupils until 11 January 2021 and thereafter remote learning until at least 18 January.130 |
| 7.56. | The Northern Ireland Executive Committee met on 20 December. Four potential cases of the Alpha variant had been identified.131 Handwritten notes record Professor McBride as having said: “[V] little doubt – variant already in NI.”132 It was agreed that Mr Swann would bring forward a paper on whether a ban on travel from “Great Britain and from the Republic of Ireland to Northern Ireland” should be introduced.133 Ultimately, ministers decided to issue travel guidance rather than a ban.134 Mr Swann indicated that, in light of the emerging situation in relation to the new variant, he did not believe that a return to school as normal in January was “a sustainable position”.135 |
| 7.57. | The following day, the Northern Ireland Executive published its statement on Christmas arrangements.136 Christmas bubbling would be reduced to one day only on a date between 23 and 27 December 2020.137 It advised:
“The safest place for everyone to spend Christmas is in their own home and people are strongly advised to stay at home for Christmas. Those who feel they need to meet with their bubble should keep it as small as possible, as close to home as possible and keep the visit short.”138 Matters would be kept under review by the Executive Committee due to the “rapidly evolving situation” and ministers were to consider the issue of restricting travel at their next meeting.139 |
Figure 21: Revised rules for Christmas 2020
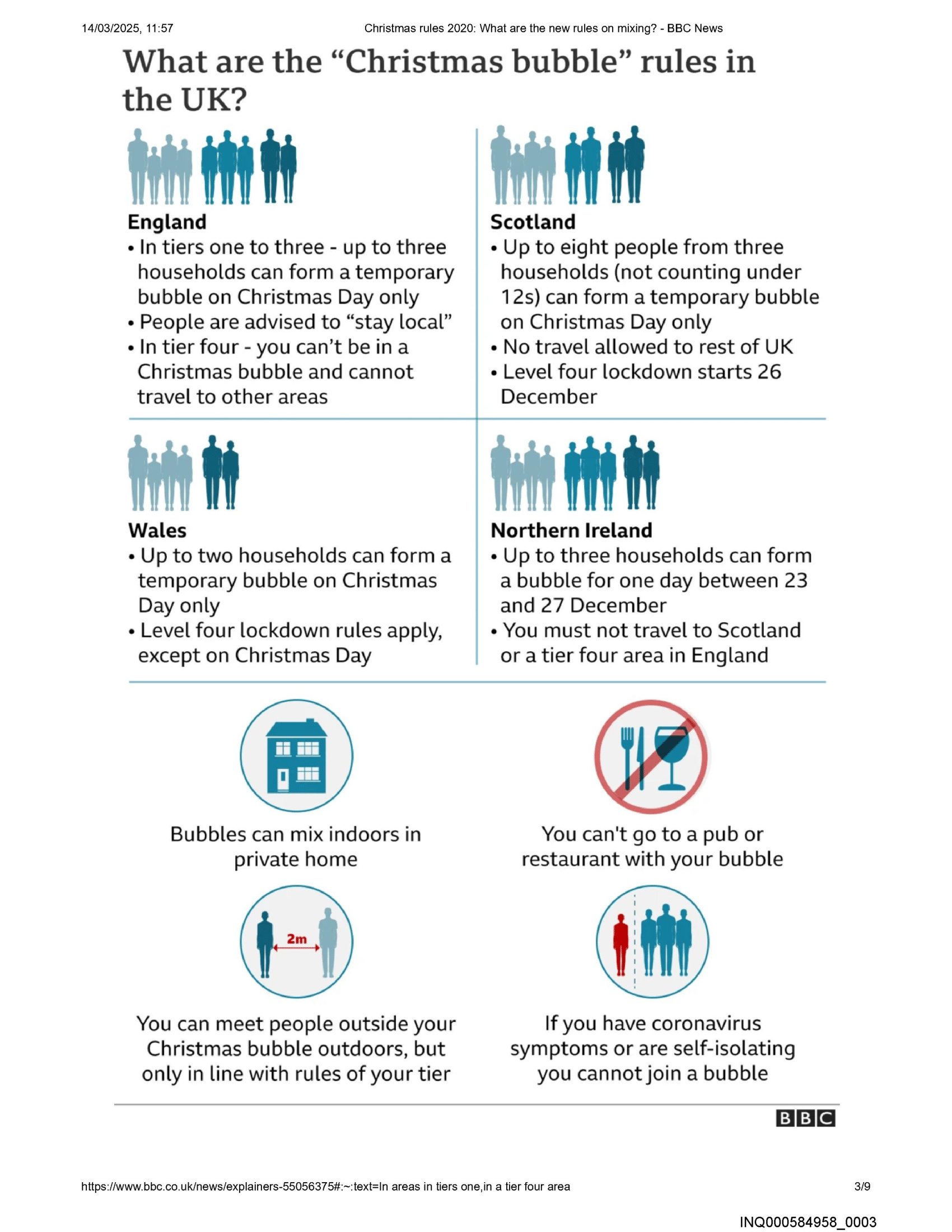
Source: Christmas rules 2020: What are the new rules on mixing?, BBC News, 23 December 2020 (https://www.bbc.co.uk/news/explainers-55056375; INQ000584958)
| 7.58. | Despite the introduction of Tier 4 and the increased restrictions on Christmas gatherings, R continued to rise in England, with a resulting increase in infections, hospitalisations and deaths.140 On 21 December 2020, NERVTAG concluded that it had “high confidence that [Alpha] can spread faster than other SARS-CoV-2 virus variants currently circulating in the UK”.141 |
| 7.59. | By 22 December 2020, R was estimated to be 1.1 to 1.3 for the UK as a whole, based on lagged data, with England at 1.1 to 1.4, Scotland 0.9 to 1.1, Wales 1.0 to 1.3 and Northern Ireland 0.8 to 1.1. The situation in the community in England was reflected in sharp rises in infections and positive cases in care homes.142 SAGE advised that Tier 4 – the equivalent of the November second lockdown with schools remaining open – was highly unlikely to result in reducing R below 1, given the transmissibility of the Alpha variant.143 It was not known whether a return to the measures in the first lockdown, with schools closed, would be sufficient to do so. |
| 7.60. | With Wales already, in effect, in lockdown, the Technical Advisory Cell confirmed the following day that the Alpha variant was circulating in Wales.144 |
| 7.61. | At the Cabinet meeting on 22 December 2020, Ms Sturgeon again noted that there was:
“a strong risk that growth in the new variant would be exponential unless significant new mitigations were put in place”.145 She announced that Level 4 restrictions, planned for all mainland areas of Scotland from Boxing Day, might need to be strengthened in order to contain the Alpha variant.146 |
| 7.62. | A review of the tiers in England took place at Covid-O on 23 December 2020, outside of the regular 14-day review.147 Infection rates were growing. Tier 1 had predictable increases but there was an “extraordinary” increase in case rates in Tier 2 and Tier 4 areas.148 The figures were described as “shocking”, with the situation “sobering and depressing”.149 Covid-O decided to escalate significant swathes of England into higher tiers.150 |
| 7.63. | The position changed so rapidly as a result of the Alpha variant that Mr Johnson could only hope “that as the days went on, the data would suggest some improvement and we might be able to save Christmas”.151 It seems likely that he also did not wish to be seen to be reversing his earlier decision. However, given the lack of adequate planning by the UK government for an increase in infections brought about by a variant of concern and a failure to take timely and decisive action, his hope was in vain. |
| 7.64. | The epidemiological picture was clear, and SAGE and other scientific advisers were advising that further intervention was required. Tier 4 restrictions were insufficient and stricter restrictions were required, including over Christmas. |
| 7.65. | Mr Hancock announced that the changes to the tiers would come into effect on Boxing Day, commenting: “[W]e have learnt that when it’s a matter of when, not if we take action. It is better to act sooner.”152 The appreciation of a need for a tougher approach appeared to be dawning on the UK government. However, this did not deter it from maintaining a tiers-based approach. |
| 7.66. | By 29 December 2020, 10 days after Wales moved to Alert Level 4, the number of hospital beds occupied in Wales was higher than at the peak of the first wave in April 2020.153 |
| 7.67. | Covid-O was convened on 29 December 2020. In a report prepared that day, Professor Vallance outlined, in stark terms, the choices between continuing to escalate through the tiers system while keeping schools open, or seeking to get ahead of the curve with more expansive Tier 4 measures and delays to the reopening of secondary schools.154 At the meeting, Mr Johnson noted:
“The situation facing the country was grim … There were around 53,000 cases reported in the UK that day and hospital inpatients had exceeded the peak of the first wave.”155 |
| 7.68. | Professor Vallance advised that, in reality, there were more likely to be in the region of 100,000 new cases. The NHS was under increasing pressure, with at least one hospital declaring a critical incident. Three hundred beds were to be made available in Nightingale hospitals.156 He also said that decisions “on schools would be important”, as the highest prevalence rates were among children of secondary school age, followed by children of primary school age.157 Professor Vallance recorded in his evening notes that Mr Gove argued that “all of England should go into Tier 4″, with other ministers arguing for greater restrictions and, conversely, no restrictions at all.158 Covid-O decided to continue with the tiers.159 Mr Johnson commented:
“Putting the whole country into tier four was premature, many areas had worked hard to suppress the virus and it did not seem fair to put in place stricter measures than needed.”160 |
| 7.69. | A further Covid-O meeting was held to discuss schools later on 29 December 2020.161 On 28 December, Professor Whitty had described the Department of Education’s plans for reopening schools, in light of the substantial new threat, as “absolutely minimalist”.162 He advised that if, in four weeks’ time, cases were rising significantly (causing death rates to rise and putting the NHS under significant pressure) then that would likely require, at short notice, the closure of all education. Professor Whitty noted that this prospect was not reflected in the advice and that ministers needed to be aware that there would have to be a Plan B if the current Plan A did not have “sufficient bite”.163 By contrast, Gavin Williamson MP (later Sir Gavin Williamson), Secretary of State for Education from July 2019 to September 2021, sought the reopening of schools at the Covid-O meeting on 29 December. This was because he had “an exceptionally high level of confidence” that the UK government could deliver the necessary testing in all secondary schools (with students getting two tests in the two weeks from 11 January and a proposal for weekly testing thereafter).164 For primary schools, rollout of testing for all teachers and serial testing of contacts would take place from the week commencing 18 January 2021.165 However, the scientific advice was that modelling of the new variant suggested that it was very unlikely its spread would be controlled without closing schools.166 Mr Johnson concluded:
“It was essential to move heaven and earth to get children back, and overwhelmingly primary children should go back on 4 January. But in some areas, cases were so high that some primary schools would have to delay the start of term.”167 The plan was that primary schools would be closed on a borough-by-borough basis within London and the south-east.168 For secondary schools across England, children in examination years would return from 11 January 2021 and other pupils from 18 January.169 The majority of primary schools would reopen on 4 January. This was announced in Parliament by Mr Williamson. In Module 8: Children and young people, the Inquiry is exploring this sequence of events in greater detail. |
| 7.70. | By 29 December 2020, R had risen to between 1.4 and 1.8 in Northern Ireland.170 Mr Swann stated that, given the considerable pressures on the hospital system and the need to maximise the benefit from the current period of restrictions, there was a strong case for considering what additional measures could be taken for schools.171 |
| 7.71. | At his press conference on 30 December 2020, Mr Johnson confirmed changes to the reopening of schools, saying:
“[W]e must face the reality that the sheer pace of the spread of this new variant requires us now to take even tougher action in some areas and that does affect schools … In most of England, primary schools will still reassemble next week, as planned for the new term. But, in the areas we have just published today on gov.uk, I am afraid the start of the new term will be delayed until at least January 18, when the latest data on those infection rates will be reviewed. That is because the rate of transmission in these areas is so high, and there’s just such pressure on the local NHS, that extra action is required to control the spread of the virus.”172 |
| 7.72. | Mr Johnson told the Inquiry:
“At the time, I considered that it was right to ease the second lockdown. It had brought the R down and bought time while huge steps had been taken towards mass testing and vaccination. I thought – wrongly as it turned out – that we had done enough, that people could enjoy Christmas with their families and there would be no need for a third lockdown.”173 However, England exited the second lockdown with a far higher prevalence of infections when compared with the point of exit from the first lockdown in April 2020. Along with the potential for emergent variants, this coincided with the start of the most challenging period of the year with regard to the virus, other illnesses and NHS pressures. |
| 7.73. | By 31 December 2020, 78% of the population of England was under the most significant restrictions. These included non-essential shops, hospitality settings (other than for takeaway), beauty salons and hairdressers being closed and people being limited to meeting in a public outdoor place with their household or one other person. In Tier 3 areas, household mixing was banned indoors and in private gardens, although the ‘rule of six’, which permitted social gatherings of up to six people from different households, applied in public spaces. Shops, gyms and personal care services could remain open.174 |
| 7.74. | In the last week of December 2020, the number of cases in Northern Ireland increased “rapidly”, and, by 29 December, R had risen to between 1.4 and 1.8.175 Intensive care unit occupancy had risen to 34, and deaths continued to vary from day to day but were not falling.176 More people died in Northern Ireland between the autumn of 2020 and the peak in January 2021 than in the first wave of the pandemic. Hospital capacity remained under sustained pressure. There is no evidence to suggest that there was any real economic dividend from those periods during which businesses were permitted to reopen. As Mr Swann noted in early January:
“Over the Christmas period, the progress of the epidemic and transmission of the virus was in line with modelling projections which were provided to the Executive before Christmas. Rt has risen to the upper end of modelling limits (close to 1.8) based on current case numbers, and this is reflected in substantial increases in case numbers and test positivity. This largely reflects the impact of behaviours prior to Christmas, and we will expect to see the impact of restrictions during the next 1-2 weeks.”177 |
| 7.75. | By 29 December, data indicated that just under 500 per 100,000 people in Wales had Covid-19 and Covid-19 critical care patients had increased by 24% since 21 December.178 |
Figure 22: UK Covid-19 statistics at 31 December 2020
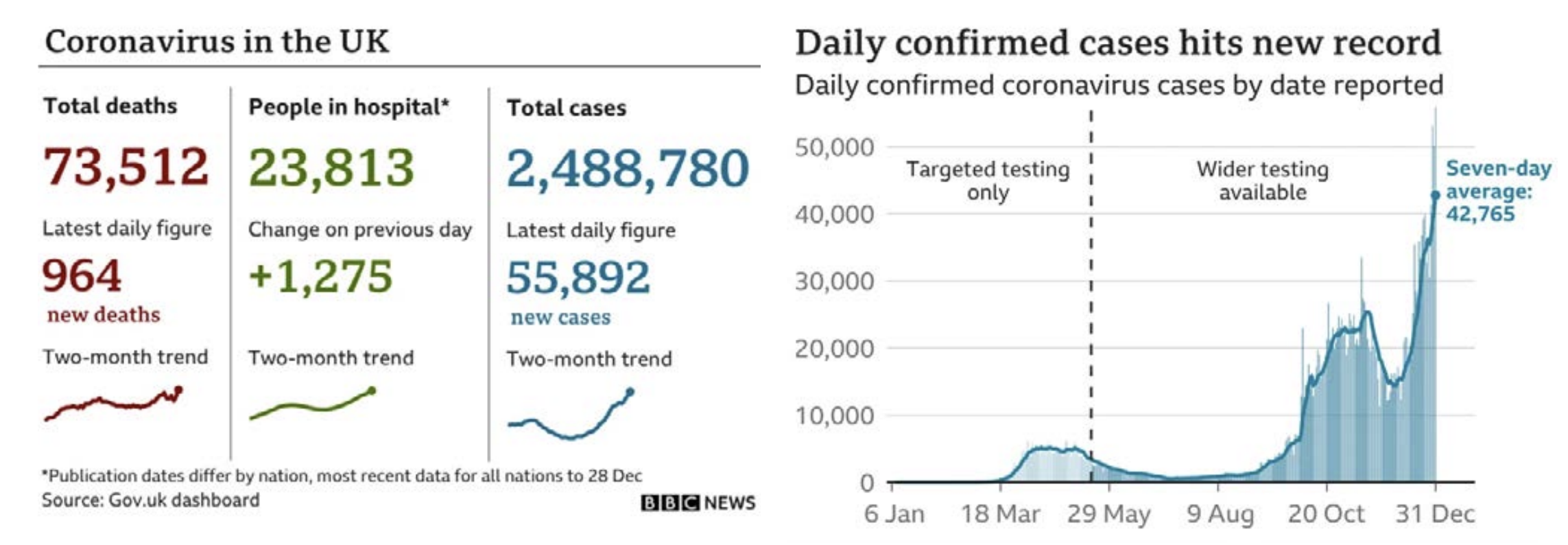
Source: As-it-happened: Millions told to stay home on New Year, BBC News, 31 December 2020 (https://www.bbc.co.uk/news/live/world-55495933; INQ000584956)
| 7.76. | On 31 December 2020, 2,622 positive tests were reported in Scotland.179 At a meeting of the Four Harms Group that day, Professor (later Sir) Gregor Smith, Interim Chief Medical Officer for Scotland from April to December 2020 and Chief Medical Officer for Scotland from December 2020, advised:
“I feel that we are now at the most dangerous point since mid-March. The escalating case numbers cannot be explained purely by people mixing. I expect that cases are going to get a lot worse and rapid growth is a huge concern … We need urgent action. I don’t believe that the current Level 4 restrictions are sufficient to contain the new variant in Scotland.”180 |
| 7.77. | The virus had continued its rapid growth in all four nations. |
Early January 2021
| 7.78. | There was a varied epidemiological picture across the UK in early January 2021:
|
Figure 23: Estimated percentage of the population testing positive for Covid-19 from 1 December 2020 to 16 January 2021
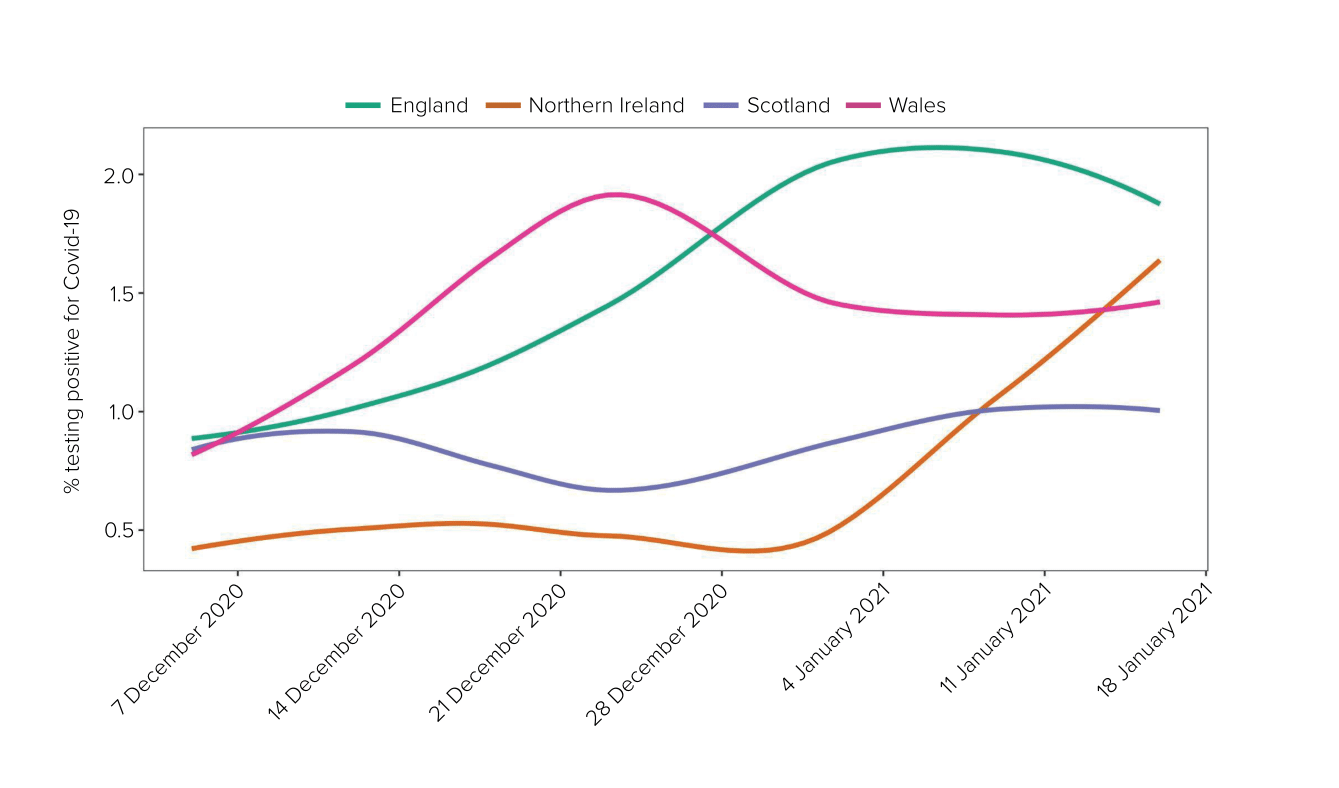
Source: For raw data, see the ONS Coronavirus Infection Survey England 2023 dataset: https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/coronaviruscovid19infectionsurveydata/2023 (modelled estimates, 95% confidence intervals not shown)
| 7.79. | On 4 January 2021, advice from the Joint Biosecurity Centre to the Chief Medical Officers for the four nations concluded:
“[A] COVID-19 epidemic is in general circulation; transmission is rising exponentially; it is almost certain that across much of the UK the NHS will exceed its assumed COVID-19 contingency capacity in the next 21 days; and there is a material risk of healthcare services being overwhelmed in England, Wales and Northern Ireland.”190 In light of this, the Chief Medical Officers and the NHS England Medical Director recommended a move to UK Alert Level 5.191 |
A third lockdown in England
| 7.80. | On 1 January 2021, Mr Gove raised the prospect of delaying all primary schools reopening in London and queried whether reconsideration of other areas was going to be necessary.192 Mr Williamson emphasised the importance of reopening schools as soon as possible and that the decision to close some had been a reluctant one. However, he and Mr Hancock subsequently provided joint advice to close all London primary schools and this was announced later that day.193 |
| 7.81. | The following day, Mr Gove sent a private note to Mr Johnson. He expressed his view that Tier 4 restrictions should be applied across England, the ‘Stay Home’ messaging should be deployed more prominently, secondary schools should be closed until the February 2021 half-term holiday and primary schools should be closed until at least 18 January 2021.194 Mr Johnson said that, while he was grateful to Mr Gove, he did not “think he was telling me anything I did not know”.195 |
| 7.82. | On 4 January 2021, Mr Johnson announced a third lockdown, putting all of England into Tier 4, to come into effect the following day.196 He said:
“By the middle of February, if things go well and with a fair wind in our sails, we expect to have offered the first vaccine dose to everyone in the four top priority groups identified by the Joint Committee on Vaccination and Immunisation … Then I hope we can steadily move out of lockdown, reopening schools after the February half term and starting, cautiously, to move regions down the tiers.”197 |
| 7.83. | The majority of primary schools in England reopened for a single day, 4 January 2021, only to close again to most children the following day. |
Lockdown in mainland Scotland
| 7.84. | The Scottish Cabinet met as scheduled on 4 January 2021.198 John Swinney MSP, Deputy First Minister of Scotland from November 2014 to March 2023, advised:
“With great reluctance, I have concluded that it will be necessary for schools to move to a model of remote learning for all children … It is difficult to predict with any certainty just now the duration of that period, although we might work on the basis of 1 February in the first instance.”199 |
| 7.85. | Ms Sturgeon explained that the new Alpha variant meant that the virus was accelerating rapidly. Tougher restrictions would therefore be required to slow its progress while ensuring that the vaccination programme proceeded as rapidly as possible. No account was taken of the impact of the further lockdown as far as other social and economic harms were concerned.200 The Cabinet decided to close schools and also to place mainland Scotland in lockdown from midnight on 4 January 2021 until the end of January, with people ordered to stay at home except for essential purposes.201 By this point, lockdown was described by Ms Sturgeon as “the only responsible course open to us”.202 The NHS in Scotland now had “less capacity and resilience than the previous spring” and was likely to be overwhelmed within the month without further preventative action.203 Professor Paul Cairney, expert witness on Scottish Government core decision-making and political governance, told the Inquiry:
“[T]he four harms approach was not a strong feature of the emergency decision-making associated with lockdowns … [in] January 2021.”204 |
| 7.86. | Mr Swinney described the period leading up to 4 January 2021 as “a terrifying couple of days” but said:
“The four harms framework acknowledged and accepted that there was one very direct acute harm which is caused by the virus, and the rest of the framework is about trying to help us navigate our way out of those — the difficulties caused by that set of circumstances if we’ve managed to get the acute threat of the pandemic under control, and at that moment on 4 January we were not in that position.”205 The framework ought to have been about assessing all four harms and making decisions that balanced them all, not disregarding Harms 2 to 4 until the recovery phase had been reached. Although the Scottish Government was in an emergency situation in January 2021, it ought to have implemented ways of minimising Harms 2 to 4, even when Harm 1 was the main threat. |
Developments in Wales and Northern Ireland
| 7.87. | In Wales, the original intention was to give schools the flexibility to decide when to reopen in the first two weeks of term.206 However, following the joint Chief Medical Officers’ recommendation to move to Alert Level 5, the Welsh Government confirmed that “it is now clear that a national approach of online learning for the first fortnight of term is the best way forward”.207 On 4 January 2021, it announced that all schools, including primary schools, would not reopen and instead would move to online learning until 18 January, with the exception of children of critical workers, vulnerable learners and those who needed to complete essential exams or assessments.208 The Welsh Cabinet also agreed, on 6 January, to retain Alert Level 4 restrictions.209 Ms Williams confirmed the following day that it would not be possible to fully reopen schools on 18 January as planned.210 |
| 7.88. | When the Northern Ireland Executive Committee met on 4 January 2021, Mr Swann noted that the increase in cases was “in line with extreme modelling”.211 Ms O’Neill emphasised the need for the Executive to be decisive, observing that “[w]e are living worst case scenario”.212 The following day, the Executive Committee agreed a number of changes to school restrictions. All mainstream education providers were to deliver remote learning until the half-term holidays in the middle of February 2021. Vulnerable children and children of key workers were able to attend school for supervised learning and special schools were to remain open.213 Mr Swann advised that cases in those aged over 60 had risen substantially due to inter-generational mixing and set out the expectation that hospital admissions would continue to rise, before peaking in the last two weeks of January “at a level significantly higher than any point in the epidemic to date”.214 The Executive Committee agreed to introduce a number of additional restrictions with effect from 7 January to 6 February, with a review on 21 January.215 |
Continuing restrictions
| 7.89. | On 19 January 2021, following a meeting of the Scottish Cabinet, Ms Sturgeon extended Scotland’s lockdown, including the closure of schools, until mid-February 2021.216 The islands of Barra and Vatersay were moved from Level 3 to Level 4 restrictions from midnight, due to a “significant outbreak”.217 Later in January, the whole of the Western Isles were moved to Level 4 restrictions to control a spike in Covid-19 cases.218 |
| 7.90. | The number of cases in Northern Ireland decreased, although hospital admissions and bed occupancy had not fallen.219 Military medical technicians had been deployed to hospitals to assist with the sustained pressures on the health service.220 On 21 January 2021, Mr Swann advised the Executive Committee that hospitalisations and intensive care unit admissions were the highest since the start of the pandemic. He also stated:
“The learning from wave 2 in the autumn of last year shows that significantly relaxing restrictions when cases continue to be at a high baseline quickly led to an escalating situation where restrictions needed to be introduced to arrest growth of the epidemic.”221 The Executive Committee agreed to extend the restrictions until 5 March 2021.222 |
| 7.91. | On 25 January 2021, the Welsh Cabinet agreed to retain Alert Level 4 restrictions. Dr Atherton told the Welsh Cabinet that the Alpha variant “could be up to 70% more likely to be transmitted”.223 |
February to April 2021
| 7.92. | On 2 February 2021, Mr Swinney advised the Scottish Cabinet that “protective measures would need to be in place for some time to come”.224 The Cabinet approved an extension of the current lockdown arrangements until at least the end of February and agreed provisional plans for a phased return to full-time education from 22 February, subject to confirmation at the next fortnightly review.225 On 17 February, following the next review, Ms Sturgeon announced that there was evidence that vaccination was reducing the number of deaths from Covid-19, with the weekly death rate having fallen for three consecutive weeks, falling in care homes by 62% during that time.226 There was also an expansion of testing from 18 February to include anyone identified as a close contact of someone who had tested positive for Covid-19.227 |
| 7.93. | By 17 February 2021, the first dose of the vaccine had been offered to all those in the four most vulnerable cohorts identified by the Joint Committee on Vaccination and Immunisation (ie elderly care home residents, those 70 and over, the clinically extremely vulnerable – see Chapter 10: Vulnerabilities and inequalities, in Volume II – and frontline health and social care staff) in all four nations.228 On 26 February 2021, the Joint Committee on Vaccination and Immunisation published interim advice on Phase 2 of the Covid-19 vaccination programme, which stated that prioritisation of the vaccine should continue to be age-based.229 |
| 7.94. | On 16 February 2021, Dr Atherton informed the Welsh Cabinet that the situation was improving in Wales and that over 780,000 people had now had their first dose of a vaccine. However, there remained a need for caution, due to uncertainty surrounding new variants and the impact that vaccines would have on transmission rates. The Cabinet agreed to retain Alert Level 4 restrictions, although four people from two households could meet outdoors provided that social distancing was observed.230 |
| 7.95. | Northern Ireland remained subject to restrictions throughout February 2021. While the number of Covid-19-positive inpatients had been on a downward trend since the peak of 834 in mid-January 2021, it remained high. On 15 February, Northern Ireland had 436 Covid-19-positive inpatients and 59 confirmed Covid-19-positive inpatients in intensive care units.231 The number of Covid-19-positive inpatients was not expected to fall below 150 before the middle of March 2021.232 |
| 7.96. | On 18 February 2021, a paper from the Department of Health (Northern Ireland) observed that the high number of patients requiring critical care would:
“continue to constrain the ability of critical care to provide dedicated support for complex elective surgery in the coming weeks. These severe pressures mean that surgery, including urgent and cancer surgery, has been adversely affected. As current pressures are likely to be sustained for many weeks … it is inevitable that there will be a detrimental impact on patient treatment and potentially patient outcome as a consequence.”233 The paper set out various modelling projections and cautioned that there was: “a material risk of significant adverse implications if there is even a minor misjudgement in the scale and speed of any relaxation of the restrictions”.234 Noting that the position remained “fragile“, the conclusion of the Department of Health (Northern Ireland) was that relaxations of the restrictions at this juncture would be premature.235 On 18 February 2021, the Executive Committee decided to extend the current restrictions until 1 April 2021, with a further review to take place on or before 18 March 2021.236 |
Roadmaps to the removal of restrictions
Figure 24: UK Covid-19 statistics at 15 February 2021
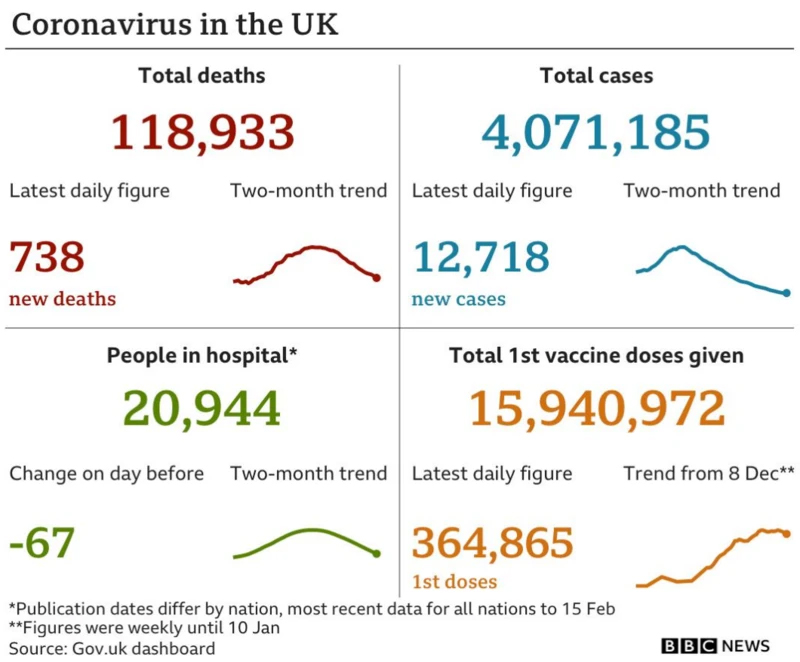
Source: ‘England restrictions to be lifted in stages – PM’, BBC News, 17 February 2021 (https://www.bbc.co.uk/news/live/uk-56095941; INQ000591890)
| 7.97. | On 19 February 2021, the Welsh Government announced that its lockdown would continue for a further three weeks.237 It also published an updated plan, entitled Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown, which set out a “more cautious approach to coming out of lockdown” given the emergence of new variants.238 It identified a number of priorities when it was possible to move to Alert Level 3:
|
| 7.98. | Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown did not assign dates for any relaxations but confirmed that the Welsh Government would take a similar approach to the one it took from May 2020, namely “careful steps and evaluating the impact before making further changes”.240 Decisions would be taken in line with the three-week review cycle but might also be taken outside of that process to ensure “restrictions are only in place for as long as they are needed”.241 |
| 7.99. | The COVID-19 Response – Spring 2021 roadmap for England was published on 22 February 2021, having been endorsed by the UK Cabinet earlier that day.242 Advice from SAGE, including by SPI-M-O, informed its development.243 It was a detailed, public-facing document with clear objectives. It outlined four tests that would inform when the UK would move to the next step:
“1. The vaccine deployment programme continues successfully. 2. Evidence shows vaccines are sufficiently effective in reducing hospitalisations and deaths in those vaccinated. 3. Infection rates do not risk a surge in hospitalisations which would put unsustainable pressure on the NHS. 4. Our assessment of the risks is not fundamentally changed by new Variants of Concern.”244 Restrictions were to be removed at the same time across England, owing to the relatively uniform spread of the virus. There were indicative “no earlier than” dates for each of the four steps, which were five weeks apart in order to assess data on the impact of the previous step and one further week’s notice of changes.245 Step 1 was to take effect on 8 March 2021, by which time cohorts 1 to 4 would have received protection from their first dose of the vaccine, with further limited changes on 29 March to allow families to meet outdoors as most schools broke up for the Easter holidays. |
Figure 25: Steps in the COVID-19 Response – Spring 2021 roadmap, February 2021
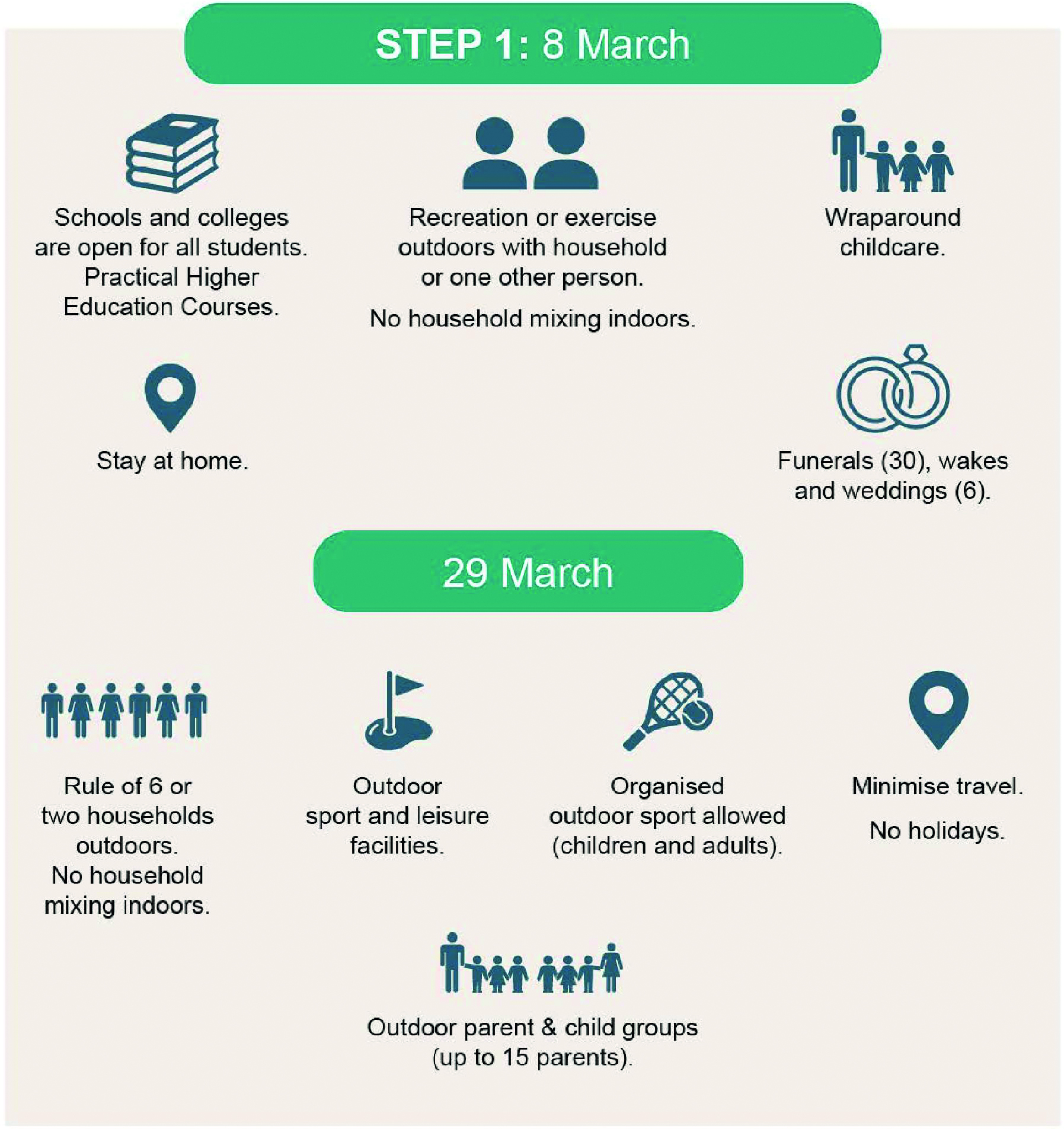

Source: COVID-19 Response Spring 2021, HM Government, February 2021, pp31, 37, 40, 43 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
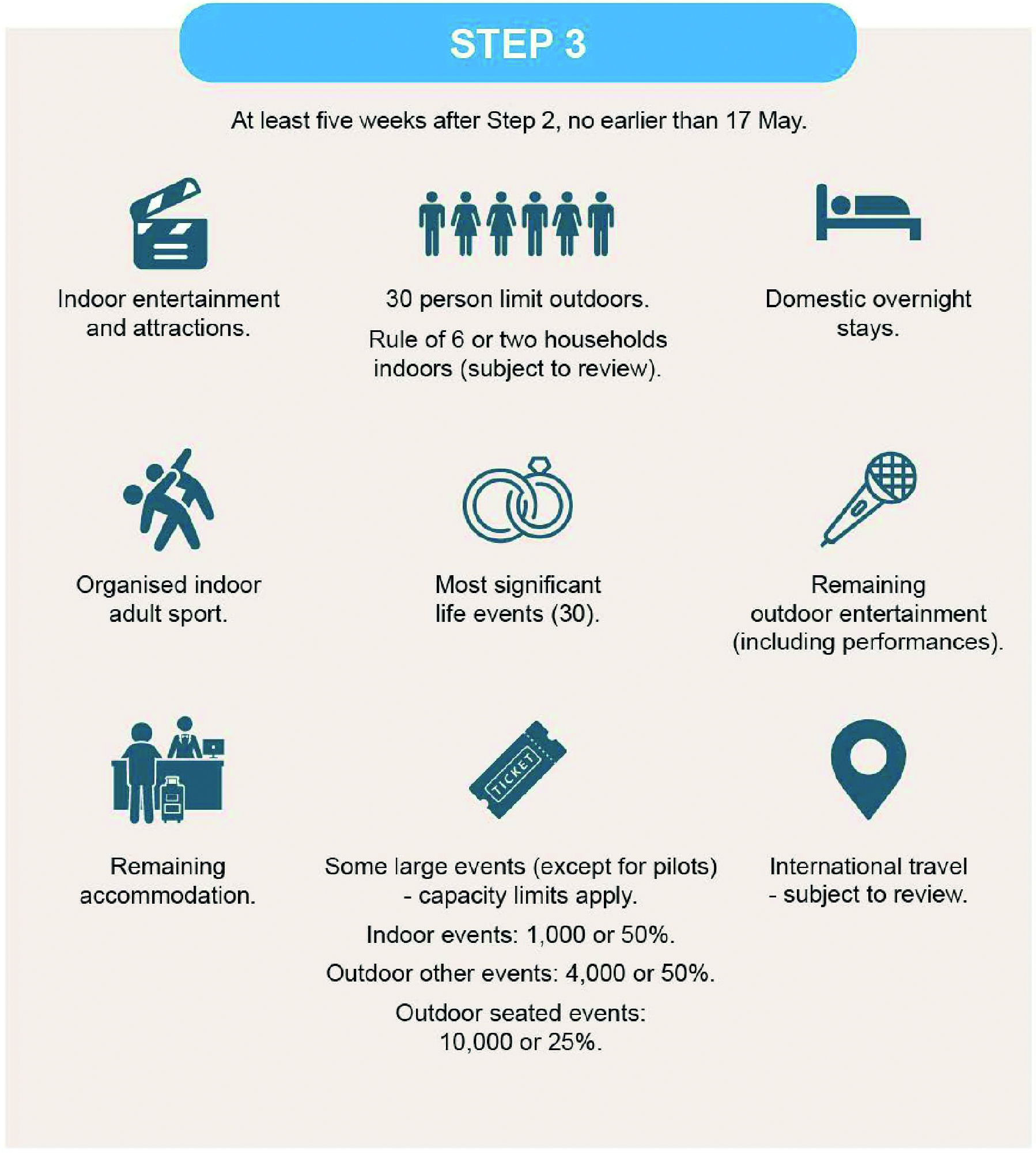
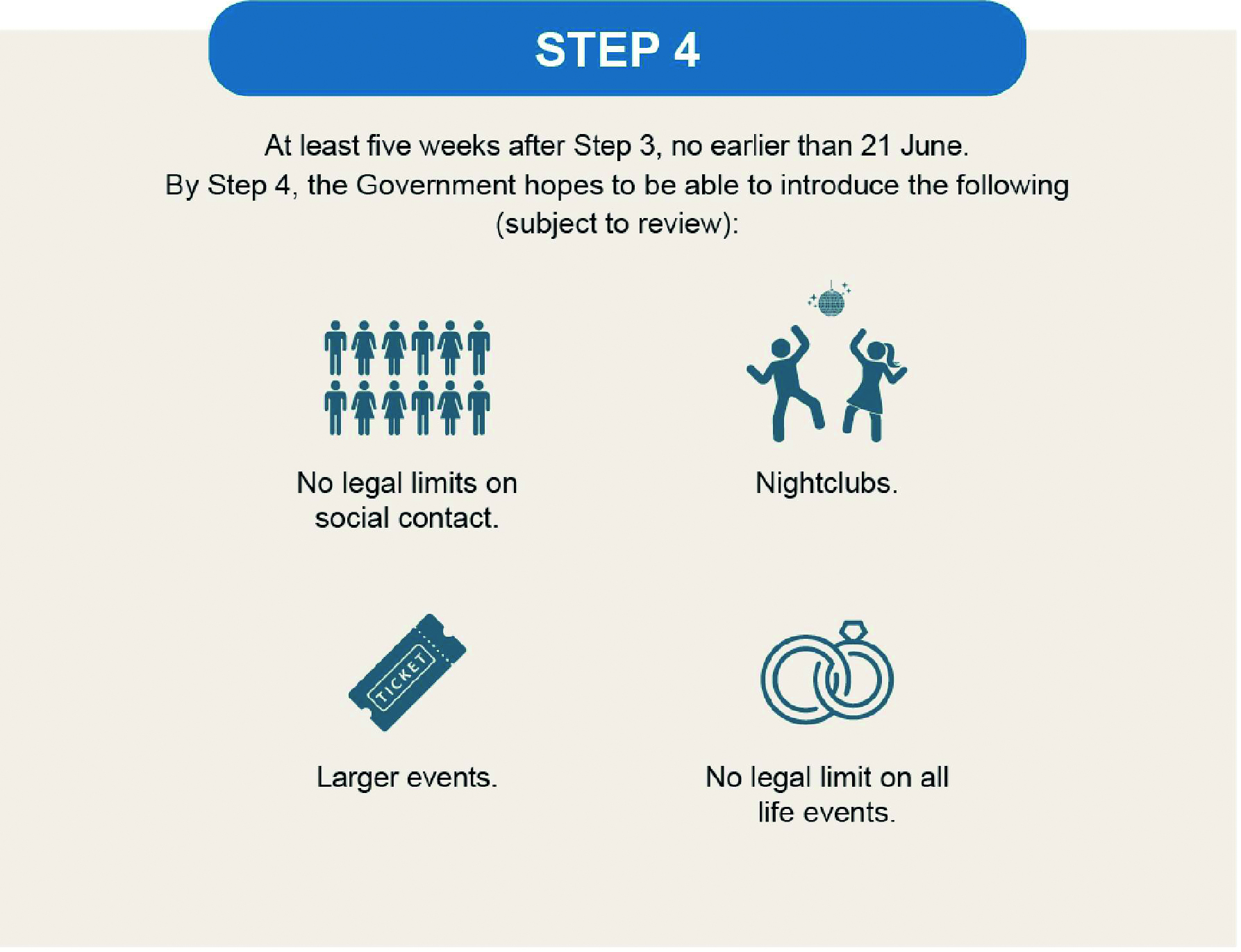
Source: COVID-19 Response Spring 2021, HM Government, February 2021, pp31, 37, 40, 43 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
| 7.100. | On 23 February 2021, COVID-19: Scotland’s Strategic Framework Update was approved by the Scottish Cabinet and published later that day.246 It set out the broad order of priority for reopening and the conditions that needed to be met to start lifting restrictions and linked the removal of restrictions to the prevalence of the virus and coverage of the vaccine rollout, without providing indicative dates.247 It envisaged that the remainder of the pandemic could effectively be divided into three phases, although timeframes were not made public “as actual progress is conditional on data”.248 These phases were:
The Four Harms Group, which had contributed to the development of the plan, noted that levels might be retained: “as an outbreak management tool to reflect potential risk from variation in population immunity (both natural as vaccine effect wears off and due to impact of new variants with vaccine escape properties)”.250 |
| 7.101. | The Northern Ireland Executive published Moving Forward: The Executive’s Pathway out of Restrictions on 2 March 2021.251 It involved a slower relaxation of restrictions and was not linked to specific dates, but set out a five-phase approach to nine pathways, including ‘Home and Community’, ‘Education and Young People’ and ‘Hospitality’.252 However, the pathway was “undermined within hours” of its publication by public criticism from other ministers.253 Naomi Long MLA, Minister for Justice in Northern Ireland from January 2020 to October 2022, told the Inquiry that this was “damaging to our being able to promote it publicly as a cohesive and clear approach”.254 |
Figure 26: Extract from Moving Forward: The Executive’s Pathway out of Restrictions
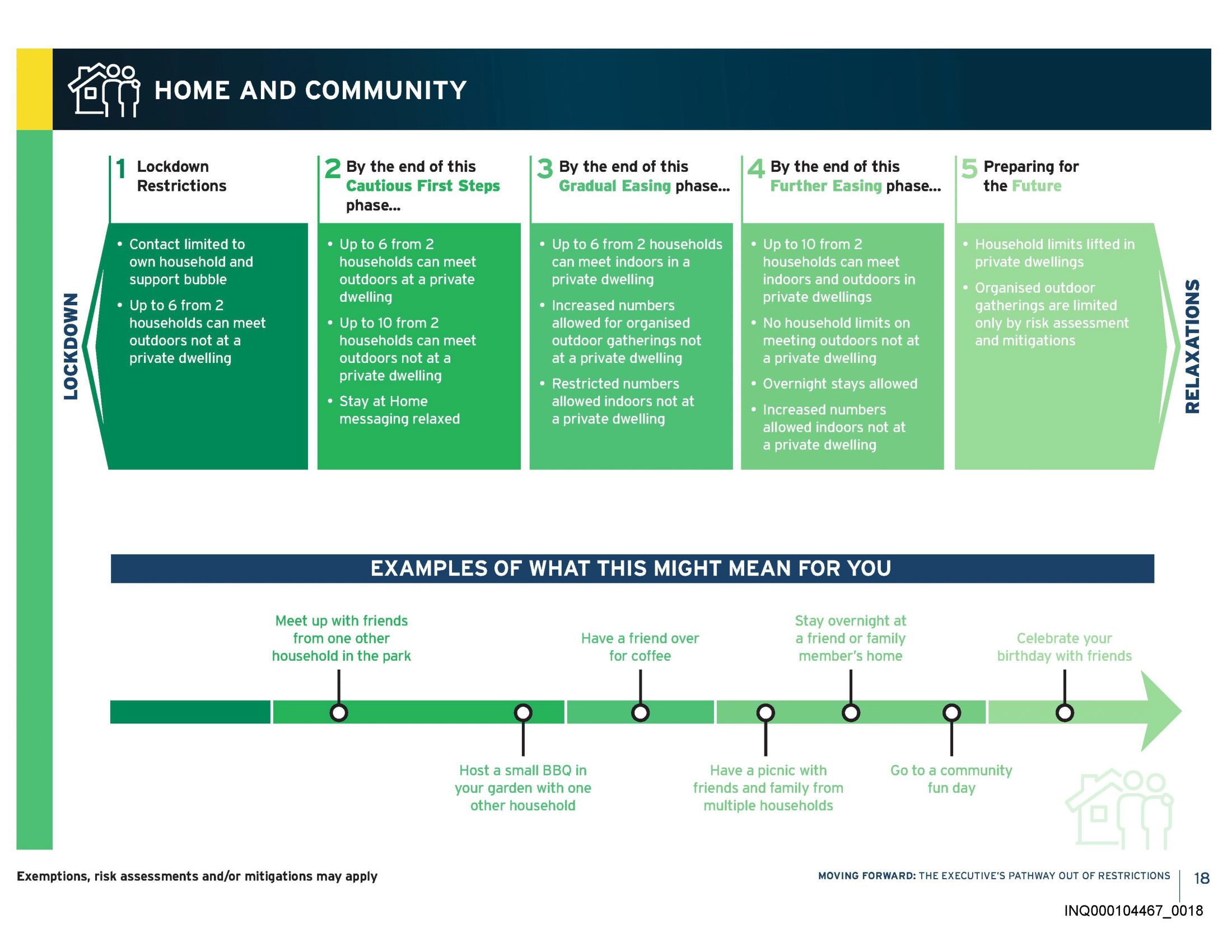
Source: Moving Forward: The Executive’s Pathway out of Restrictions, Northern Ireland Executive, 2 March 2021, p18 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/executives-pathway-out-of-restrictions.pdf; INQ000104467)
| 7.102. | Vaccines featured prominently in plans – for example, being described as “at the heart of the UK Government’s strategy to manage COVID-19“.255 Ms Sturgeon, in her foreword to COVID-19: Scotland’s Strategic Framework Update, explained that vaccines:
“will reduce illness and deaths from COVID and also, ultimately, when a high proportion of our population has been vaccinated, let us return to a more normal way of living”.256 Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown adopted a more cautious tone, noting that the Welsh Government was still “learning about the effectiveness of vaccines”, but if they worked “as hoped” they would, along with other measures, “enable us to move out of the alert level four measures”.257 Similarly, in Northern Ireland, Moving Forward: The Executive’s Pathway out of Restrictions recognised that no vaccine was “100% effective” and “not everyone will be vaccinated” and cautioned: “[T]his might mean that some measures to limit transmission are still needed for some time even after all adults have been offered a vaccine.”258 |
Figure 27: Vaccine doses across the UK, as at 21 February 2021
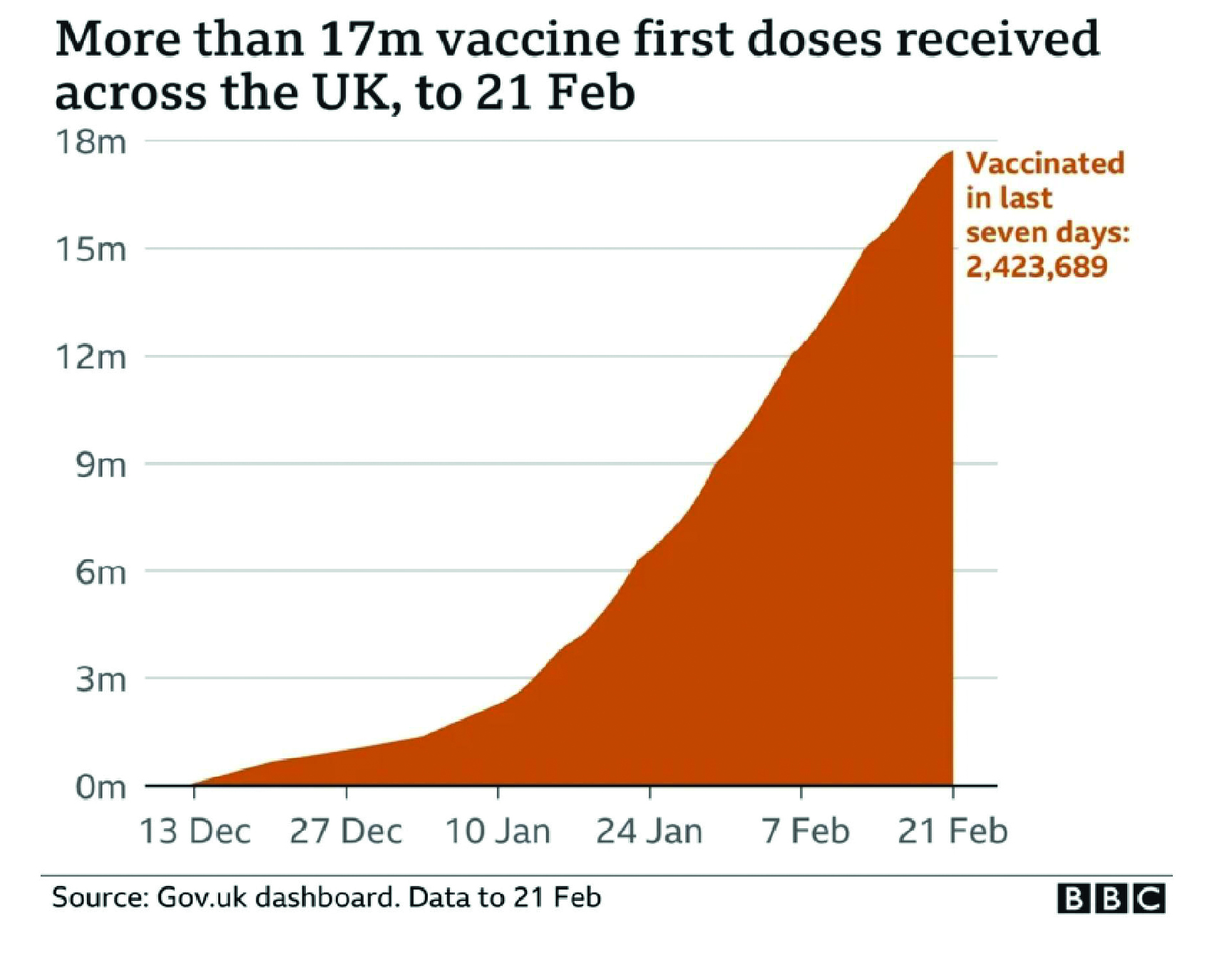
Source: We’re travelling on a one-way road to freedom” – PM’, BBC News, 22 February 2021 (https://www.bbc.co.uk/news/live/uk-56149494?page=2; INQ000591903)
Tentative steps to remove restrictions
| 7.103. | By early March 2021, the restrictions in Northern Ireland were leading to reduced case numbers. In the seven days between 5 and 11 March, 1,311 individuals tested positive for Covid-19 in Northern Ireland.259 As at 10 March, the number of Covid-19-positive inpatients in Northern Ireland stood at 169.260 The intensive care unit position was a matter for concern. The standard funded position was for 72 intensive care unit beds – as at 10 March, the number of critically ill patients stood at 91 (of whom 29 were Covid-19 positive).261 The rolling average number of daily deaths in Northern Ireland was 4 on 9 March.262 |
| 7.104. | By 3 March 2021, the most recent estimate of R in Wales was between 0.7 and 0.9.263 The number of people in hospital with confirmed Covid-19 continued to decrease but remained high with “approximately 600 beds occupied”.264 Intensive care unit occupancy continued to decrease, but there were still two to four Covid-19 admissions daily. The Welsh Cabinet decided that, from 13 March, the stay at home restrictions would be replaced with ‘Stay Local’ rules.265 This would allow people to travel within their local area, using a distance of five miles as a “rule of thumb”.266 This reflected earlier advice from Dr Atherton that “a staggered approach to the lifting of restrictions would allow better monitoring of the impact on the spread of the virus on the specific easements”, particularly in light of the Alpha variant.267 A few days later, the Welsh Government published the Coronavirus Control Plan: Revised Alert Levels in Wales (March 2021), which stated:
“[A] wholesale jump from alert level four to alert level three at this time would have endangered the significant progress we have made to date.”268 |
| 7.105. | On 16 March 2021, among discussions about the lifting of the ‘stay at home’ order, it was proposed to the Scottish Cabinet that, during the pre-election period, there would be a need for continuing collective decision-making at ministerial level in relation to the management of the pandemic.269 It was agreed, provided decisions remained consistent with Scotland’s Strategic Framework Update and the indicative timetable, to delegate decision-making to the First Minister, supported by the Gold Command group of key ministers and input from the Chief Medical Officer for Scotland, as well as other advisers and officials. The Cabinet agreed, and it was later announced that the stay at home order would be lifted on 2 April 2021 in favour of a ‘Stay Local’ order within local authority areas.270 Hairdressers and garden centres would reopen on 5 April. It was planned that the Stay Local order would be lifted on 26 April in favour of a ‘Stay within Scotland’ order, at which time gyms and tourist accommodation would also be allowed to reopen. |
| 7.106. | In Northern Ireland, the eighth review of the restrictions took place on 16 March 2021. An Executive Paper from Mr Swann noted that, in the period after 16 March, there were two events that would traditionally see increased social contact: St Patrick’s Day (17 March) and Easter (4 April) and cautioned:
“We do not wish to undo the good work following the difficult recovery from the relaxations around the Christmas period, and to ease the restrictions now before Easter, allowing inter-household gatherings would put us at significant risk of falling further backwards.”271 While the Executive Committee concluded that the existing restrictions should remain in place, it agreed a limited number of amendments.272 From 1 April 2021, ten people from two households (including children under twelve) could undertake outdoor sporting activities and up to six people from two households could meet outdoors in a private dwelling (increasing to ten people from two households from 12 April). Subject to ratification by the Executive Committee in the week after the Easter weekend, it was agreed that the requirement to ‘stay at home unless you have a reasonable excuse’ provision would be removed.273 |
| 7.107. | On 26 March 2021, the Welsh Government announced the removal of the Stay Local provisions in favour of an “interim all-Wales travel area … Until 12 April, people will need a reasonable excuse to travel into or out of Wales.”274 By 29 March, the Welsh Cabinet was told that the number of people with confirmed Covid-19 in hospital was continuing to decrease.275 The Cabinet agreed that non-essential retail and close-contact services would reopen from 12 April. The evidence presented to the Cabinet justified this easing of restrictions. |
| 7.108. | The UK government announced that, from 9 April 2021, everyone in England would be able to access two rapid Covid-19 tests twice a week.276 The Welsh Government announced that a similar initiative would be in place for those unable to work from home, along with an extension of testing in schools to all pupils in Year 7 and above from 16 April.277 The Scottish Government confirmed that lateral flow testing would be made available to everyone in Scotland from 26 April.278 On 28 April, the Department of Health (Northern Ireland) announced a further expansion of the workforce testing programme to organisations with 10 or more employees who could not work from home.279 |
| 7.109. | On 12 April 2021, the UK government implemented Step 2 of its COVID-19 Response – Spring 2021 roadmap, which included reopening non-essential retail, personal care and outdoor hospitality settings, as well as allowing for an increased number of visitors to care homes (from one to two).280 |
| 7.110. | In Scotland, the Stay Local order was lifted early on 16 April 2021, allowing up to six people from six different households to meet outside again. People were still not permitted to stay overnight outside their council area, and the advice remained for people to shop within their council area whenever possible.281 |
| 7.111. | On 19 April 2021, Dr Atherton advised that the situation in Wales was “stable” and that “[t]esting data indicated that positivity for Covid-19 continued to fall slowly, but consistently”.282 The Welsh Cabinet agreed that outdoor hospitality would reopen from 26 April, and its intention was a complete move to Alert Level 3 by 3 May 2021.283 |
| 7.112. | By 23 April 2021, R in Scotland had fallen for the first time in four weeks, dropping from between 0.8 and 1.0 to between 0.7 and 0.9.284 A few days later, all of Scotland moved to Level 3 restrictions as non-essential shops, gyms, swimming pools, pubs, restaurants and cafes were allowed to reopen, while travel between Scotland and the rest of the UK was also permitted again.285 |
| 7.113. | On 30 April 2021, a number of relaxations took effect in Northern Ireland, as agreed by the Executive Committee on 15 April:
|
The situation by the end of April 2021
| 7.114. | The exit strategies were based on data rather than aspiration.287 According to Professor Stephen Reicher, Professor of Psychology at the University of St Andrews, the relevant data were gathered according to World Health Organization principles. Notably, these principles were whether transmission was controlled and whether there was health service capacity to identify, test and treat all cases and also to trace and quarantine contacts. In addition, minimising outcome risks to the most vulnerable, the existence of preventative measures in workplaces, managing import and export of cases from hotspots and the participation of communities in the transition were all invoked.288 |
| 7.115. | The UK government’s COVID-19 Response – Spring 2021 roadmap was a good example of a well-defined and comprehensive strategy, with clear aims and objectives. It adopted the data-driven approach, marked with caution and incremental and monitored relaxation of restrictions. It sought to:
“balance health, including mental health, economic and social factors and how they disproportionately impact certain groups, as well as epidemiological evidence”.289 However, it explicitly stated that the dates for easing restrictions were “wholly contingent on the data and … subject to change”.290 It provided clear information to the public and explained the rationale for the steps, along with setting out the evidential basis or scientific advice. For example, it explained: “The sequencing of easing will be driven by the evidence on sources of transmission. Outdoor activity has been prioritised because the likelihood of COVID-19 transmission is substantially lower in the open air than indoors. This restores more freedom to people more quickly while minimising the impact on transmission.”291 This allowed the public and businesses to plan ahead. When plans changed, there was a readily understandable rationale or metric, with clear criteria for the next step. This assisted in avoiding the mixed messages and reactive decision-making that had marked much of 2020 and the early part of 2021. |
| 7.116. | In Wales, Mr Gething believed that the Welsh Government struck the right balance in the easing of restrictions in 2021.292 In his view:
“[T]he vaccination gave us headroom to make choices but, dealing with the level of uncertainty about the level of population protection it provided, going through February and March in particular, we really did have to take seriously advice we’d had, taking account of where we were before Christmas.”293 The Welsh Government was right to adopt a cautious approach to lifting restrictions, given the uncertainties about varieties and the impact of vaccines, in the period from January to April 2021. |
| 7.117. | In Northern Ireland, some ministers expressed concerns that the pace of removing restrictions was too slow. Diane Dodds MLA, Minister for the Economy in Northern Ireland from January 2020 to June 2021, suggested that the length and complexity of the Executive’s review process was threatening the continued existence of businesses already heavily affected by the ongoing restrictions.294 Edwin Poots MLA, Minister for Agriculture, Environment and Rural Affairs in Northern Ireland from January 2020 to October 2022, referred to the “glacial pace of easing”.295 Ms O’Neill explained:
“The time built in between key steps and relaxations was to allow for decisions to be properly informed by the health, community, and economic data and to see the real time impact of the steps taken on the prevalence of the virus. This allowed us to use the ongoing modelling and take risk-based decisions on next steps. The Executive did not want to be driven by dates but by the evidence. A commitment was made to only keep restrictions in place as long as necessary.”296 Ms O’Neill considered that this “represented an appropriate, balanced, and reasonable strategy for reopening society”.297 The Inquiry agrees. The Northern Ireland Executive’s cautious approach to the relaxation of restrictions at this time was the right one, given the uncertainty about the emerging Alpha variant and the fragility of Northern Ireland’s health service in this period. The caution demonstrated that lessons had been learned from what happened when restrictions were removed too swiftly in late 2020. |
Winter lockdowns and exit plans
| 7.118. | The Inquiry accepts that restrictions were lifted carefully and proportionately throughout the spring of 2021 across the UK, and to this extent lessons had been learned from previous lockdowns. This meant that the four governments were better placed at the end of April 2021 to balance recovery from the effects of the virus and restrictions with the continued need to manage the direct and indirect harms of the virus and emerging variants. |
| 7.119. | However, all four governments of the UK might have avoided the need for any further lockdown or exit strategy in the first place had the lessons of 2020 about the spread of the virus and its devastating consequences been learned earlier and more comprehensively. |
| 7.120. | It was clear at the beginning of December 2020 that R was likely to be above 1 in parts of the UK – especially Wales and some regions of England – and that the various measures that had been implemented had failed to reduce the relatively high level of incidence. Yet, all four governments decided to proceed with plans to relax (to varying degrees) the restrictions over Christmas. This decision was understandable but unjustified given the exponential growth of the virus. It gave rise to false hope. |
| 7.121. | It compounded their failure to take the necessary steps to get the virus under control. All four governments bear responsibility for the hurried and chaotic descent into further and immensely damaging lockdowns. |
- ‘Landmark moment as first NHS patient receives COVID-19 vaccination’, NHS England, 8 December 2020 (https://www.england.nhs.uk/2020/12/landmark-moment-as-first-nhs-patient-receives-covid-19-vaccination; INQ000237370)
- INQ000248853_0086 para 5.239
- INQ000248853_0086 paras 5.239-5.240
- INQ000128575_0002
- ‘COVID-19 vaccine authorised by medicines regulator’, Department of Health and Social Care, Department for Business, Energy and Industrial Strategy and Alok Sharma, 2 December 2020 (https://www.gov.uk/government/news/covid-19-vaccine-authorised-by-medicines-regulator; INQ000479077)
- ‘Landmark moment as first NHS patient receives COVID-19 vaccination’, NHS England, 8 December 2020 (https://www.england.nhs.uk/2020/12/landmark-moment-as-first-nhs-patient-receives-covid-19-vaccination; INQ000237370)
- ‘First COVID-19 vaccinations in Scotland take place’, Scottish Government, 8 December 2020 (https://www.gov.scot/news/first-covid-19-vaccinations-in-scotland-take-place; INQ000369703)
- ‘Written Statement: COVID-19 vaccine launch in Wales’, Vaughan Gething, Minister for Health and Social Services, Welsh Government, 8 December 2020 (https://www.gov.wales/written-statement-covid-19-vaccine-launch-wales; INQ000321010); INQ000083199_0002
- INQ000276549_0001
- INQ000276549_0001
- INQ000276552_0002
- INQ000304288_0002-0003
- INQ000305410_0001; INQ000065642_0020
- INQ000214798_0003 para 12
- INQ000089081_0001
- INQ000089081_0001
- INQ000273901_0300
- ‘Huge crowds of Christmas shoppers fill UK cities despite virus fears’, Metro, 12 December 2020 (https://metro.co.uk/2020/12/12/huge-crowds-of-christmas-shoppers-fill-uk-cities-despite-virus-fears-13742852; INQ000625229); ‘COVID-19: Christmas shoppers flood high streets in return after lockdown’, Sky News, 5 December 2020 (https://news.sky.com/story/covid-19-christmas-shoppers-flood-high-streets-in-return-after-lockdown-12152120; INQ000625228)
- INQ000048788_0003-0004
- See Part 3 of The Health Protection (Coronavirus Restrictions) (No. 4) (Wales) Regulations 2020 (https://www.legislation.gov.uk/wsi/2020/1219/contents/made) as updated on 4 December 2020.
- INQ000066405_0002
- INQ000066405_0002
- INQ000129910_0008
- INQ000056303_0001-0002
- INQ000056303_0001-0002
- INQ000065642
- INQ000208784_0001 paras 1-2
- INQ000276549_0001
- INQ000065642_0008-0009
- INQ000048501_0004 para 16(iv)
- ‘Ministers outline new Covid-19 measures’, The Executive Office, 4 December 2020 (https://www.executiveoffice-ni.gov.uk/news/ministers-outline-new-covid-19-measures; INQ000276553)
- INQ000065956_0008; Ian Young 7 May 2024 195/11-21; INQ000286272_0001; see also Ian Young 7 May 2024 194/6-9
- INQ000286272_0002
- INQ000452486_0019 para 64
- INQ000418976_0039-0040 para 127
- INQ000539016_0124
- INQ000048917_0001
- INQ000350062
- INQ000120576_0002 para 12
- INQ000048793_0002 para 1.4
- INQ000350062
- INQ000088967_0005
- INQ000251645_0152-0153 para 8.85
- INQ000251645_0152-0153 para 8.85
- INQ000214799; ‘Scotland’s toughest Covid restrictions to be eased’, BBC News, 8 December 2020 (https://www.bbc.co.uk/news/uk-scotland-55230778; INQ000357854)
- INQ000120576_0001-0002 paras 1-2; see also paras 8-9, 11
- INQ000120576_0001 para 9
- INQ000120576_0001 para 2
- INQ000350065
- INQ000362237_0077-0078 paras 266-268; INQ000350063
- INQ000048793
- INQ000048794
- INQ000236513_0001; INQ000153472
- INQ000120390_0002
- INQ000120390_0006 para 4.12
- INQ000229912_0002
- COVID-19: Framework for Decision Making – Assessing the Four Harms of the Crisis, Scottish Government, 11 December 2020 (https://www.gov.scot/publications/covid-19-framework-decision-making-assessing-four-harms-crisis/documents; INQ000131028); see also Chapter 5: Exit from lockdown
- INQ000056302_0001-0002 para 3
- INQ000056302_0001 para 2
- INQ000228507_0002; INQ000321019
- Michael Gravenor 1 March 2024 185/12-187/4
- INQ000228579
- INQ000048501_0004, 0007-0008 para 16(iv)
- INQ000251645_0153 para 8.87
- INQ000072127. Mr Gething was first informed of the Alpha variant on 14 December 2020 (INQ000391237_0086 para 341).
- INQ000091065
- INQ000054310
- INQ000091065_0006-0007
- INQ000273901_0309
- ‘UK Chief Medical Officers’ statement on the self-isolation period: 11 December 2020′, Department of Health and Social Care, 11 December 2020 (https://www.gov.uk/government/news/uk-chief-medical-officers-statement-on-the-self-isolation-period-11-december-2020; INQ000203967)
- Coronavirus Control Plan: Alert Levels in Wales – A Guide to Restrictions, Welsh Government, December 2020, p4 (https://www.gov.wales/sites/default/files/publications/2020-12/coronavirus-control-plan-alert-levels-in-wales.pdf; INQ000227576)
- INQ000321015; INQ000321016
- INQ000321014; INQ000350099
- INQ000056304_0002
- INQ000056304_0002
- Vaughan Gething 11 March 2024 189/7-190/17
- INQ000214800_0003 para 10
- INQ000214800_0007 para 24(n)
- ‘Joint statement on UK-wide Christmas arrangements from the UK Government and Devolved Administrations’, Cabinet Office, 24 November 2020 (https://www.gov.uk/government/news/joint-statement-on-uk-wide-christmas-arrangements-from-the-uk-government-and-devolved-administrations; INQ000086871); INQ000199004; INQ000199006. Ms Foster represented Northern Ireland at the meeting on 15 December – she was joined by Ms O’Neill on 16 December.
- INQ000199004_0002-0003
- INQ000199004_0003-0004
- INQ000199006_0001
- INQ000199006_0002; see also INQ000539017_0019
- INQ000199006_0002
- INQ000199006_0003
- Coronavirus (COVID-19) update: First Minister’s speech – 16 December 2020′, Scottish Government, 16 December 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-tuesday-16-december-2020; INQ000354143)
- INQ000350118_0003; ‘Covid-19: Welsh Government update’, BBC News, 16 December 2020 (https://www.bbc.co.uk/news/live/uk-wales-55331021 (see 12.25 Breaking news); INQ000584971_0015-0016)
- INQ000350118_0001
- INQ000350118
- Mark Drakeford 13 March 2024 170/14-173/9, 172/22-24
- ‘Joint statement on staying safe at Christmas from the UK Government, Scottish Government, and Welsh Government’, Cabinet Office, 16 December 2020 (https://www.gov.uk/government/news/joint-statement-on-staying-safe-at-christmas-from-the-uk-government-scottish-government-and-welsh-government; INQ000220411)
- INQ000412903_0057 para 171; ‘Executive statement on Christmas arrangements’, The Executive Office, 21 December 2020 (https://www.executiveoffice-ni.gov.uk/news/executive-statement-christmas-arrangements; INQ000214870)
- INQ000412903_0057 para 172
- Michelle O’Neill 14 May 2024 177/2-12; see also INQ000095177_0001; INQ000418976_0063 para 206; INQ000426982_0020 paras 74-75
- ‘Prime Minister’s statement on coronavirus (COVID-19): 16 December 2020’, Prime Minister’s Office and Boris Johnson, 16 December 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-16-december-2020; INQ000086622)
- INQ000548311
- ‘Covid: Two household limit at Christmas to be made law in Wales’, BBC News, 16 December 2020 (https://www.bbc.co.uk/news/uk-wales-55336452; INQ000584975); The Health Protection (Coronavirus Restrictions) (No. 5) (Wales) Regulations 2020, Schedule 6 (https://www.legislation.gov.uk/wsi/2020/1609/schedule/6/made)
- INQ000350127
- INQ000091076
- INQ000091076_0007
- INQ000091076_0007
- INQ000075736_0004 paras 9-10
- INQ000075736_0004 para 11
- INQ000075736_0004 para 13
- INQ000065641
- INQ000065641_0001 para 5
- INQ000065641_0004 para 16
- INQ000065641_0006 para 33
- INQ000065641_0006 para 36
- INQ000048504. This included enhanced restrictions between 20:00 and 06:00 from 26 December 2020 to 2 January 2021, with an accompanying power for the Police Service of Northern Ireland to direct people home where they were engaged in prohibited activity, or intended to be so engaged.
- INQ000065740_0001
- INQ000065641_0008 para 46
- INQ000065641_0010 para 57(d)
- INQ000091081_0004
- INQ000128575
- INQ000091087; INQ000091082; INQ000251913; INQ000091091; INQ000091279
- INQ000217008; INQ000255836_0165 para 581
- ‘Prime Minister’s statement on coronavirus (COVID-19): 19 December 2020’, Prime Minister’s Office and Boris Johnson, 19 December 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-19-december-2020; INQ000086623)
- INQ000091091_0008
- INQ000199009
- INQ000321022; INQ000321023_0001
- INQ000048803
- ‘Written Statement: Alert level four restrictions’, Mark Drakeford, First Minister, Welsh Government, 19 December 2020 (https://www.gov.wales/written-statement-alert-level-four-restrictions; INQ000216561)
- INQ000389184_0086 para 301
- Mark Drakeford 13 March 2024 170/14-173/9
- INQ000276282_0030-0031 paras 126-127
- INQ000232740_0002
- INQ000232744_000 para 12
- ‘Covid: Lockdown looms as Scotland tightens Christmas rules’, BBC News, 19 December 2020 (https://www.bbc.co.uk/news/uk-scotland-55379632; INQ000357747); ‘New guidance issued for the festive period’, Scottish Government, 19 December 2020 (https://www.gov.scot/news/new-guidance-issued-for-the-festive-period; INQ000369718)
- ‘Coronavirus (COVID-19) update: First Minister’s speech – 19 December’, Scottish Government, 19 December 2020 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech; INQ000354144)
- INQ000276560
- INQ000065740_0007
- INQ000022460_0002 para 5
- INQ000276561_0002; INQ000065742_0022
- INQ000276560_0003
- ‘Executive statement on Christmas arrangements’, The Executive Office, 21 December 2020 (https://www.executiveoffice-ni.gov.uk/news/executive-statement-christmas-arrangements; INQ000214870)
- ‘Executive statement on Christmas arrangements’, The Executive Office, 21 December 2020 (https://www.executiveoffice-ni.gov.uk/news/executive-statement-christmas-arrangements; INQ000214870)
- ‘Executive statement on Christmas arrangements’, The Executive Office, 21 December 2020 (https://www.executiveoffice-ni.gov.uk/news/executive-statement-christmas-arrangements; INQ000214870)
- ‘Executive statement on Christmas arrangements’, The Executive Office, 21 December 2020 (https://www.executiveoffice-ni.gov.uk/news/executive-statement-christmas-arrangements; INQ000214870)
- INQ000184012_0001, 0013-0014
- INQ000212114_0003
- INQ000091280_0001
- INQ000075511_0 para 11
- INQ000310630_0001
- INQ000214801_0003 para 10
- ‘Covid in Scotland: Scottish level four rules “may be strengthened”‘, BBC News, 22 December 2020 (https://www.bbc.co.uk/news/uk-scotland-55414617; INQ000357665)
- INQ000091116
- INQ000091116_0005
- INQ000091116_0006-0007
- INQ000091116_0009
- INQ000255836_0168 para 590
- ‘Health and Social Care Secretary’s statement on coronavirus (COVID-19): 23 December 2020’, Department of Health and Social Care, 23 December 2020 (https://www.gov.uk/government/speeches/speech-on-coronavirus-restriction-tiers-vaccines-and-testing; INQ000086620); INQ000091282
- INQ000022520_0004 para 3.2
- INQ000063113
- INQ000091113_0004
- INQ000091113_0006-0007
- INQ000091113_0007
- INQ000273901_0336
- INQ000091113_0008
- INQ000091113_0008
- INQ000091117_0001-0003
- INQ000063116_0003
- INQ000063116_0003
- INQ000091117_0004
- INQ000091117_0004
- INQ000091117_0007-0008
- INQ000091117_0008-0009
- INQ000091117_0008-0009; INQ000075513_0002
- INQ000091117_0004; ‘Prime Minister’s statement on coronavirus (COVID-19): 30 December 2020’, Prime Minister’s Office and Boris Johnson, 30 December 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-30-december-2020; INQ000075739)
- INQ000276566_0001
- INQ000276566_0002
- ‘Prime Minister’s statement on coronavirus (COVID-19): 30 December 2020’, Prime Minister’s Office and Boris Johnson, 30 December 2020 (https://www.gov.uk/government/speeches/prime-ministers-statement-on-coronavirus-covid-19-30-december-2020; INQ000075739)
- INQ000255836_0161 para 569
- Covid-19: Twenty million in England added to toughest tier of restrictions’, BBC News, 30 December 2020 (https://www.bbc.co.uk/news/uk-55489932; INQ000584970_0002); INQ000088942_0002
- INQ000276566_0001
- INQ000382097_0001
- INQ000276571_0001 para 3
- INQ000022520_0004 paras 3.3-3.4
- ‘Covid in Scotland: Cases hit record high for third day in a row’, BBC News, 31 December 2020 (https://www.bbc.co.uk/news/uk-scotland-55497996; INQ000357524)
- INQ000232954_0002. The Four Harms Group had responsibility for discussing direct health harm, broader health harm, social harm and economic harm, as well as potential responses, to inform advice for decision-making (INQ000280694).
- INQ000022521_0002 para 2.3
- INQ000022521_0002-0003 para 2.6
- INQ000382104_000
- Moving Forward: The Executive’s Pathway out of Restrictions, Northern Ireland Executive, 2 March 2021, p6 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/executives-pathway-out-of-restrictions.pdf; INQ000104467)
- INQ000136711_0010
- INQ000238826_0143 para 431
- INQ000238826_0143 para 431
- INQ000232688_0008
- INQ000232688_0008
- INQ000072317
- ‘COVID-19 alert level: Update from the UK Chief Medical Officers’, Department of Health and Social Care, 4 January 2021 (https://www.gov.uk/government/news/covid-19-alert-level-update-from-the-uk-chief-medical-officers; INQ000234691); INQ000072317
- INQ000217071
- INQ000075513; Contingency Framework – Implementation Guidance, Department for Education, 1 January 2021 (https://s4s.wandsworth.gov.uk/Pages/Download/E82BB4DF-3F5E-4C2C-B904-C402E83E7EEF/PageSectionDocuments; INQ000075516); INQ000259848_0064-0065 para 127; ‘Contingency framework implemented across London boroughs’, Department for Education, Department of Health and Social Care and Gavin Williamson, 1 January 2021 (https://www.gov.uk/government/news/contingency-framework-implemented-across-london-boroughs; INQ000075740)
- INQ000184013
- INQ000255836_0172-0173 para 598
- ‘Prime Minister announces national lockdown’, Prime Minister’s Office and Boris Johnson, 4 January 2021 (https://www.gov.uk/government/news/prime-minister-announces-national-lockdown; INQ000065415)
- ‘Prime Minister’s address to the nation: 4 January 2021’, Prime Minister’s Office and Boris Johnson, 4 January 2021 (https://www.gov.uk/government/speeches/prime-ministers-address-to-the-nation-4-january-2021; INQ000086664)
- INQ000214456
- INQ000232688_0002 para 10
- INQ000214456_0004 para 13; INQ000274154_0057 para 163
- ‘Scotland in lockdown’, Scottish Government, 4 January 2021 (https://www.gov.scot/news/scotland-in-lockdown; INQ000357841)
- INQ000339033_0130 para 366
- INQ000214456_0002-0003 paras 4-5
- INQ000274154_0057 para 163
- John Swinney 30 January 2024 175/4-177/2
- INQ000353851_0001
- INQ000353851_0001
- INQ000353851_0001
- INQ000022521
- INQ000022521
- INQ000065709_0002
- INQ000065709_0003
- INQ000207210_0002; INQ000235720_0058-0059 para 118
- INQ000276571_0002 para 6
- INQ000276571_0010-0013; INQ000207210_0002
- ‘Covid in Scotland: Schools to stay closed as lockdown extended’, BBC News, 19 January 2021 (https://www.bbc.co.uk/news/uk-scotland-55718133; INQ000357660)
- INQ000078427_0011 para 55
- ‘Covid in Scotland: Western Isles goes into lockdown’, BBC News, 30 January 2021 (https://www.bbc.co.uk/news/uk-scotland-highlands-islands-55857072; INQ000357716; INQ000369751)
- INQ000391432_0001
- INQ000400872; INQ000421542
- INQ000065591_0012-0013 para 34
- INQ000048510_0004 para 12(iv)
- INQ000129912_0003 para 3.5
- INQ000214460_0003 para 12
- INQ000214460_0005-0006 para 19; ‘Covid: Scottish schools to start phased return this month’, BBC News, 2 February 2021 (https://www.bbc.co.uk/news/uk-scotland-55904466; INQ000357764)
- ‘Covid in Scotland: Deaths falling as vaccine “having an effect”‘, BBC News, 17 February 2021 (https://www.bbc.co.uk/news/uk-scotland-scotland-politics-56098578; INQ000357539)
- ‘Close contacts to be offered testing’, Scottish Government, 17 February 2021 (https://www.gov.scot/news/close-contacts-to-be-offered-testing; INQ000571289)
- Moving Forward: The Executive’s Pathway out of Restrictions, Northern Ireland Executive, 2 March 2021, p8 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/executives-pathway-out-of-restrictions.pdf; INQ000104467); INQ000354293_0003; INQ000584968; INQ000591900
- JCVI Interim Statement on Phase 2 of the COVID-19 Vaccination Programme: 26 February 2021, Joint Committee on Vaccination and Immunisation, updated 13 April 2021 (https://www.gov.uk/government/publications/priority-groups-for-phase-2-of-the-coronavirus-covid-19-vaccination-programme-advice-from-the-jcvi/jcvi-interim-statement-on-phase-2-of-the-covid-19-vaccination-programme; INQ000354488_0003-0004)
- INQ000057770_0003 paras 1.7, 1.9, 1.12
- INQ000065592_0005-0006 para 14
- INQ000065592_0006 para 16
- INQ000065592_0006 paras 15-16
- INQ000065592_0007 para 19
- INQ000065592_0012-0013 para 36
- INQ000048516_0003 para 10(iv)
- ‘Lockdown to continue for further three weeks as pupils return to school’, Welsh Government, 19 February 2021 (www.gov.wales/lockdown-continue-further-three-weeks-pupils-return-school; INQ000584988)
- Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown, Welsh Government, February 2021, p2 (https://www.gov.wales/sites/default/files/publications/2021-02/coronavirus-control-plan-alert-levels-in-wales-coming-out-of-lockdown.pdf; INQ000081858)
- Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown, Welsh Government, February 2021, p13 (https://www.gov.wales/sites/default/files/publications/2021-02/coronavirus-control-plan-alert-levels-in-wales-coming-out-of-lockdown.pdf; INQ000081858)
- Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown, Welsh Government, February 2021, p11 (https://www.gov.wales/sites/default/files/publications/2021-02/coronavirus-control-plan-alert-levels-in-wales-coming-out-of-lockdown.pdf; INQ000081858)
- Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown, Welsh Government, February 2021, p12 (https://www.gov.wales/sites/default/files/publications/2021-02/coronavirus-control-plan-alert-levels-in-wales-coming-out-of-lockdown.pdf; INQ000081858)
- COVID-19 Response – Spring 2021, HM Government, February 2021 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087); INQ000088893
- INQ000061587; INQ000061588; INQ000061589; INQ000061593
- COVID-19 Response – Spring 2021, HM Government, February 2021, p25, para 83 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- COVID-19 Response – Spring 2021 (Summary), Cabinet Office, 22 February 2021 (https://www.gov.uk/government/publications/covid-19-response-spring-2021/covid-19-response-spring-2021-summary; INQ000054709)
- COVID-19: Scotland’s Strategic Framework Update, Scottish Government, February 2021 (https://www.gov.scot/publications/coronavirus-covid-19-strategic-framework-update-february-2021; INQ000339831); INQ000214549; INQ000232693; INQ000233242
- INQ000369727; COVID-19: Scotland’s Strategic Framework Update, Scottish Government, February 2021 (https://www.gov.scot/publications/coronavirus-covid-19-strategic-framework-update-february-2021; INQ000339831)
- INQ000232952_0001 paras 5-6
- INQ000232952_0001 paras 5-6
- INQ000232952_0001 paras 5-6
- Moving Forward: The Executive’s Pathway out of Restrictions, Northern Ireland Executive, 2 March 2021, pp1-4 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/executives-pathway-out-of-restrictions.pdf; INQ000104467)
- Moving Forward: The Executive’s Pathway out of Restrictions, Northern Ireland Executive, 2 March 2021, p14 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/executives-pathway-out-of-restrictions.pdf; INQ000104467)
- INQ000065711_0007
- INQ000436642_0032-0033 paras 146-147. The issue of ministers making public statements that contradict or undermine Executive Committee decision-making is discussed in Chapter 11: Government decision-making, in Volume II.
- COVID-19 Response – Spring 2021, HM Government, February 2021, p7 para 3 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- COVID-19: Scotland’s Strategic Framework Update, Scottish Government, February 2021, p3 (https://www.gov.scot/publications/coronavirus-covid-19-strategic-framework-update-february-2021; INQ000339831)
- Coronavirus Control Plan: Alert Levels in Wales – Coming out of Lockdown, Welsh Government, February 2021, p3 (https://www.gov.wales/sites/default/files/publications/2021-02/coronavirus-control-plan-alert-levels-in-wales-coming-out-of-lockdown.pdf; INQ000081858)
- Moving Forward: The Executive’s Pathway out of Restrictions, Northern Ireland Executive, 2 March 2021, p8 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/executives-pathway-out-of-restrictions.pdf; INQ000104467)
- INQ000065606_0004
- INQ000065606_0006 para 12
- INQ000065606_0007 para 13
- INQ000065606_0005 para 10
- INQ000066445_0002
- INQ000066445_0002
- INQ000022529; INQ000066445_0002
- ‘Stay local: Wales takes first steps out of lockdown’, Welsh Government, 12 March 2021 (https://www.gov.wales/stay-local-wales-takes-first-steps-out-of-lockdown; INQ000054847_0002)
- INQ000022529
- Coronavirus Control Plan: Revised Alert Levels in Wales (March 2021), Welsh Government, March 2021, p17 (https://www.gov.wales/sites/default/files/publications/2021-03/coronavirus-control-plan-revised-alert-levels-in-wales-march-2021.pdf; INQ000066069)
- INQ000214489
- INQ000214489_0007 para 20(a)
- INQ000065606_0020 paras 56, 57
- INQ000048521_0003-0004 para 10
- INQ000048521_0003-0004 para 10
- INQ000023284_0001
- INQ000022532
- ‘New campaign urges public to get tested twice a week’, Department of Health and Social Care, 9 April 2021 (https://www.gov.uk/government/news/new-campaign-urges-public-to-get-tested-twice-a-week; INQ000234854_0001)
- ‘Free lateral flow Covid tests in Wales for those unable to work at home’, BBC News, 14 April 2021 (https://www.bbc.co.uk/news/uk-wales-56746340; INQ000584981)
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 20 April 2021’, Scottish Government, 20 April 2021(https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-20-april-2021; INQ000354330)
- ‘Further extension to Workforce Covid-19 testing programme’, Department of Health, 28 April 2021 (https://www.health-ni.gov.uk/news/further-extension-workforce-covid-19-testing-programme; INQ000348844)
- INQ000255836_0178 para 616(b); COVID-19 Response – Spring 2021, HM Government, February 2021 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- ‘Covid in Scotland: Families and friends reunite as restrictions ease’, BBC News, 16 April 2021 (https://www.bbc.co.uk/news/uk-scotland-56765188; INQ000357550)
- INQ000129892_0002 para 2.3
- INQ000129892_0003 paras 2.6, 2.8, 2.10
- ‘Covid: Scotland’s R number falls for first time in four weeks’, BBC News, 23 April 2021 (https://www.bbc.co.uk/news/uk-scotland-56863783; INQ000357762)
- ‘Covid in Scotland: Shops, gyms, pools and pubs reopen after lockdown’, BBC News, 26 April 2021 (https://www.bbc.co.uk/news/uk-scotland-56878753; INQ000357672)
- INQ000048525_0004-0005 para 18
- ‘Don’t drop “data, not dates” approach, UK adviser warns as Covid cases surge’, The Guardian, 29 May 2021 (https://www.theguardian.com/world/2021/may/29/dont-drop-data-not-dates-approach-uk-adviser-warns-as-covid-cases-surge; INQ000370285)
- INQ000370347_0053-0054 para 108
- COVID-19 Response – Spring 2021, HM Government, February 2021, p8, para 8 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- COVID-19 Response – Spring 2021, HM Government, February 2021, p8, paras 8, 10 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- COVID-19 Response – Spring 2021, HM Government, February 2021, p25, para 82 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- Vaughan Gething 11 March 2024 194/17-22
- Vaughan Gething 11 March 2024 195/9-14
- INQ000048522_0002-0003 para 6
- INQ000065698_0005
- INQ000436641_0051 para 199
- INQ000436641_0051-0052 para 200
Chapter 8: Learning to live with Covid-19 (May 2021 to May 2022)
Introduction
| 8.1. | In late April and early May 2021, infection rates were low and the four nations of the UK began to emerge from the restrictions imposed in December 2020 and January 2021, in line with the published strategies in each nation. |
| 8.2. | The subsequent period from May 2021 to May 2022 was characterised by an attempt by the four governments to balance recovery from the effects of the first wave with the emergence of variants of Covid-19 and the continued need to manage the direct and indirect harms of the virus. The emergence of the Delta variant, first detected in March 2021, led to delays in the planned relaxation of restrictions. In the autumn of 2021, the emergence of the more transmissible Omicron variant caused an increase in infections and led to the reintroduction of restrictions. This period was characterised by a race between the rollout of the vaccines and the emerging variants. |
| 8.3. | By May 2022, about 1.75% of the UK population was still testing positive for Covid-19 at the time that all legal restrictions came to an end, but vaccines had succeeded in substantially reducing the rates of death and serious illness caused by the virus.1 This chapter examines the events of the period between May 2021 and May 2022, the decisions taken in each nation in light of the evidence that was available to decision-makers at the time and whether such decisions were reasonable. |
May to July 2021
| 8.4. | At the start of May 2021, all four nations were still subject to strict restrictions. England was at Step 2 of the COVID-19 Response – Spring 2021 roadmap (discussed in Chapter 7: Further lockdowns, in this volume).2 On 26 April 2021, all of Scotland had moved to Level 3 restrictions.3 On 3 May, Wales had moved to Alert Level 3 (high-risk) of its system of restrictions.4 By the start of May, the Northern Ireland Executive had taken initial steps across a number of the pathways in The Executive’s Pathway out of Restrictions and indicative dates for further relaxations in May had been identified.5 |
The emergence of the Delta variant: May 2021
| 8.5. | A new threat began to emerge in April 2021, with a surge of cases in India.6 This variant – Delta – ultimately proved to be more transmissible than the Alpha variant.7 First identified in the UK in March 2021, cases rapidly grew throughout April and May 20218 and it went on to become the dominant strain throughout the UK.9 This new wave peaked in the UK on 15 July 2021 with 62,000 cases.10 At the peak, it is likely that over 1 million people were infected across the UK.11 |
| 8.6. | On 5 May 2021, the Scientific Advisory Group for Emergencies (SAGE) noted that there had been “a significant recent increase in prevalence of [the Delta variant], including some community transmission“.12 Early indications were that it “may be more transmissible“.13 Modelling indicated that while Step 3 of the COVID-19 Response – Spring 2021 roadmap alone was “highly unlikely to put unsustainable pressure on the NHS“, it was “likely to lead to R [the reproduction number] being greater than 1 in England“.14 It remained “highly likely” that there would be a further resurgence in hospitalisations and deaths, though “the scale, shape, and timing remain highly uncertain“.15 The resurgence would be smaller if baseline measures and sustained behavioural changes “which reduce transmission are maintained beyond the end of the roadmap“.16 Baseline measures included self-isolation, use of certification or ‘test to enter’, partial home working, good ventilation and face coverings.17 The speed of vaccine rollout was also a key factor. SAGE advised that, without interventions, a variant that substantially escaped immunity through the vaccines or was highly transmissible could lead to a very significant wave of infections, potentially larger than that seen in January 2021. |
| 8.7. | Subsequently, on 10 May 2021, the UK Cabinet approved the decision to move to Step 3 on 17 May.18 Boris Johnson MP, Prime Minister from July 2019 to September 2022, noted that although new variants “remained a cause for concern“, they did not prevent Step 3 from proceeding.19 That same day, following advice from the Joint Biosecurity Centre, the Chief Medical Officers for the four nations and the NHS England National Medical Director announced that the UK-wide alert level should be reduced from Level 4 to Level 3.20 |
Figure 28: Step 3, COVID-19 Response – Spring 2021 roadmap
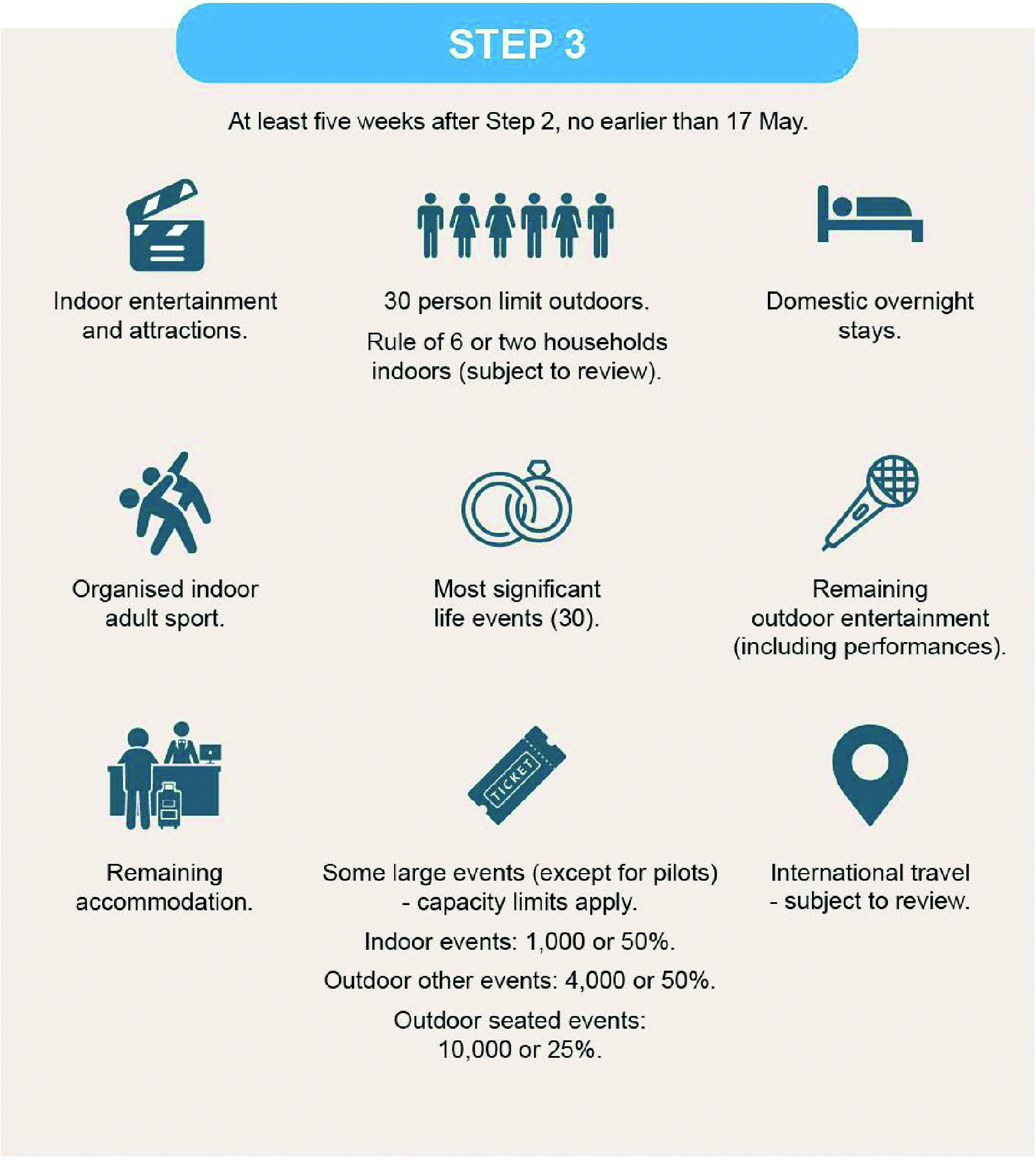
Source: COVID-19 Response – Spring 2021, HM Government, February 2021 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087_0040)
| 8.8. | On 12 May 2021, the Scientific Pandemic Infections Group on Modelling, Operational sub-group (SPI-M-O) estimated the Delta variant to be up to 50% more transmissible than the Alpha variant. It was uncertain whether this would apply to wider community transmission because the number of Delta variant cases was “small and relatively focussed“.21 If it did, there were:
“still too few adults vaccinated to prevent a significant resurgence that ultimately could put unsustainable pressure on the NHS, without non-pharmaceutical interventions“.22 This was endorsed by SAGE on 13 May, which advised that it was “likely that progressing with step 3 alone“, without further measures, “would lead to a substantial resurgence of hospitalisations … [p]rogressing with both steps 3 and 4 at the earliest dates could lead to a much larger peak“.23 SAGE reiterated the lessons learned earlier in the pandemic, emphasising that the: “‘earlier, harder, broader’ principles of responding quickly, taking strong measures, and doing so over a wider geography than where the issues have been identified in response to outbreaks, remain relevant. Testing, tracing and, in particular, isolating cases remained very important.“24 |
| 8.9. | On 12 May 2021, Dr Rob Orford, Chief Scientific Adviser (Health) for Wales from January 2017, updated the Welsh Cabinet about “concerns amongst the scientific community on the rapid spread of this [Delta] variant and the potential for any vaccine escape“.25 The Welsh Cabinet determined that it was too soon to make any further decisions on social distancing. However, it confirmed the move to Alert Level 2 from 17 May, which included the reopening of indoor hospitality subject to the ‘rule of six’.26 |
| 8.10. | On 13 May 2021, the reproduction number (R) was estimated to be between 0.8 and 1.1 in England and Northern Ireland, 0.8 and 1.0 in Scotland, and 0.7 and 1.0 in Wales. R is an indicator that lags by two to three weeks.27 The Joint Committee on Vaccination and Immunisation considered data that showed “evidence of vaccine effectiveness particularly after two doses against the variant“.28 It concluded that “bringing the second dose interval forwards from 12 to 8 weeks would be reasonable” and “the overarching priority was to vaccinate those in vulnerable groups who had not yet received their first dose of vaccine“.29 The following day, the UK government announced that the most vulnerable would be offered a second dose earlier.30 |
| 8.11. | On 13 May 2021 in Northern Ireland, Arlene Foster MLA (later Baroness Foster of Aghadrumsee), First Minister of Northern Ireland from January 2016 to January 2017 and from January 2020 to June 2021 and Michelle O’Neill MLA (deputy First Minister of Northern Ireland from January 2020 to February 2022) proposed a series of further relaxations. These were to come into effect on 21 June subject to ratification by the Executive Committee on 17 June.31 Professor (later Sir) Michael McBride (Chief Medical Officer for Northern Ireland from September 2006) and Professor Ian Young (Chief Scientific Adviser to the Department of Health (Northern Ireland) from November 2015) reiterated their preference for “an incremental approach to easing of restrictions“.32 Following discussion and amendment to a number of recommendations contained in the Executive Paper, the Executive Committee agreed to a number of relaxations and mitigations, including increasing the number of people allowed for indoor gatherings to those permitted by a risk assessment or the venue. The Minister of Health and the Minister for Infrastructure did not support the Northern Ireland Executive’s decision to increase the numbers permitted for indoor gatherings in this way.33 |
| 8.12. | On 14 May 2021, the Scottish Government’s Four Harms Group, an advisory group responsible for facilitating discussion of the four harms approach, noted that Delta could become the dominant variant in Scotland within a fortnight and agreed that it should be monitored.34 On 17 May, the Scottish Government proceeded with the easing of restrictions, which it had announced on 11 May. Most of mainland Scotland moved from Level 3 to Level 2, which permitted indoor service in pubs and restaurants. The Scottish island regions moved to Level 1, which permitted higher numbers of people to meet for significant life events and outdoor events.35 England also moved to Step 3. |
| 8.13. | On 18 May 2021, the UK Cabinet recognised that cases were “very low“, although “everyone was acutely aware of the risks posed by [the Delta variant] and its prevalence in particular areas“.36 Professor Sir Patrick Vallance (later Lord Vallance of Balham), Government Chief Scientific Adviser from April 2018 to March 2023, advised that the Delta variant was “more transmissible” and was replacing the Alpha variant. Professor (later Sir) Jonathan Van-Tam, Deputy Chief Medical Officer for England from October 2017 to March 2022, expressed confidence “that two doses of the vaccine could interrupt transmission, rather than one“.37 Mr Johnson insisted on a cautious approach being maintained.38 |
| 8.14. | By 20 May 2021, there was no evidence of sustained community transmission of the Delta variant in Northern Ireland.39 However, there was a higher incidence of Covid-19 cases generally than in the rest of the UK.40 The Northern Ireland Executive ratified a series of proposed relaxations.41 Robin Swann MLA (Minister of Health for Northern Ireland from January 2020 to October 2022 and from February to May 2024) advised that “[o]verall, there is no immediate reason based on current data not to confirm the proposed relaxations“.42 However, the Executive Paper from the Department of Health observed that:
“The relaxations proposed by the Executive go somewhat beyond those assumed in modelling or being implemented elsewhere in the UK or ROI [Republic of Ireland] at present, despite our higher incidence compared with the rest of the UK … In addition, modelling does not account for the potential impact of [the Delta variant] (up to 60% increase in transmission), the possibility of reduced vaccine uptake or effectiveness, waning immunity or cross border movements, or poor adherence to remaining mitigations.“43 In a pessimistic scenario, it was estimated that: “cases would peak at 5000 – 15000 per day, and hospital pressures would be similar to or a little less than those observed in January/February this year“.44 |
| 8.15. | On 21 May 2021, the Scottish Cabinet noted preliminary indications that the Delta variant would be unlikely to cause a significant increase in serious illness or mortality, even among older age groups.45 |
| 8.16. | In a meeting of the Four Harms Group on 25 May 2021, there was some concern about the Scottish Government’s working assumption that Scotland would move to Level 0 (the lowest level of restrictions, permitting gatherings of up to eight people from up to four households in private dwellings) on 28 June, and beyond Level 0 at the regular review three weeks later on 16 July.46 Nicola Sturgeon MSP, First Minister of Scotland from November 2014 to March 2023, wanted “to move away from Government direction to a point where people make decisions themselves“, but stated: “[W]e are not out of the woods yet.“47 There was a tension between Ms Sturgeon’s desire to move down in levels and the ongoing concerns about the threat of Covid-19, in particular the emerging information about the Delta variant and the ability of the vaccination programme to keep it under control. It was around this time that Humza Yousaf MSP, Cabinet Secretary for Justice from June 2018 to May 2021 and Cabinet Secretary for Health and Social Care from May 2021 to March 2023, expressed his view privately that Ms Sturgeon was worried about “losing the dressing room“.48 This suggested that there was some concern that the imposition of greater restrictions at this time would not be popular with the public. |
| 8.17. | On 27 May 2021, R was estimated to be between 1.0 and 1.1 in England, between 1.0 and 1.3 in Scotland, between 0.8 and 1.1 in Wales, and between 0.7 and 1.1 in Northern Ireland.49 SAGE remained uncertain about how much more transmissible the Delta variant was, but, if in the region of 40%, it was likely that there would be a substantial increase in hospitalisations. It was expected that the uncertainty would reduce within a fortnight as data became available. Public Health England analysis also indicated some decrease in vaccine effectiveness. Data were not available with regard to the Delta variant’s severity, but there had been no indication that it was more severe.50 The number of people estimated to have Covid-19 in England was approximately half of the estimate in April 2021.51 SPI-M-O’s consensus view was that deaths across the UK would remain very low over the forthcoming four weeks, with the caveat that their projections and views did not fully reflect policy or behavioural change in the two to three weeks prior, owing to delays in infection, need for hospital care and deaths.52 |
| 8.18. | That same day, the Welsh Cabinet agreed that it should proceed to move to Alert Level 1 (at the time, the lowest level of Wales-wide restrictions, as outlined in Coronavirus Control Plan: Revised Alert Levels in Wales) on 7 June 2021, provided that conditions remained stable over the following week.53 |
| 8.19. | In Northern Ireland, while a number of cases had been detected, there remained no evidence of sustained transmission of the Delta variant.54 The relaxations at the end of April had not significantly impacted transmission.55 On 27 May 2021, the Executive Committee agreed to ratify some proposed relaxations and to lift the guidance (but retain mitigations) relating to Common Travel Area travel, aligning Northern Ireland with the rest of the UK.56 However, Mr Swann remained of the view that the guidance should be retained:
“until the impact of the easement of restrictions from … 24 May could be assessed, and in order to delay the importation of variants of concern … allowing time for wider vaccination roll-out and minimising any potential for community transmission“.57 Professors McBride and Young cautioned that removing the guidance on self-isolation on travel within the Common Travel Area “would accelerate the introduction” of the Delta variant into Northern Ireland.58 |
| 8.20. | A Scottish Cabinet meeting on 1 June 2021 concluded:
“[A] ‘one size fits all’ approach to the next review of protection levels due by 7 June was unlikely to be effective or credible at a time when there was very low incidence [in many areas].”59 |
| 8.21. | On 5 June 2021, much of mainland Scotland was moved to Level 1 restrictions (apart from the Central Belt, including Glasgow, which was put at Level 2) and island communities were moved to Level 0.60 |
| 8.22. | By 3 June 2021, R was estimated to have increased in England, Wales and Scotland since 13 May, but estimates for Northern Ireland remained similar.61 SAGE confirmed that this did not fully reflect changes following the relaxation of measures on 17 May in England, or the recent rapid increases in transmission of the Delta variant. There remained uncertainty about transmissibility and potentially an increased risk of hospitalisation. There was no evidence of worse outcomes for those hospitalised with the Delta variant. Vaccination continued to reduce the risks of hospitalisation in older people. SAGE advised that “delaying further increases in contacts (e.g., step 4 of the roadmap in England)” for even a few weeks “would allow more people to be protected by vaccination before transmission increases further“.62 This in turn would reduce hospital admissions and delay and reduce the peak number of admissions. |
Long Covid
| 8.23. | It is well recognised that viral infections can cause longer-term illnesses, known as long-term sequelae. Professor Sir Christopher Whitty, Chief Medical Officer for England from October 2019, told the Inquiry:
“[I]nitial planning for COVID-19 took no account of the group of chronic (prolonged) syndromes which have subsequently become known as Long COVID. It was not that the possibility of some chronic sequelae was not accepted, but rather that the nature and scale of it was not foreseen.“63 |
| 8.24. | At the outset of the pandemic, messaging also focused almost exclusively – and understandably – on the potential severity of becoming infected with Covid-19 and the risk of death. Even when it was clear that there was a risk from Long Covid, there were no public health campaigns focused on communicating the risks or the evolving understanding of the syndrome.64 Dr Rachael Evans, expert witness with Professor Chris Brightling on Long Covid, underscored the need for distinct public messaging to distinguish Long Covid from the narrower risk profile of severe, acute Covid-19 infection:
“[A]ctually anyone can develop Long Covid. So anyone that’s contracting the infection can end up unfortunately with this very prolonged illness.“65 |
| 8.25. | In the absence of such information, individuals would have been unable to make their own, fully informed decisions about the levels of risk they were prepared to tolerate and the risks posed to others around them. Public messaging about the incidence and existence of Long Covid would likely have had a considerable, positive impact on those experiencing it and, perhaps, on those dismissive of symptoms. The UK government should have acknowledged Long Covid and made the risks clear in public health messaging. The potential for long-term sequelae arising from infection and any developing understanding should be communicated to the public in any future pandemic. |
| 8.26. | In May 2020, SAGE had noted the “existence of longer-term health sequelae” and “the importance of monitoring these impacts through longer-term cohort studies“.66 Patient-led groups had begun to be formed in May and June 2020 to provide support to those affected and to promote public awareness of ongoing symptoms.67 A literature review and research into the long-term effects of Covid-19 were commissioned and funded.68 |
| 8.27. | In July 2020, the NHS launched the ‘Your Covid Recovery’ website and Matt Hancock MP (Secretary of State for Health and Social Care from July 2018 to June 2021) chaired a roundtable to consider the long-term impacts of Covid-19 infection.69 Guidance about the long-term health effects of Covid-19 was subsequently published in early September 2020.70 In October 2020, NHS England launched a five-point plan, including guidance from the National Institute for Health and Care Excellence (known as NICE), research funding and a Long Covid Taskforce, while Wales also funded a recovery programme and Scotland provided investment to the health boards to support local services for Long Covid.71 |
| 8.28. | There was sufficient information available by October 2020 for decision-makers to understand that Long Covid was a significant policy and health issue to be tackled.72 However, the UK government – in particular Mr Johnson – remained slow to acknowledge the seriousness and prevalence of the condition and to direct that greater attention be paid to how it could be addressed, mitigated and taken into account in decision-making on strategy and the imposition of interventions. In October 2020, Mr Johnson wrote “BOLLOCKS” on a box note relating to Long Covid.73 He acknowledged that it took him “some time to recognise that long Covid was a serious condition“, adding: “For some time, therefore, I was not convinced that long Covid truly existed.“74 Imran Shafi (Private Secretary to the Prime Minister for public services from March 2018 to March 2021) advised Mr Johnson in January 2021 that he was obtaining “objective clinical advice” on the extent to which Long Covid was a “reasonable policy consideration“.75 |
| 8.29. | In response to a request from Mr Johnson, on 31 May 2021 Professor Whitty produced a note on Long Covid.76 His written advice outlined that there was “a large enough problem to be concerned about“.77 Professor Whitty’s solution was to “stop people getting COVID; no COVID, no Long COVID“.78 |
| 8.30. | Professor Brightling and Dr Evans told the Inquiry:
“[I]t was foreseeable that there was going to be long-term sequelae from Covid-19 extrapolated from previous coronavirus pandemics and previous knowledge of post-viral syndromes.“79 |
| 8.31. | Professor Whitty acknowledged that the failure to recognise that “Long COVID would be a significant part of the disease burden of COVID-19 early in the pandemic however had important practical implications” for the management of the pandemic and consideration of the effects of Covid-19.80 In future pandemics, consideration of long-term sequelae must be built into any strategy and supporting plans.81 |
June 2021
| 8.32. | On 3 June 2021, the Welsh Cabinet followed public health advice to stagger the move to Alert Level 1 to delay the “most risky relaxations” and obtain data on the new variant.82 In the first stage, up to three different households could meet indoors and different events would be subject to maximum capacity levels.83 |
| 8.33. | By 9 June 2021, R was estimated to have increased across the UK.84 It was difficult to separate the effects of the Delta variant’s growth from recent changes in restrictions.85 Modelled scenarios showed a larger wave than that modelled prior to Step 3 in England, owing to the emergence of the Delta variant. However, uncertainty remained about the impact on hospital admissions.86 SAGE advised that a number of potential hospitalisations and deaths could be avoided rather than simply delayed if Step 4 of the COVID-19 Response – Spring 2021 roadmap was taken after 21 June. Modelling suggested that delaying Step 4 by four weeks beyond 21 June could reduce hospital admissions by around one-third to one-half (by allowing further time for vaccine coverage) and would move relaxations closer to the school holidays when transmission was expected to reduce. It would also allow time to better understand the risk and impact of the Delta variant. The peak was expected to occur around August 2021. There was considerable uncertainty about the impact on the NHS of taking Step 4.87 |
| 8.34. | Discussions had been taking place within the UK government throughout this period on the impact of the Delta variant on Step 4. An update to the public was due on 14 June 2021, in advance of implementation on 21 June.88 However, the rising rates of infections and scientific advice caused concern. On 8 June, Mr Johnson reiterated to the UK Cabinet the need for a cautious approach.89 |
| 8.35. | By 14 June 2021, there were around 8,000 cases a day in England – the highest since the end of February.90 Hospitalisations were doubling. Professor Whitty noted that “[w]ithin five to six doublings, the numbers would be at very dangerous levels“.91 The next phase of opening up would further increase doubling speed. Professor Vallance reiterated that a second dose of the vaccine was required to give more protection against the Delta variant and reduce hospitalisation. A four-week delay would allow further uptake.92 |
| 8.36. | Following meetings on 13 and 14 June 2021, the Covid-19 Operations Committee (Covid-O) decided to delay Step 4 in England, with some limited exceptions, by four weeks to 19 July.93 The emergence of the Delta variant meant that the fourth test in the COVID-19 Response – Spring 2021 roadmap – “our assessment of the risks is not fundamentally changed by new Variants of Concern” – was not met.94 In advance of the next review on 12 July, the time between the first and second dose of the vaccine was to be reduced from 12 weeks to 8 weeks.95 As noted by Professor Vallance, the interval between steps was an important opportunity to obtain and analyse data and information.96 The advice was clear that there would be:
“an increase in the number of people hospitalised and dying, but this would be proportionately fewer than in previous waves. There would be a race between the number of people that the vaccination programme would protect against the growth of the virus.“97 |
| 8.37. | Similar advice about pausing restrictions to await vaccine uptake, in the wake of rising cases, was provided to the Scottish Government, Welsh Cabinet and Northern Ireland Executive.98 All three governments followed this advice. The Welsh Cabinet agreed to pause the move to Alert Level 1 until at least the next review, due by 15 July 2021.99 |
| 8.38. | On 10 June 2021, Professors McBride and Young advised the Northern Ireland Executive that, in light of health service pressures, there was “little tolerance or capacity for significant increased Covid-19 admissions“, and that if:
“admissions of the Delta variant are x2.4 and vaccine effectiveness more dependent on second doses then the Executive will need to factor this into the timing of decisions on any further relaxations which may be best deferred to middle to end of July“.100 In Northern Ireland, a new ratification date was fixed for 1 July 2021 for relaxations to take effect on 5 July.101 |
| 8.39. | On 18 June 2021, Ms Sturgeon announced a ban on non-essential travel between Scotland and parts of Greater Manchester and Salford from 21 June because of rising Covid-19 cases in the area.102 The Scottish Cabinet had not discussed the ban and there was no consultation with the UK government or with Andy Burnham (Mayor of Greater Manchester from May 2017). Mr Burnham told the Inquiry it was “[e]xactly what the Scottish National Party would always have accused Westminster of doing to Scotland“.103 |
| 8.40. | Several days later, on 22 June 2021, the Scottish Government announced the lifting of all Covid-19 restrictions (ie, beyond Level 0) in Scotland for 9 August, but it delayed the move to Level 0 for the Scottish mainland from 28 June to 19 July.104 The highest number of daily cases in Scotland since the start of mass testing was reported the next day.105 |
| 8.41. | On 26 June 2021, Mr Hancock resigned as Secretary of State for Health and Social Care, apologising for breaching social distancing guidance.106 Sajid Javid MP was appointed in his place and served in the role from June 2021 to July 2022. |
| 8.42. | Vaccines were, as predicted, disrupting the connection between infection and serious illness, hospitalisation and death. The median age of those hospitalised with Covid-19 had reduced from people in their mid-60s to those in their mid-40s, due to vaccination coverage in older people.107 |
Increasing cases
Figure 29: Estimated percentage of the population testing positive for Covid-19 from 1 May to 31 July 2021 across the UK
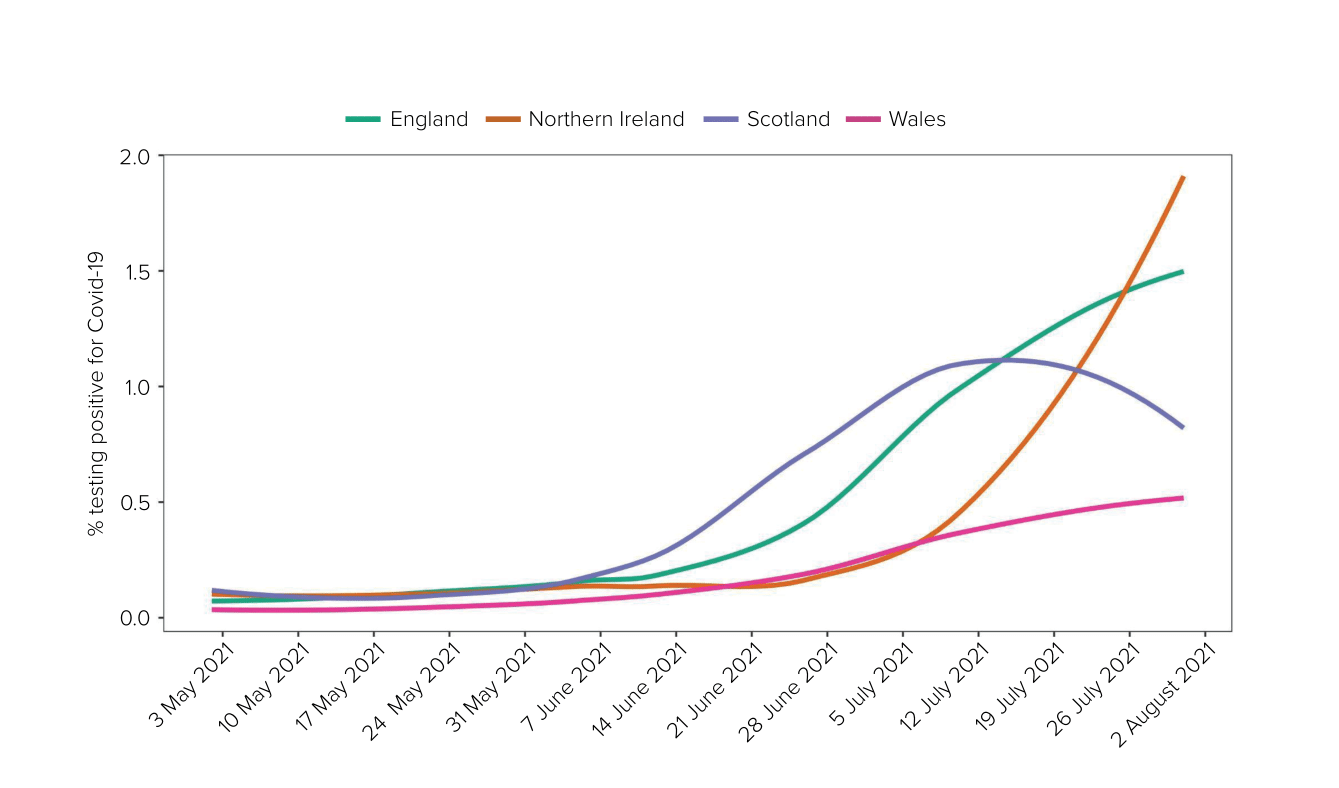
Source: Coronavirus Infection Survey from 1 May to 31 July 2021. (Modelled estimates, 95% confidence intervals not shown). For raw data, see the Coronavirus (COVID-19) Infection Survey: England, dataset, Office for National Statistics, 10 March 2023 (https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/coronaviruscovid19infectionsurveydata/2023)
| 8.43. | At the beginning of July 2021, although the rate of infection was growing across all parts of the UK, there were differences in prevalence between the four nations.108 By 1 July, there was an early indication of increased hospital admissions in Northern Ireland.109 It was estimated that there might be 2,000 to 3,000 cases per day by the end of July, with significantly greater numbers in August.110 The Department of Health advised delaying any further relaxations to reduce the risk of even greater increases.111 Nonetheless, ministers agreed that, from 5 July, relaxations, including for mass and outdoor gatherings at domestic settings, would take effect.112 The Northern Ireland Executive published Building Forward: Consolidated Covid-19 Recovery Plan.113 |
| 8.44. | By 5 July 2021, some Scottish health boards were experiencing “considerable pressure” – if cases continued to grow, there would be a need to consider “standing down elective services“.114 There had been a 61% increase in Covid-19 hospital bed occupancy in one week.115 However, overall hospital occupancy remained considerably below the January 2021 peak.116 |
| 8.45. | On 5 July 2021, the UK government published Covid-19 Response: Summer 2021.117 This was not a roadmap akin to the COVID-19 Response – Spring 2021 roadmap. It was a much shorter document, which set out at a high level the government’s new approach and intentions for the summer. It did not, for example, contain triggers or tests to be met for the imposition of restrictions or specific responses. It explained that Step 4 would mark a new phase in the response, “moving away from stringent restrictions” towards an advisory approach with targeted interventions to:
Contingency measures would be retained to respond to unexpected events, while accepting that further cases, hospitalisations and deaths would occur as the country learned to live with Covid-19. The most significant risk was a ‘variant of concern’, which fully or partially escaped immunity otherwise conferred by past infection or the vaccines. Contingency plans would be maintained but such “measures would only be re-introduced as a last resort to prevent unsustainable pressure on the NHS“.118 |
| 8.46. | That same day, the Welsh Cabinet discussed Technical Advisory Group advice that indicated “a significant weakening of the link between infections and serious illness“, which might lead to a shift in the balance of harms. The Cabinet therefore agreed that a baseline alert level should be created to represent a final set of restrictions.119 |
| 8.47. | On 7 July 2021, SAGE advised that modelling scenarios showed an “extremely high prevalence of infection lasting until at least the end of August“.120 This presented four “major risks“.121 SAGE warned that the “combination of high prevalence and high levels of vaccination creates the conditions in which an immune escape variant is most likely to emerge“.122 Furthermore:
“If the aim is to avoid the NHS becoming overwhelmed … it is important to understand the impact of different levels of admissions on NHS function and have appropriate contingency plans in place … at any point that cases are still increasing exponentially, admissions can be expected to at least double once more regardless of any measures put in place at that point.“123 On Step 4, it advised: “Although a further delay to step 4 could have some additional positive impact by allowing more people to be vaccinated, the effect of this would be much smaller than the effect of the current delay and it would push the wave further towards the autumn and winter.“124 SAGE emphasised that the peak of the resurgence would be much lower if the return to pre-pandemic behaviours was “gradual” – a very rapid return could lead to a peak in hospitalisations similar to (or possibly even higher than) previous peaks.125 Baseline measures would assist in reducing transmission and hospitalisation. |
| 8.48. | On 8 July 2021, Professor Young advised the Northern Ireland Executive Committee that rates of transmission were increasing in those over the age of 60. Hospital admission rates were increasing; however, intensive care unit occupancy remained low compared with earlier in the pandemic.126 The Executive Committee agreed to extend the restrictions and scheduled a further review four weeks later. It voted against proposals for certain venues to be permitted to open from 8 July and against increasing the number of households permitted to meet in a domestic setting from 8 July. An indicative date of 26 July for these relaxations was retained.127 |
| 8.49. | At a Covid-O meeting on 12 July 2021, James Bowler (Second Permanent Secretary to the Cabinet Office and Head of the Covid-19 Taskforce from October 2020 to August 2021) advised that the benefits of a further delay were “unclear, and could compound risks by pushing the third wave into the winter“, although it was acknowledged that the country would be opening up against a backdrop of increasing and high infection and prevalence rates.128 Once again during this period, the Secretary of State for Health (which was now Mr Javid) and Michael Gove MP (later Lord Gove), Chancellor of the Duchy of Lancaster from July 2019 to September 2021 and Minister for the Cabinet Office from February 2020 to September 2021, were urging a more cautious approach, with Mr Johnson and Rishi Sunak MP (Chancellor of the Exchequer from February 2020 to July 2022) in favour of loosening restrictions and opening up more quickly.129 Covid-O agreed that, as recommended by the Covid-19 Taskforce, the four tests the UK government had outlined for easing Covid-19 restrictions had been met. However, the confidence that test three – which related to the risk of pressures on the NHS – had been met was not as high.130 The priority was to avoid a return to pre-pandemic behaviour. Messaging would be crucial and should be focused on a gradual and cautious return and reopening.131 Mr Johnson announced on the evening of 12 July that Step 4 of the COVID-19 Response – Spring 2021 roadmap would go ahead as planned in England on 19 July.132 |
Figure 30: Step 4, COVID-19 Response – Spring 2021 roadmap
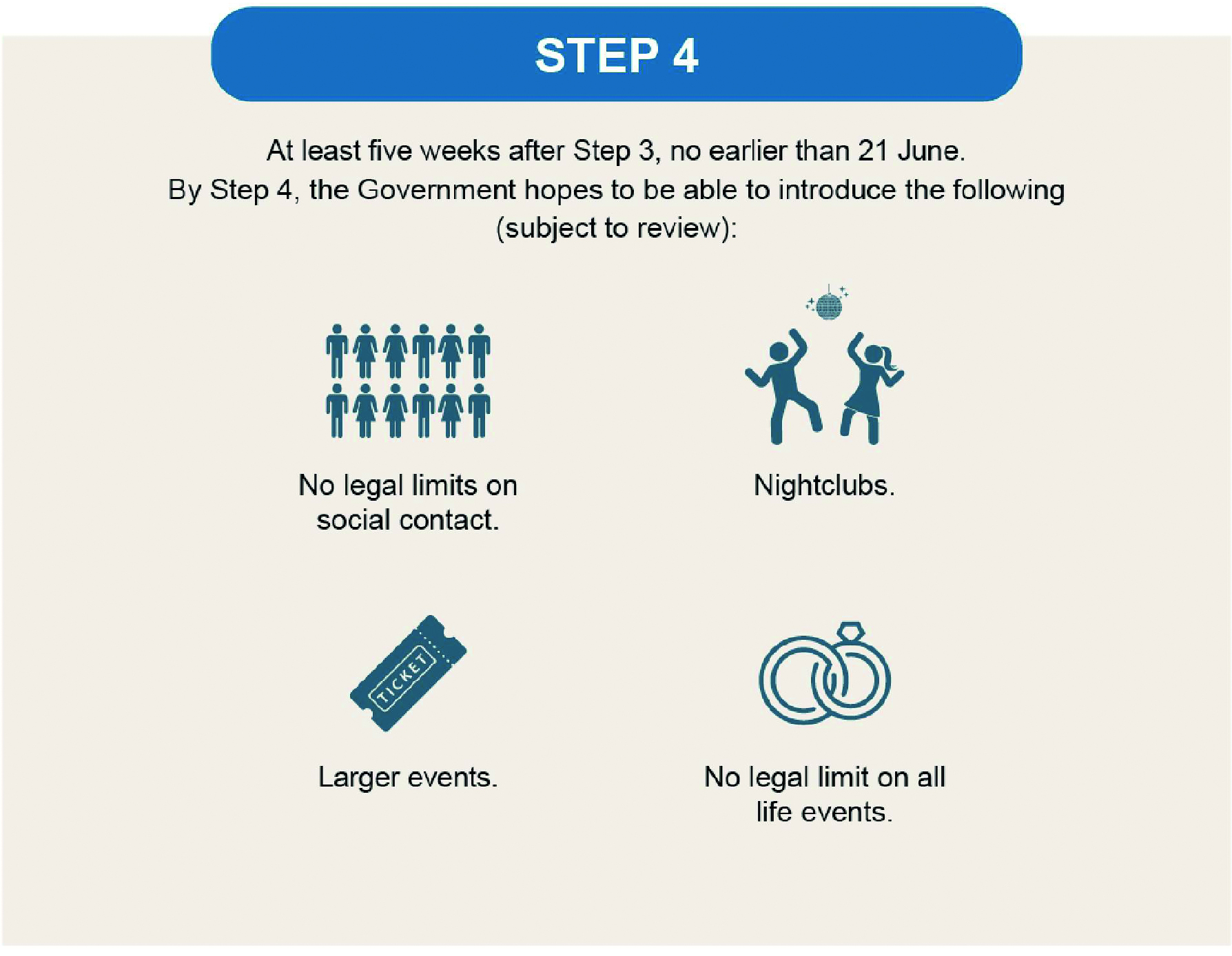
Source: COVID-19 Response – Spring 2021, HM Government, February 2021 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087_0043)
| 8.50. | In Wales, while community transmission was high, the “pressure on the NHS in Wales was stable and it was experiencing the lowest levels of COVID-19 since reporting had begun“.133 Vaccination coverage in people aged over 40 was also high and “this … appeared to have altered the relationship between community transmission and harms“.134 Dr (later Sir) Frank Atherton, Chief Medical Officer for Wales from August 2016, advised that this:
“indicated that the current epidemiological picture changed the balance between direct and indirect harms and made it increasingly difficult to justify the stringent use of public health powers to continue restricting economic, social and cultural activities“.135 Reflecting these assessments, the updated Coronavirus Control Plan acknowledged that “other harms from the pandemic … are beginning to outweigh the direct harms from the virus“.136 The Welsh Cabinet agreed to make a number of relaxations from 17 July 2021, including a move to Alert Level 0 on 7 August.137 |
Figure 31: Alert levels in Wales in the summer of 2021

Source: ‘Most Covid rules set to be lifted in Wales on 7 August’, BBC News, 14 July 2021 (https://www.bbc.co.uk/news/uk-wales-57823021; INQ000548025)
| 8.51. | On 13 July 2021, the Scottish Cabinet considered that pressures on NHS and care staff would remain at excessive levels unless cases could be reduced.138 It noted that Covid-19 was becoming a disease that was more likely to be caught by younger people and that increasing knowledge of “‘long COVID’ … should also give pause for thought“.139 This was the first discussion of Long Covid in the Scottish Cabinet. Despite the recognition that the number of cases had to be reduced to protect the NHS, the Cabinet agreed that, from 19 July, Level 0 should be applied across Scotland, but with a number of modifications.140 |
| 8.52. | England moved to Step 4 that same day, at the same time changing advice for the clinically extremely vulnerable (see Chapter 10: Vulnerabilities and inequalities, in Volume II), who were to follow the same guidance as the rest of the population.141 This was widely publicised as ‘Freedom Day’ – to the dismay of many vulnerable people, who continued to face increased risks of serious illness and death.142 It was marked by what became known as the ‘pingdemic’, as a consequence of the high number of infections and prevalence, which resulted in the NHS COVID-19 app (launched in England and Wales in September 2020, with a Bluetooth-based contact tracing functionality) notifying large numbers of people to self-isolate.143 This had significant impacts across the economy and more generally.144 |
| 8.53. | On 22 July 2021, SAGE noted that levels of hospitalisations in England were broadly in line with the COVID-19 Response – Spring 2021 roadmap modelling. It reiterated the importance of contingency plans and the threat of new variants. It welcomed a report, commissioned by Professor Vallance, on preparing for winter and advised that the report’s recommendations should be considered by government departments.145 The previous day, following a policy meeting to review risks for winter, Professor Vallance recorded in his evening notes that nobody had looked at the report and “once again DHSC [the Department of Health and Social Care] had done nothing“.146 The report warned of the potential for Covid-19, a flu epidemic and a rise in other seasonal illnesses arising in the winter. It set out a detailed plan of action.147 SAGE advised that, while there was “an understandable and intense desire for ‘normality’ to return“, efforts needed to be sustained “to limit the spread of the disease and the harm it can cause this year and beyond“.148 |
| 8.54. | From 22 July 2021, Covid-O considered the response to the high prevalence of infection in the summer. The main risks identified included pressures on the test, trace and isolate programme and genomic sequencing capacity, travel and borders, high-risk settings and NHS pressures.149 Long Covid was noted in the context of workforce absence.150 NHS pressures presented both demand and supply challenges, with a resurgence of demand on urgent and emergency care pathways. There were further pressures from increasing hospital admissions, the backlog of electives and on the ambulance services.151 |
| 8.55. | In Northern Ireland, on 22 July 2021, case numbers and hospital inpatient numbers were increasing rapidly.152 A lower percentage of the Northern Ireland adult population had received a first dose of vaccination compared with the rest of the UK.153 Consequently, Northern Ireland was “at risk of a bigger wave proportionally than the rest of the UK, by as much as 50%“.154 There was “considerable uncertainty” as to whether it was following the central or pessimistic modelling scenario and sufficient data and analysis would not be available until the end of July.155 The Department of Health (Northern Ireland) advised that it would be preferable to wait until it was clear which trajectory Northern Ireland was following before deciding on further relaxations.156 Nonetheless, the Executive Committee decided on 22 July to ratify three further relaxations from 26 July. For example, up to 15 people from different households were permitted to meet outdoors.157 On 26 July, ministers agreed the relaxation of a further five restrictions to take effect on 27 July.158 Professors McBride and Young cautioned that:
“[T]he risk of relaxations needs to be considered in the context of COVID prevalence, which is currently close to an all-time high.“159 |
| 8.56. | Cases in Wales had increased rapidly since the beginning of June, but data suggested that rates might be beginning to decline by 29 July 2021. Pressure on the NHS remained below previous waves. On 2 August, Dr Atherton advised that the rate of infection was stable. A total of 80% of the Welsh population was now fully vaccinated. The Welsh Cabinet confirmed the move to Alert Level 0 from 7 August.160 |
The situation at the end of July 2021
| 8.57. | By the end of July, an estimated 1 in 75 people in England had Covid-19. In Scotland, this figure stood at 1 in 120, in Wales it was 1 in 230, and in Northern Ireland it was 1 in 55.161 By the start of August 2021, 72% of adults aged 18 and over had received two doses of the vaccine in England, Scotland and Northern Ireland.162 By 7 August, in Wales, 81% of people aged 16 and over were fully vaccinated.163 |
| 8.58. | There was an openness across the four governments throughout this time to accept greater risk and manage the consequent increase in cases through less stringent restrictions. This high-prevalence strategy brought with it enhanced risks of variants that escaped natural or vaccine immunity and increased infections, hospitalisations and deaths, albeit tempered by the vaccine’s impact on severity. The Inquiry saw no evidence to suggest that any of the governments had explicitly agreed a tolerable level of infection and deaths, but such calculations are inherent to the pursuit of a high-prevalence strategy. |
| 8.59. | However, by this time, the public across the UK had been under some form of restrictions for over a year. The UK government and devolved administrations were attempting to balance the risk of emerging variants with the desire to return ‘normal’ life to the public and the substantial economic and social harms caused by the restrictions. |
| 8.60. | The emergence of the Delta variant, with increased transmissibility, was a significant public health threat and necessitated a reappraisal of the timetable for relaxing restrictions during the summer of 2021. To allow for further vaccine uptake and consequent protection from serious illness or death, the UK government and the devolved administrations made changes to their initial plans by delaying the relaxation of measures. The scientific advice on the benefits of such a delay was clear and the governments sensibly heeded that advice. This was appropriate – the risks were not worth taking for the sake of a few weeks. It inevitably prevented some deaths. |
| 8.61. | However, while the UK government heeded the advice to delay the relaxation of measures, it chose not to follow the additional scientific advice with regard to maintaining baseline measures. This included even those measures that were relatively modest. Instead, it relied on communications. Throughout this period, Professors Whitty and Vallance:
“had to make the point repeatedly that ‘we were not there yet’, and that the prospect of future population immunity did not mean that all of the brakes could be rapidly released“.164 |
| 8.62. | The tensions for the UK government were acute. However, the consequence of these decisions meant that the autumn and winter challenges, including any resurgence, would be set against a starting point of high levels of infections and hospitalisations. Ministers were advised that a very rapid return to normal behaviour could lead to a peak in hospitalisations similar to, or possibly higher than, previous peaks. This was a known risk and, by its decisions, one that the UK government was willing to take. It was a reasonable approach in light of the competing economic and social concerns and the comparatively low number of deaths. |
| 8.63. | There was, however, limited long-term planning, with no overarching strategic plan, aims or objectives, or proper consideration as to the potential impact of this approach. A plan for the autumn and winter of 2021 was not prepared by the UK government until September 2021. Had an active decision been taken on the tolerable level of infections and deaths, or a broad aim identified, it would have been significantly easier to make contingency plans. |
| 8.64. | Professors McBride and Young had advised the Northern Ireland Executive of the need for an incremental approach to the relaxation of restrictions and of significant uncertainties inherent in modelling.165 The Executive Committee had also been advised that sufficient data and analysis would not be available until the end of July 2021.166 Nevertheless, on a number of occasions between May and July 2021, the Executive Committee decided to relax restrictions despite contrary advice from the Department of Health (Northern Ireland).167 While, of course, it was appropriate for the Executive Committee to take into account a wider set of considerations, such as economic and social impacts, it was clear from the advice it had been given that the relaxation of restrictions – in the absence of sufficient data to permit analysis of the direct health impacts – was fraught with risk. |
| 8.65. | On 1 May 2021, Scotland had only 3 cases per 100,000 of the population, which was fewer than both England and Northern Ireland.168 However, between 14 May and 9 July, Scotland had the highest incidence of Covid-19 in the UK, peaking at 61 cases per 100,000 of the population on 3 July. Around this time, World Health Organization figures placed Scotland as one of the top Covid-19 hotspots in Europe.169 By 31 July, the number of cases had decreased to 21 cases per 100,000 of the population, which was comparable with Wales and significantly lower than England and Northern Ireland. The number of deaths in Scotland remained stable until around 15 July, at which point the daily deaths from Covid-19 doubled to around seven or eight each day.170 Professor Jason Leitch, National Clinical Director and Co-Director of the Directorate for Healthcare Quality and Improvement in the Scottish Government from January 2015, attributed this spike in positive cases in Scotland to a lack of “natural immunity” (immunity through prior infection) in the population.171 Similarly, at its meeting on 13 July, the Scottish Cabinet noted that relatively high figures for Scotland compared with the rest of the UK were thought to reflect that Scotland had been “behind and below” infection levels during the previous two waves but now appeared to be “above and ahead” of the rest of the UK in terms of the spread of the far more transmissible Delta variant.172 |
| 8.66. | Despite the significant increase of cases in Scotland from the middle of May 2021, the Scottish Government continued with the planned relaxation of restrictions, but with some modifications. The Scottish Government’s approach, based on advice, was to ease restrictions “at a careful and gradual pace, in order to minimise demands on the NHS – both now and in expectation of autumn/winter pressures“.173 The Scottish Government was less cautious at this time because of a desire “to move away from Government direction to a point where people make decisions themselves” and concerns about “losing the dressing room” if stricter measures were imposed.174 Such an approach was reasonable in light of the need to balance the other economic and societal harms caused by the restrictions and the fact that prevalence of the virus was higher among younger people. This meant that deaths remained relatively low, despite the increasing cases. |
| 8.67. | The Welsh Government agreed indicative dates to remove restrictions, but at various points it paused to await further information about the new variant and to allow greater vaccine uptake before further easing restrictions, including delaying the full move to Alert Level 1. This was also a reasonable approach in light of uncertainty and, at this stage in the pandemic, each government was entitled to weigh up the competing harms within its own nation. Wales did not see a sharp increase in death rates throughout July 2021. Pressures on the NHS and death rates remained significantly lower than in previous waves. In those circumstances, by 7 August 2021, it was reasonable for the Welsh Government to conclude that a move to Alert Level 0 was appropriate, having received advice that direct harm from infections was beginning to be outweighed by the other harms caused by restrictions and that vaccines had weakened the link between infection and severe illness. |
August to October 2021
| 8.68. | On 1 August 2021, The Executive Office published Building Resilience Together: NI Civil Contingencies Framework, which set out the Northern Ireland arrangements for emergency management and replaced a number of former protocols and guidance documents.175 Northern Ireland’s civil contingencies arrangements had, prior to this, not been reviewed in over 20 years.176 This had been acknowledged within The Executive Office in February 2020, when a strategic review of the civil contingencies arrangements within Northern Ireland had been proposed.177 The development of an up-to-date and consolidated civil contingencies framework for Northern Ireland was an appropriate step, albeit one which was far too late by August 2021. |
| 8.69. | Cases began to rise in August 2021 across the four nations. Deaths still remained low compared with previous waves but, by September, hospitals across the UK were under significant pressure, with Northern Ireland and Scotland facing acute pressures. |
Figure 32: Estimated percentage of the population testing positive for Covid-19 from 1 August to 31 October 2021 across the UK
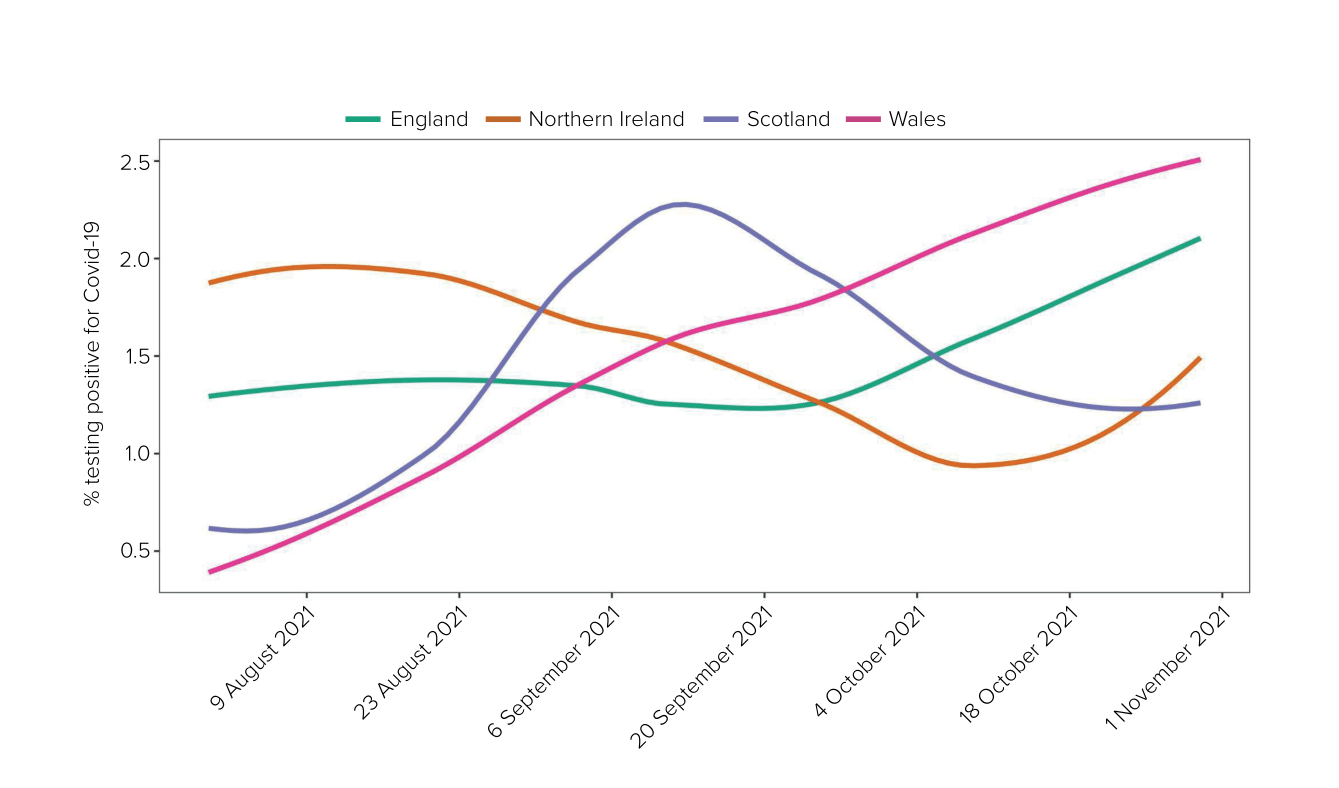
Source: Coronavirus Infection Survey from 1 August to 31 October 2021 (Modelled estimates, 95% confidence intervals not shown). For raw data, see the Coronavirus (COVID-19) Infection Survey: England, dataset, Office for National Statistics, 10 March 2023 (https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/coronaviruscovid19infectionsurveydata/2023)
| 8.70. | On 11 August 2021, only eight intensive care unit beds were available in Northern Ireland, with Covid-19 accounting for nearly half of all intensive care admissions and ventilated patients.178 At its meeting on 12 August, the Executive Committee was advised that adult vaccination remained lower in Northern Ireland than elsewhere and that, in the circumstances, it was not recommended that relaxations proceed at the same rate as the rest of the Common Travel Area.179 The Executive Committee agreed to a number of relaxations (including removing the ban on large, outdoor house parties, removing the rule of six in hospitality settings and removing ‘bubble’ provisions) but retained several restrictions. It was agreed that the Executive Committee would consider the remaining restrictions at its next meeting.180 |
| 8.71. | On 1 September 2021, the hospital system in Northern Ireland was operating at 106% bed capacity with a waitlist.181 While the number of new positive cases had begun to decline, Northern Ireland had the highest prevalence of Covid-19 in the UK, with 1 in 40 people infected.182 Professors McBride and Young advised that hospital pressures would remain considerable when prevalence was high, particularly given increasing evidence of waning immunity after natural infection or vaccination. Adult vaccination coverage also remained lower in Northern Ireland.183 Despite this and advice to the contrary, on 6 September the Executive Committee agreed to relax a number of restrictions, including increasing the maximum number of people who could meet indoors in a domestic setting to 15 from up to 4 households.184 |
| 8.72. | In Scotland, by 30 August 2021, Covid-19 cases had virtually doubled each week since the lifting of restrictions on 9 August, leading to an increase in hospitalisations and the cancellation of non-urgent procedures.185 It was reported that, according to World Health Organization figures, Lanarkshire’s and Glasgow’s health board areas had Europe’s highest case rates.186 At this point, Scotland had moved beyond Level 0 to a set of ongoing baseline measures and the use of temporary, targeted responses.187 These baseline measures were legal requirements and included the wearing of face coverings in most indoor public settings and on public transport (unless exempt), the gathering of contact details in hospitality settings so that Test and Protect (Scotland’s testing programme) could continue to contact-trace positive cases, and the setting of capacity limits on live events.188 Ms Sturgeon publicly stated that the Scottish Government was not considering the introduction of a ‘circuit breaker’ lockdown.189 The Scottish Cabinet met on 31 August and considered two scenarios: one in which cases would peak within a fortnight without further intervention, and a second in which cases continued to rise and required the reintroduction of restrictions.190 It agreed not to impose further restrictions but to continue to monitor the situation.191 |
| 8.73. | By 14 September 2021, the Scottish Cabinet noted that pressures on the NHS were at an “extremely high level” and that there might yet be a need to reimpose more stringent restrictions in due course.192 On 16 September, Ms Sturgeon described the situation to the Scottish Parliament as being the most challenging set of circumstances in NHS Scotland’s history.193 Scotland had the highest Covid-19 daily infection rate in the UK in the week ending 11 September and daily deaths were at comparable levels to February 2021, with 135 deaths involving Covid-19 recorded in the week ending 19 September.194 |
| 8.74. | The number of deaths and hospital admissions in England was described through this period as remaining “relatively stable although the rates were high“.195 Mr Javid reported in September 2021 that the NHS was “currently coping, and coping well, but there would be higher pressures to come“.196 |
| 8.75. | Deaths in Wales continued to “remain very low compared with previous waves“.197 Public Health Wales had advised that the focus of the Welsh Government should “shift to the impacts of Covid rather than case numbers“.198 The Welsh Cabinet agreed that Alert Level 0 should be retained.199 By 17 September 2021, there had been a rise in hospital numbers, deaths and pressures on the NHS.200 |
| 8.76. | It was in this context that autumn and winter planning commenced. The scientific advice was that the pandemic was “entering a period of uncertainty“.201 SAGE and SPI-M-O advised that hospital occupancy and deaths were lower than expected.202 Behavioural change following Step 4 had been slower than anticipated and it was increasingly unlikely that the peak of the January 2021 wave would be reached.203 There was, however, evidence of waning vaccine effectiveness. They advised that it was likely that there would be a delay in the timing of peaks later in October to December 2021, with possibly “broader, longer peaks” and the potential for another large wave of hospitalisations.204 While vaccination had changed the relationship between infection and hospitalisation, rising infections would remain “the earliest warning sign that hospital admissions are likely to rise“.205 Advice was reiterated regarding early interventions to curb growth and prevalence, noting that a relatively light set of measures could be sufficient if enacted early.206 |
| 8.77. | Planning work for the autumn and winter response had been due to commence at the end of June 2021 but in fact began after the announcement of a move to Step 4 of the COVID-19 Response – Spring 2021 roadmap and “in earnest” in August 2021.207 It is unclear why this planning was delayed – it would have been better for the planning to run alongside the roadmap. The aim was to shift from “crisis to active management“, with departmental plans in place to respond to any surge in Covid-19 alongside managing recovery.208 The Covid-19 Taskforce advised that the COVID-19 Response – Spring 2021 roadmap should not be reversed – the aim was to live with Covid-19 without the need for increased interventions.209 |
| 8.78. | The UK government subsequently published COVID-19 Response: Autumn and Winter Plan 2021 on 14 September 2021, following its approval at Covid-O and the UK Cabinet.210 The plan explained that the country was learning to live with Covid-19. The main line of defence was “vaccination rather than lockdown“.211 It provided for ‘Plan A’ and a more pessimistic, contingency ‘Plan B’ to be used only if it was needed to protect the NHS from coming under unsustainable pressure. Plan A was described as a comprehensive approach. Interventions were minimal, with an emphasis on:
|
| 8.79. | Plan B provided for the reintroduction of face coverings, public health communications focused on risk and behaviours and potential mandatory vaccine certification for nightclubs and mass events. Consideration would also be given to asking people to work from home if necessary.213 The UK government stated that it remained:
“committed to taking whatever action is necessary to protect the NHS from being overwhelmed but more harmful economic and social restrictions would only be considered as a last resort“.214 The UK government should have understood, by this time and given previous experience, that the modest measures outlined in Plan B were unlikely to deal adequately with a more transmissible or lethal variant evading natural or vaccine-induced immunity. |
| 8.80. | The document noted the SPI-M-O and SAGE advice, in that they considered the most pessimistic modelling to be unlikely except in the case of a new variant of concern or “significant waning immunity“, but it warned that “scenarios which place the NHS under extreme and unsustainable pressure remain plausible“.215 |
| 8.81. | On 17 September 2021, following a request from Mr Javid, the Joint Committee on Vaccination and Immunisation announced the rollout of the booster vaccine programme for the winter of 2021 for the most vulnerable groups.216 |
| 8.82. | On 8 October 2021, the Welsh Government published the Coronavirus Control Plan: Autumn and Winter 2021 Update.217 It outlined two scenarios: ‘Covid Stable’ would not require the reimposition of significant restrictions; however, ‘Covid Urgent’ may be caused by unexpected pressures such as a new and highly transmissible variant, which would necessitate more “significant action“.218 This reflected a recommendation from the Technical Advisory Group.219 While it stated that “our response to these challenges will not be to simply return to lockdown measures or to impose new restrictions“, the plan for a Covid Urgent scenario was predicated on the basis of retaining:
“the coronavirus restrictions regulations, which set out the alert levels and enable us to move up and down the levels, depending on the specific risk to public health that is identified“.220 Annex A to the plan contained a list of key indicators that would be monitored.221 It would have been of even greater benefit if these indicators had clearer thresholds for the Welsh Government to consider further action. |
| 8.83. | In Northern Ireland, on 7 October 2021, the Executive Committee endorsed an autumn and winter contingency plan.222 Its premise was that the pandemic could change course rapidly and unexpectedly. It therefore set out measures that could be deployed “to contain the virus or to respond to surges or pressures that may emerge” while minimising economic and social impacts.223 The document recognised that the early introduction of ‘low-cost’ interventions would help to avoid unacceptable hospital pressures and more disruptive interventions at a later stage.224 |
| 8.84. | In contrast, the Scottish Government continued to operate in terms of Scotland’s Strategic Framework Update, published on 22 June 2021.225 This document set out plans for the easing of restrictions to beyond Level 0, when all levels’ restrictions and physical distancing regulations would be lifted in Scotland, with the indicative date of 9 August 2021. The strategic framework did not contain plans for the autumn and winter of 2021 and was not updated again until 16 November, over a month after the other three governments had updated their pandemic response plans for the autumn and winter. The Scottish Government appears to have delayed devising its autumn and winter strategic plans.226 |
| 8.85. | Instead, on 5 October 2021, the Scottish Government published its Covid Recovery Strategy, which noted that the success of the vaccination programme and the summer 2021 “lifting of restrictions has provided the platform for recovery“.227 The Scottish Government’s focus was now shifting to “the next 18 months” and the need to seize the “opportunity to drive a more positive change“.228 The document set out actions to address inequalities made worse by Covid-19, to make progress towards a “wellbeing economy” and to accelerate inclusive, person-centred services.229 John Swinney MSP (Deputy First Minister of Scotland from November 2014 to March 2023) had been appointed as Cabinet Secretary for Covid Recovery after the Scottish Parliament elections in May 2021. He explained that his appointment was:
“a recognition by the First Minister that we needed to ever more turn our attention to recovering from Covid and to make sure there was a whole-government response in a co-ordinated and cohesive way to that effort“.230 Although it was proper for the Scottish Government to focus on recovery from the pandemic, the prevailing attitude was to focus too much on recovery to the exclusion of the still present threat and the timely development of autumn and winter plans. |
| 8.86. | On 14 October 2021, SAGE warned that “there should be no complacency around the risk posed by further viral evolution“.231 It was a “real possibility” that a further variant would become dominant globally.232 As had been seen with Alpha and Delta, variants were emerging with increased transmissibility, but there were also concerns that, for some variants, the vaccines would be less effective or would cause more severe disease. SAGE reviewed Plan B and advised that policy work on the reintroduction of restrictions “should be undertaken now so that it can be ready for rapid deployment if required“.233 It noted that other “measures beyond those proposed as part of Plan B are available to mitigate the need for further measures over winter“.234 This endorsed SPI-M-O’s advice that “action beyond Plan B may be required to control growth“.235 |
| 8.87. | SAGE’s advice about efficacy, early deployment of measures and the use of triggers was repeated. This was less than a month after Plan A had been announced. As Professor Vallance observed: “[T]hese were common and repeated themes of SAGE advice which had been reinforced by the experience of previous waves.“236 |
| 8.88. | On 25 October 2021, this advice was reinforced by Professors Whitty and Vallance to Simon Ridley (Head of the Cabinet Office Covid-19 Taskforce from July 2021 to March 2022). The “main ministerial objective” was understood to be preventing NHS ‘overwhelm’.237 They advised that pressures on the NHS would inevitably worsen over the winter period. They considered that the measures in Plan B, combined with good immunity from ongoing vaccination, would:
“likely be enough to take the edge off things and allow numbers of infections to decrease. The earlier action is taken the less severe the measures need to be.“238 Despite this – and Mr Johnson having already acknowledged privately as early as 9 October that Plan A was “clearly not working and time for plan b” – as addressed below, the decision to move to Plan B in England was not taken for a further two months.239 |
| 8.89. | Throughout October 2021, Wales had the highest infection rates of the four nations. Higher case rates had begun to translate into increased hospital occupancy; however, this remained significantly lower than in previous waves.240 The Welsh Cabinet discussed ways to avoid moving to its Covid Urgent scenario and agreed that messaging should encourage people to take precautions and explain that there may be a need to tighten restrictions in the future. On 29 October, more stringent rules on self-isolation were announced.241 This was a sensible precaution. |
The situation at the end of October 2021
| 8.90. | Although the vaccine rollout was reducing rates of deaths and serious illness, the higher rates of transmission of the Delta variant meant the number of cases continued to climb. On 31 October 2021, Wales had the highest number of infections, with the infection rate being an estimated 81 cases per 100,000 people. The comparative figure was 60 for each of England and Northern Ireland and 48 for Scotland.242 While the number of patients in hospital and intensive care and the deaths due to Covid-19 increased, these remained substantially lower than in previous waves.243 |
| 8.91. | Restrictions had, understandably, given way to efforts to balance and alleviate indirect harms, which in themselves were significant. In this respect, the UK government and devolved administrations relied heavily on the success of the vaccine rollout. By the end of October 2021, the percentage of adults aged 18 and over who had received two doses of the vaccine stood between 84% and 88% across the four nations.244 However, the booster vaccination programme for vulnerable groups was only introduced in mid-September 2021, despite growing concerns about waning immunity.245 |
| 8.92. | The period was marked by increasing pressure on health service capacity across the four nations.246 This underscored the importance of planning ahead for a difficult winter. |
| 8.93. | The aim in England was to manage surges alongside recovery and to live with Covid-19 without the need for increased interventions.247 As such, there was to be no return to more stringent restrictions as implemented earlier in the pandemic. This was an optimistic approach, given the potential for variants of concern to emerge and the known seasonal issues. The better approach would have been for full contingency plans to have been drawn up to enable a swift and flexible response, if necessary. A more lethal and vaccine-evading variant was a realistic possibility and comprehensive plans should have been made accordingly. |
| 8.94. | In establishing Covid Urgent, the Welsh Government acknowledged that it might need to respond urgently to a new variant or waning vaccine immunity by the implementation of significantly more stringent measures to avoid unsustainable pressure on the NHS. This was useful as a communication tool to remind the public that the risks from Covid-19 were not yet over. The Welsh Government also confirmed publicly that, if the situation deteriorated, further restrictions could be needed.248 However, the response under a Covid Urgent scenario did not envisage anything other than a return to the suite of restrictions that had been used to respond in other waves of the pandemic. |
| 8.95. | The approach of the Scottish Government over this period had changed from its position in the summer of 2020, when it had sought maximum suppression of the virus in Scotland. The greater focus on recovery and non-Covid-19 harms during this period meant that more stringent measures were not introduced. |
| 8.96. | The Northern Ireland Executive eased restrictions at a slower pace across this period. This was a comparatively cautious approach to that taken previously and was understandable in the context of uncertainty as to the potential impact of the Delta variant. The Executive Committee’s Autumn/Winter COVID-19 Contingency Plan recognised the possibility that case numbers might rise sharply or that hospital pressures might become unsustainable.249 While the plan set out potential contingency measures that could be used in those circumstances, these were limited and included only a bare reference to the possible “re-imposition of a legal requirement for minimum social distancing in prescribed settings“.250 Given the uncertainty at the time, detailed contingency plans were required. |
| 8.97. | Throughout this period, Delta had been the dominant variant, but concerns relating to potential new and evolved variants continued to feature heavily in scientific advice.251 |
Omicron: November and December 2021
| 8.98. | As the UK moved into the winter period, the situation in the UK was one of high but stable prevalence.252 It was in this context that the Omicron variant emerged. It was to fuel exponential growth in cases across the four nations. |
Figure 33: Estimated percentage of the population testing positive for Covid-19 from 31 October to 31 December 2021 across the UK
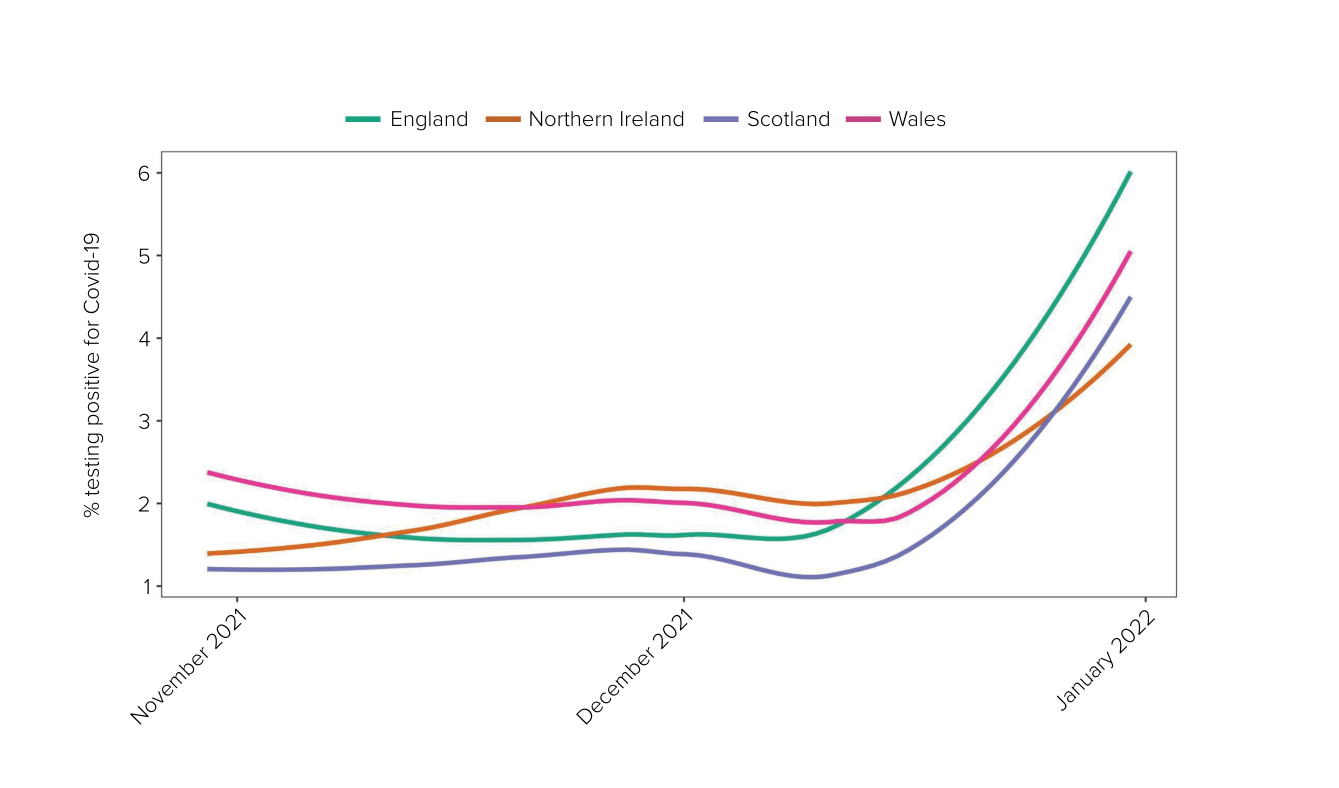
Source: Coronavirus Infection Survey from 31 October to 31 December 2021. (Modelled estimates, 95% confidence interval not shown). For raw data, see the Coronavirus (COVID-19) Infection Survey: England, dataset, Office for National Statistics, 10 March 2023 (https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/coronaviruscovid19infectionsurveydata/2023)
Figure 34: Daily deaths per 100,000 population by date of death from 31 October to 31 December 2021 across the UK
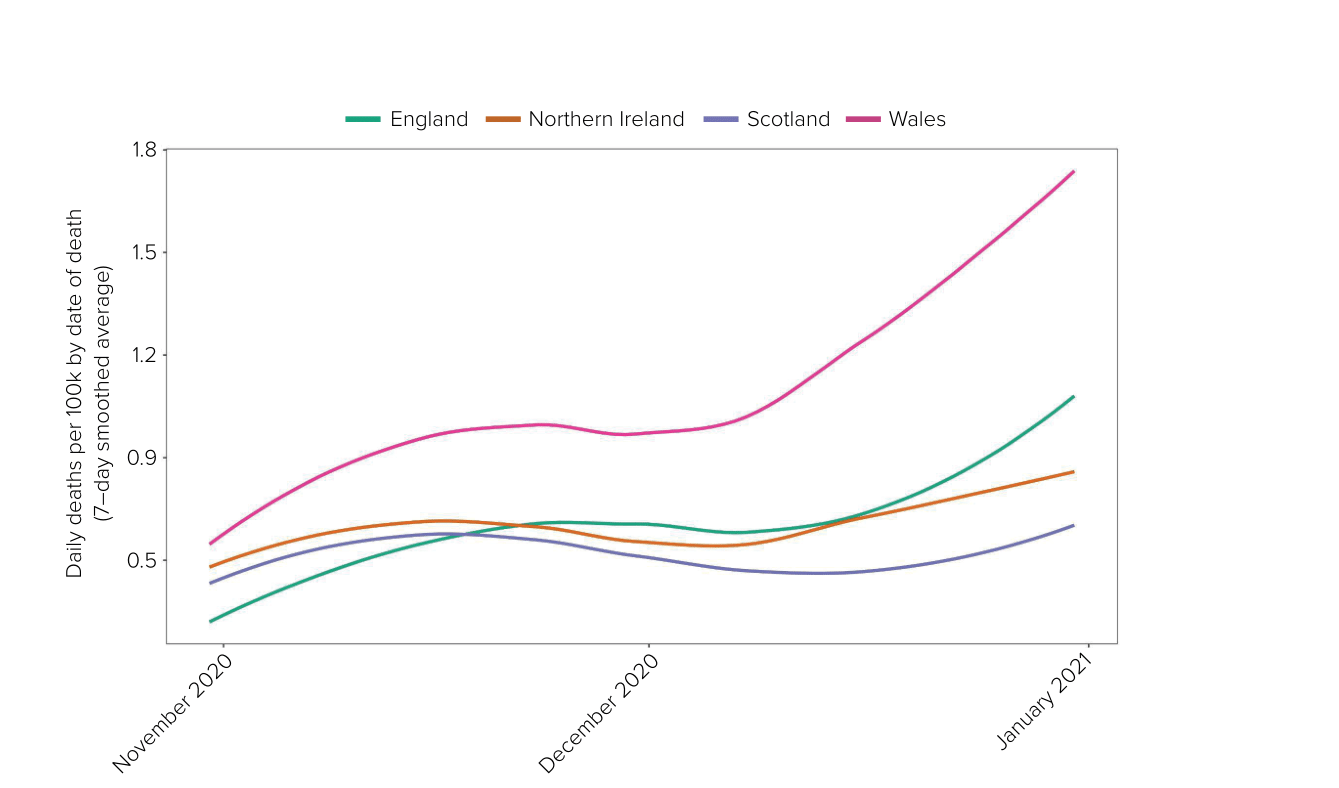
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 8.99. | The Omicron variant was reported to the World Health Organization on 24 November 2021 after detection in South Africa. It was highly transmissible, with an alarming growth rate – it doubled every two to three days.253 This meant that it could – and did – lead to a significant number of cases in a short period of time. |
| 8.100. | The Omicron variant spread across several countries quickly. The first two cases in the UK were identified within days in England on 27 November 2021.254 Six of the first eleven cases were found in Scotland.255 The first cases in Wales and Northern Ireland were reported on 3 December and 7 December respectively.256 The wave peaked on 4 January 2022, with 275,647 confirmed cases and an estimated 5 million people infected across the UK.257 It led to further large peaks in hospitalised patients across the UK, reaching a high of 20,176 on 6 April, although far fewer needed admission to an intensive care unit or died of Covid-19 than in the initial waves.258 Ultimately, although the Omicron variant caused less severe illness (especially in a vaccinated population), the sheer volume of infections led to 30,000 people dying with Covid-19 in the UK between November 2021 and June 2022.259 |
| 8.101. | The sense of alarm was apparent within the scientific community. The New and Emerging Respiratory Virus Threats Advisory Group (NERVTAG) convened an extraordinary meeting on 25 November 2021.260 Professor Vallance recorded in his evening notes that Professor Van-Tam (observing) had never “seen NERVTAG so rattled“.261 The R number for the Omicron variant was estimated to be 1.9 against a backdrop of high levels of immunity (following the Delta variant and immunisation) in South Africa. It noted that, while there was “substantial current uncertainty” about the characteristics of the Omicron variant, there were “sufficiently worrying signals“.262 NERVTAG advised that it could not rule out a large wave of infections, accompanied by a wave of severe cases, which could be sufficient to overwhelm the NHS.263 The introduction of the Omicron variant “into the UK might have very serious consequences and, therefore, early and aggressive actions to prevent introduction and onward transmission” were warranted.264 |
| 8.102. | Covid-O also met on 25 November 2021. No cases of the Omicron variant had yet been detected in the UK but they had been detected in South Africa, Botswana and Hong Kong – the latter relating to travel from South Africa.265 Professor Whitty warned that the new variant had a worrying number of mutations and was spreading very quickly in a highly immune population. He advised a cautious approach.266 Immediate actions, including the temporary suspension of flights from southern Africa, the addition of a number of southern African countries to the ‘red list’ (countries posing a high public health risk to the UK) and polymerase chain reaction (or PCR) testing for recent arrivals were agreed.267 Tensions about the approach to be taken were once again apparent. Mr Javid described the relationship as “testy” because of the Omicron variant.268 Professor Vallance recorded in his evening notes:
“Afterwards, No 10 says they are at war with No 11 + that anything Javid says they assume is wrong. They say they are missing Gove.“269 |
| 8.103. | A number of meetings were held on 27 November 2021 to consider the response in England.270 At Covid-O, in addition to the earlier measures, it was decided that arrivals into the UK would have to self-isolate and undertake a PCR test on the second day of their arrival, with a negative test result allowing them to end their self-isolation.271 Mr Javid had sought to extend the measures to a period of 10-day self-isolation, with testing at days 2 and 8. However, this was rejected on the basis of economic concerns and the risk of undermining the benefits of vaccination.272 Covid-O further agreed that contacts of a suspected Omicron variant case would be required to self-isolate for 10 days, face masks would be required in shops and on public transport (but not in hospitality settings) and that the booster vaccination programme would be expedited, with Mr Javid having asked the Joint Committee on Vaccination and Immunisation to look at reducing the time between the second dose and the booster.273 The Cabinet was updated.274 The Covid-19 Taskforce was to coordinate a review of all measures by 17 December. |
| 8.104. | Mr Johnson informed the public of the new variant and the temporary measures to be implemented in a press conference on 27 November 2021.275 |
| 8.105. | Ms Sturgeon and Mr Yousaf preferred a different approach, requiring all travellers to self-isolate for 10 days, even as a short-term measure. In a WhatsApp exchange with Ms Sturgeon, Mr Yousaf noted that the UK government wanted to stick to a PCR test on day two of self-isolation and that “[i]t is very clear they are going against the public health advice they’ve received“.276 Ms Sturgeon noted that:
“If we go to 10 days we’ll be back in position of people just flying into England. So we don’t get health benefit but we cripple our airports.“277 Ms Sturgeon and Mr Yousaf concluded that they would be “reluctantly aligning” with the UK government measures due to the practical difficulties of taking a different approach.278 Ms Sturgeon requested that the Four Harms Group start work on possible scaling up of protections, such as social distancing and working from home.279 |
| 8.106. | At its meeting on 29 November 2021, SAGE was concerned about the likely increased transmissibility as well as the potential that the Omicron variant could escape from natural or vaccine-induced immunity, given the manner in which it had spread in South Africa and the potential consequent impacts on severity.280 SAGE noted that, even with good protection against serious disease from vaccination:
“[A]ny significant reduction in protection against infection could still result in a very large wave of infections. This would in turn lead to potentially high numbers of hospitalisations even with protection against severe disease being less affected. The size of this wave remains highly uncertain but may be of a scale that requires very stringent response measures to avoid unsustainable pressure on the NHS. If vaccine efficacy is substantially reduced, then a wave of severe disease should be expected.“281 SAGE emphasised the need to act ahead of the data being available and warned about a quickly developing situation and the importance of being prepared “for a potentially very significant wave of infections with associated hospitalisations now“.282 As previously, SAGE advised that border measures could not completely prevent the introduction of variants into the country but could be effective in delaying the subsequent wave to allow time for further preparations – for example, increasing vaccination coverage.283 |
| 8.107. | On 29 November 2021, the Welsh Cabinet was advised that the Omicron variant was more transmissible than the Delta variant, but it was not known whether it was more harmful or if it had the potential for vaccine escape.284 The same day, the Joint Committee on Vaccination and Immunisation recommended that boosters should be offered to everyone aged over 18, and that the minimum gap between the second dose and the booster be halved to three months.285 |
| 8.108. | The UK Cabinet met on 30 November 2021.286 Cases of the Omicron variant remained low, with 5 confirmed and 10 highly probable. There were, however, more than 100 suspected cases. Mr Javid advised that the UK government should be prepared for a rise in case numbers. In England, all cases were linked to travel. However, in Scotland, there was the possibility of transmission in the community. The expedited booster vaccination programme had a target of immunising those eligible by the end of January 2022. Mr Johnson stated that it was important to take urgent steps to slow down the Omicron variant and especially to limit travel.287 If the variant did evade vaccine immunity, there would be a “big problem. However, it was also important not to overreact.”288 This was, in his view, a proportionate response.289 That same day, the press reported details of alleged rule-breaking in 10 Downing Street, which became known as ‘partygate’.290 This is discussed further in Chapter 11: Government decision-making, in Volume II. |
| 8.109. | On 30 November 2021, the Scottish Cabinet agreed to consider the response to the Omicron variant on a weekly basis.291 Ms Sturgeon confirmed that all nine cases of the Omicron variant found in Scotland were linked to a single event on 20 November. She suggested that this meant that there was “limited” but not “sustained or widespread” community transmission of the Omicron variant in Scotland.292 An emergency meeting of the Scottish Government Covid-19 Advisory Group took place on 2 December. It recognised:
“[W]e don’t have enough information but by the time we get it the need to act could well be acute. Intervening early could mean not needing to intervene more drastically.“293 |
| 8.110. | Also on 2 December 2021, the Northern Ireland Executive decided that current restrictions remained appropriate and it scheduled a further review for 13 January 2022.294 |
| 8.111. | On 4 December 2021, Covid-O considered further travel and border restrictions.295 The Covid-19 Taskforce was tasked to provide analysis on an exit strategy.296 By 6 December, there were 197 confirmed Omicron variant cases in England (in six of the nine regions), 48 in Scotland and 1 in Wales. The UK had the second highest number of reported, confirmed Omicron variant cases internationally. The numbers were expected to rise.297 |
| 8.112. | SAGE convened again on 7 December 2021.298 The Omicron variant was increasing rapidly, and daily infections were thought likely to be in the thousands.299 Preliminary modelling suggested that, without changes to the measures in place:
“[T]he number of hospitalisations from Omicron may reach 1,000 per day or higher in England by the end of the year (and still be increasing at that point).“300 SAGE advised: “[D]ecision makers will need to consider response measures urgently to reduce transmission if the aim is to reduce the likelihood of unsustainable pressure on the NHS.“301 |
| 8.113. | The Scottish Cabinet agreed on 7 December 2021 that it did not yet appear to be proportionate to introduce further protective measures, although further measures might be required in the near future.302 Later that day, Ms Sturgeon announced plans to review Covid-19 protections on a daily basis.303 |
| 8.114. | On 7 December 2021, the Covid-19 Taskforce presented Mr Johnson with a number of options.304 The objective remained to avoid unsustainable pressure on the NHS. At that point, NHS England had about 97,000 beds – of which, 91,000 were occupied and 6,000 were Covid-19 patients. In the first and second waves, the NHS dealt with about 19,000 and 34,000 Covid-19 patients, respectively.305 |
| 8.115. | Early case growth in the UK was consistent with that seen in South Africa, which had experienced “extraordinary case growth“, at a rate steeper than for any other variant.306 A number of European countries had imposed more stringent measures in response to the Delta and Omicron variants – Germany was in lockdown.307 |
| 8.116. | There were three options: stick with Plan A (and warn the public about the Omicron variant), move to Plan B (with the option to strengthen, with Plan B+ involving expanded mandatory vaccine, test or immunity certification – to include entertainment and hospitality with mandatory check-in at such venues) or “go harder” with Plan C and revert to Step 2 of the COVID-19 Response – Spring 2021 roadmap.308 It does not appear that actual plans were developed for steps akin to Plan C or Step 2.309 It was acknowledged by the Covid-19 Taskforce that Plan B was “unlikely to bring Omicron sustainably under control if highly transmissible and/or vaccine escaping” and that further escalation might be required.310 Lateral flow testing capacity would also be strained.311 The taskforce advised that Plan C would “rapidly bring down Delta transmission and hospitalisations” – freeing up capacity for a possible Omicron variant wave – slow the Omicron variant and have the benefit of acting early if it escaped vaccine immunity.312 The taskforce recognised that the measures could be in place for a significant period of time and recognised the impact this would have on the economy and on mental health.313 |
| 8.117. | That same day, Mr Johnson told the Cabinet:
“[A]ny disease, however mild, that replicated that quickly and affected large numbers of people, would inevitably put pressure on the health system. This posed a significant problem.“314 The solution, in his view, was the booster vaccination programme.315 Mr Javid explained that it would be impossible to administer boosters to everyone within two weeks.316 Professor Whitty urged the UK government to “consider acting now“.317 The Omicron variant was doubling roughly every three days, which would lead “to big numbers fast“.318 The severity of illness was unclear, but it: “was clear from the modelling that it would have to be very substantially less severe than Delta to avoid unmanageable pressures on the NHS“.319 Professor Vallance concurred: “[A]ny gains from lower severity would quickly be overtaken by rapid exponential growth.“320 |
| 8.118. | On 8 December 2021, Mr Johnson chaired Covid-O. Previously, Covid-O had been chaired by Mr Gove as Chancellor of the Duchy of Lancaster. The data suggested community transmission, with rapid growth in the Omicron variant (particularly in London) and in hospitalisations.321 Mr Johnson considered that there “seemed little option than to implement Plan B. The reality was that they were running out of road,” echoing sentiments expressed in the winter of 2020.322 Professor Whitty advised there was a strong case for acting earlier. Due to the booster vaccination programme targeting the vulnerable groups first and the quick doubling times, “buying time at the start of the variant spreading had a disproportionately positive impact“.323 Summing up, Mr Johnson stated that the “country was facing a nightmare situation again“.324 Plan B was approved. These were temporary measures to be reviewed in advance of 5 January 2022.325 |
| 8.119. | That same day, in a UK Cabinet update call, Mr Johnson described the Covid-19 situation as “infuriating“.326 He noted that some would consider Plan B an “overreaction” – his view was that it was “moderate, proportionate and precautionary“.327 Professor Vallance described the effect of Plan B as a “behavioural change that would slow the spread … and buy time for the booster programme“.328 Once again, tensions had arisen between the Department of Health and Social Care and the Treasury, with Mr Javid unsuccessfully supporting measures in excess of Plan B, including legal requirements for check-in settings such as hospitality venues.329 Mr Gove was recorded, by Professor Vallance in his evening notes, as asserting that Plan B was not enough, but was said to have concluded that it was “pointless, no one is listening“.330 Professor Vallance described it as feeling “like March 2020 all over again“.331 |
| 8.120. | Plan B was announced on 8 December 2021, to commence in England on 10 December.332 Face coverings were required in indoor venues, working from home was encouraged from 13 December and the NHS COVID Pass (which allowed for the sharing of Covid-19 vaccination status) became mandatory for nightclubs and large gatherings from 15 December.333 These were similar to the restrictions already in place in Wales.334 |
Figure 35: Plan B measures announced on 8 December 2021
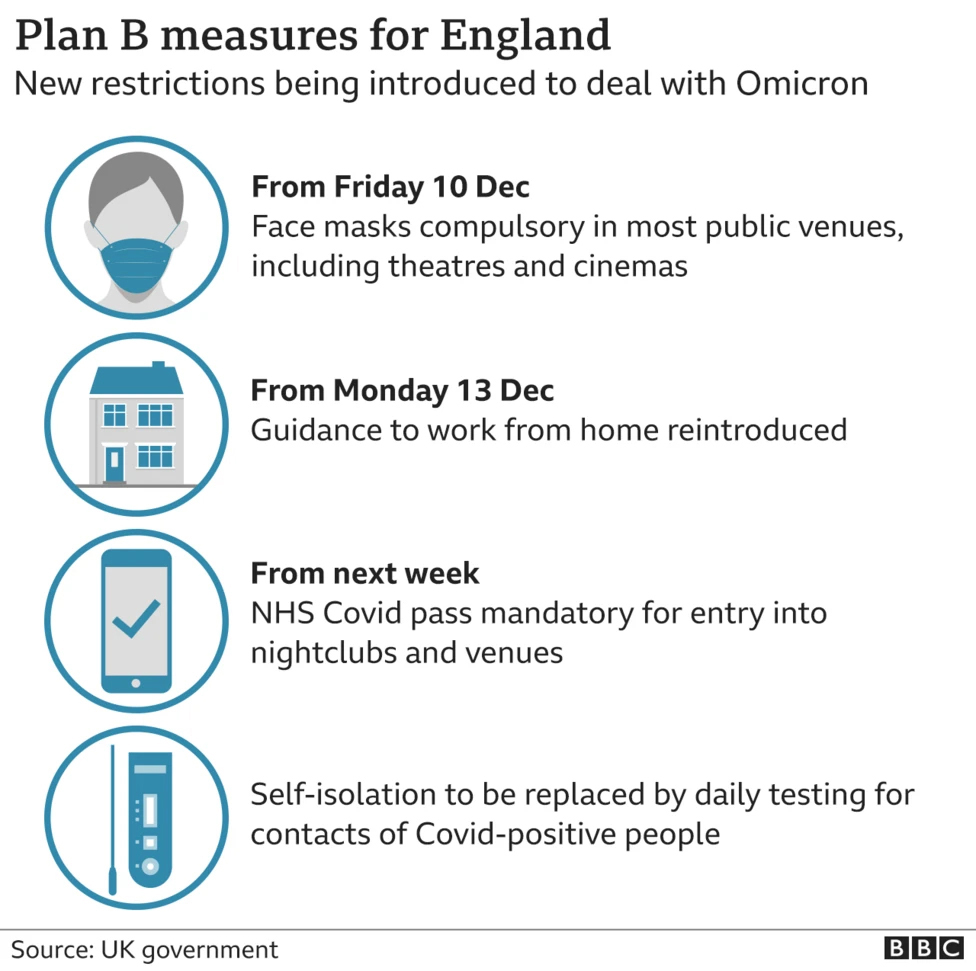
Source: ‘Covid: New Plan B rules on working from home and masks announced for England’, BBC News, 8 December 2021 (https://www.bbc.co.uk/news/uk-59585307; INQ000548020)
| 8.121. | The Welsh Government held Cabinet meetings to discuss the Omicron variant on 2, 6, 8 and 9 December 2021.335 On 2 December, Dr Atherton confirmed that the Delta wave “appeared to be plateauing“.336 It was hoped that Test, Trace, Protect and new self-isolation requirements would help slow transmission.337 Nonetheless, recognising the developing situation, the Welsh Cabinet agreed that restrictions should be reviewed weekly and it considered planning for a Covid Urgent scenario:
“[I]f there was a risk the NHS could become overwhelmed by COVID cases, Alert Level 4 should be the basis for the Government’s response.“338 It was, however, concerned that, without financial support from the UK government, “the economic harms from moving to Alert Level 4 would be much greater than in previous waves“.339 |
| 8.122. | On 8 December 2021, there were three cases of the Omicron variant in Northern Ireland and the hospital system continued to operate at over 100% of bed capacity.340 Professor Young advised the Northern Ireland Executive Committee on 9 December that the Omicron variant was likely to result in a steep rise in infections, although more data were required to determine the potential increase in hospital admissions and the efficacy of booster vaccines. He said that it was unlikely that Omicron could be prevented from becoming the dominant variant but that its spread could be delayed.341 |
| 8.123. | Also on 9 December 2021, Public Health Scotland urged people to cancel Christmas parties on the basis that some Omicron variant cases were linked to such parties.342 Ms Sturgeon indicated that Scotland faced a “tsunami” of Omicron variant cases.343 She warned the public that “once again we face a situation that frankly has no easy options“.344 Ms Sturgeon also announced that she would be pressing the UK government for financial support and announced changes to self-isolation rules.345 |
| 8.124. | A COBR meeting attended by the devolved administrations took place on 10 December 2021, chaired by Mr Gove. This was convened following a request to Mr Johnson from the Scottish and Welsh governments on 29 November for a meeting to discuss a four-nations approach.346 Professor Whitty stated that “infections [from the Omicron variant] were likely even for those who had two vaccines“, with doubling times between two and three days, and closer to two in parts of Scotland.347 Scotland was seeing a “rapidly deteriorating situation“.348 Both Wales and Northern Ireland had a small number of identified cases of the Omicron variant.349 |
| 8.125. | The same day, Mark Drakeford MS (First Minister of Wales from December 2018 to March 2024) stated that if Wales saw a situation:
“coming at us because of what we see happening elsewhere, that tells us that action needs to be taken, difficult as it is and upsetting as it can be“.350 This gave some expectation to the public that further measures might be necessary. Dr Atherton noted that Wales would “likely move to [Alert Level 4] prior to Xmas“.351 |
| 8.126. | On 12 December 2021, the Chief Medical Officers for the four nations and the NHS England National Medical Director advised that the UK coronavirus (Covid-19) alert level should be increased from Level 3 to Level 4.352 |
| 8.127. | That day, Mr Johnson chaired a UK Cabinet call.353 He noted that there were 3,127 confirmed cases of the Omicron variant in the UK, up by 1,239 on the previous day.354 Severity remained uncertain. However, it was:
“increasingly clear that two doses of the AstraZeneca vaccine were not as effective at stopping Omicron transmission as they had been for Delta“.355 |
| 8.128. | Mr Johnson announced a UK-wide mission, ‘Get Boosted Now’, with every adult in England to be offered the vaccine by the end of December 2021.356 The UK government would assist the devolved administrations in achieving the same acceleration. Mr Johnson considered that this approach “would not involve further restrictions and only minimal impact on the economy“.357 He explicitly recognised that “taking this additional step might not be enough to deal with the variant“, but considered “it was plainly right to pursue it“.358 Communications to the public “needed to emphasise that the risk of Omicron causing significant pressure on the NHS and deaths was serious“.359 Professor Vallance warned that the government needed to be “extremely wary” – the Omicron wave was going to come quickly.360 |
| 8.129. | The measures were to be reviewed in January 2022, by which point more data would be available.361 |
| 8.130. | By 14 December 2021, the UK had experienced the first confirmed death of an Omicron-positive patient. At a UK Cabinet meeting chaired by Mr Johnson, Mr Javid reiterated the scientific advice that “even with a low hospitalisation rate, the overall number of cases meant that the number of hospitalisations would be very high“.362 Professor Whitty warned of public debate being based on misunderstandings about the speed of spread and lack of severity. There was “no doubt that there would be a rapid rise in hospitalisations“.363 Plan B “would slow [it] down, but only to some degree“.364 He warned that, in the January 2021 peak of the second wave, NHS England:
“had coped but had been under severe pressure, and the decline in treatment of other conditions had led to excess mortality from other causes“.365 There would also be a sharp rise in sickness, self-isolation and caring for others.366 |
| 8.131. | It was noted in discussions that a package similar to Plan B had been in place in Scotland since October 2021 and had made no difference to the spread of the Omicron variant. Plan B was described as having “very minor restrictions, designed to keep the economy open“.367 It was noted that “[b]oosters and Plan B might be sufficient to prevent the NHS being overwhelmed, but only with luck“.368 The issue of consistency of messaging with the advice to continue with Christmas parties was raised.369 Professor Vallance advised:
“The most important response was to reduce the number of social contacts and make sure people self-isolated if they tested positive. It was certain that cases would go up: the situation was not looking good.“370 At the Cabinet meeting, Mr Johnson concluded: “The right response was to move to the Plan B package and roll out boosters rapidly. This would hopefully avoid the worst but it would be bumpy.“371 |
| 8.132. | An additional complicating factor was that Mr Johnson was facing significant internal political pressure not to impose further restrictions. On 14 December 2021, a number of Conservative MPs voted against Plan B measures – 98 voted against mandatory Covid-19 passes, 63 voted against mandatory vaccination for front-line NHS staff and 38 voted against compulsory face coverings in most indoor spaces.372 Reporting of ‘partygate’ resulted in some asserting that increased restrictions were intended to distract from the criticisms.373 That same day, the UK government announced additional Covid-19 funding for the devolved nations.374 |
| 8.133. | The following day at COBR, Mr Drakeford, Ms Sturgeon and Ms O’Neill raised concerns about funding arrangements. Simon Clarke MP, Chief Secretary to the Treasury from September 2021 to September 2022, confirmed that devolved administration “funding would be reviewed before Christmas and on a regular basis thereafter“.375 The following day, Mr Drakeford asked Mr Johnson to either reintroduce furlough for the UK or provide the devolved administrations with:
“access to the necessary Treasury funding so that we can ourselves consider the introduction of measures where these are necessary“.376 |
| 8.134. | On 15 December 2021, the highest daily number of Covid-19 cases (78,610) was recorded since the start of the pandemic. However, positively, around 24.6 million booster vaccines had been administered across the UK. In Scotland, there had been a “steep rise in COVID-19 cases“.377 Wales was beginning to see a rise and Northern Ireland a “slight rise“.378 |
| 8.135. | That same day, at a 10 Downing Street press conference, Professor Whitty warned that the Omicron variant posed “a really serious threat” and was “moving at an absolutely phenomenal pace“.379 When asked about the potential for overwhelming hospital capacity, Professor Whitty warned that there would be “substantial numbers” going into hospital and intensive care, which was likely to become apparent after Christmas.380 He added that records would “be broken a lot“.381 Professor Whitty also advised members of the public to modify their behaviours and social mixing in the run-up to Christmas in order to protect and “prioritise what matters“.382 This did result in some behavioural change – for example, journeys on London Underground services on 16 December 2021 stood at only 31% of the previous week.383 |
| 8.136. | On 16 December 2021, Mr Drakeford confirmed that Alert Level 4 measures might be necessary in Wales from 27 December.384 The Technical Advisory Group advised that measures below this were “not likely to have significant enough effect on the peak of Omicron cases to prevent material harm to case services“.385 Waiting for further evidence on severity was “likely to involve going beyond the point where strong preventions would have a material impact on the immediate peak“.386 By 14 December, more than 1.1 million doses of the booster vaccine had been administered in Wales.387 The advice reminded decision-makers to balance direct and indirect harms and advised that it would be “probably impossible” for the Welsh Government to provide comprehensive financial support without “large scale additional funding from the UK Government“.388 It further advised that, if Alert Level 4 measures could not be introduced, then Alert Level 2 measures could reduce the size of the peak.389 |
| 8.137. | In Northern Ireland, on 16 December 2021, the Executive Committee discussed the greater transmissibility of the Omicron variant – without further intervention, cases could rise to over 10,000 per day by the New Year. Professor McBride advised of the importance of introducing additional measures immediately after Christmas and noted that the health service was likely to come under severe pressure.390 |
| 8.138. | That day, Ms Sturgeon wrote to Mr Johnson warning that further restrictions on “higher risk” sectors may now be unavoidable and that urgent financial help was needed to protect businesses from “economic shock“.391 The Scottish Government also issued new guidelines for hospitality and retail businesses, advising the return of social distancing and one-way systems for shops and supermarkets.392 Omicron had replaced Delta as the dominant variant in Scotland.393 |
| 8.139. | On the same day, Dr Atherton informed the Welsh Cabinet that there were “reports of reduced severity in symptoms but the large number of people expected to be infected would lead to substantial pressure on the NHS“.394 The Cabinet agreed to a move to restrictions “at least at Alert level 2” after Christmas.395 Restrictions would include the reintroduction of two-metre social distancing. Regulations would be imminently changed to require people to work from home wherever possible.396 Mr Drakeford reported that the Welsh Cabinet had to consider what actions to take in the context that Mr Clarke had “refused to provide financial support to the Devolved Governments, should they need to re-introduce restrictions independently“.397 However, the Welsh Government had “up to £200m available until the end of the financial year” to provide support for businesses.398 On 17 December 2021, it announced financial support of up to £60 million to support businesses affected by the new restrictions.399 By 20 December 2021, the UK government had provided an additional £270 million of funding for Wales.400 |
| 8.140. | On 16 December 2021, SAGE noted that the number of Omicron variant infections had continued to increase rapidly, with the doubling time at around two days.401 It was “almost certain” that there were hundreds of thousands of new daily Omicron variant infections.402 There was a data lag in hospitalisations, but SAGE expected hospital admissions to reach 1,000 to 2,000 per day by the end of the year.403 Scenarios from SPI-M-O suggested that measures equivalent to those in place after Step 1 or 2 of the COVID-19 Response – Spring 2021 roadmap could substantially reduce infections and hospitalisations if enacted before the end of the year.404 |
| 8.141. | The following day, Mr Javid informed Mr Johnson by letter that he considered that the UK government should implement measures beyond Plan B and move quickly to implement measures that were in place at Step 2.405 |
| 8.142. | Covid-O also met on 17 December 2021.406 The Covid-19 Taskforce advised that there had been “rapid growth” in cases that week. The previous day, 88,000 cases had been reported. This was a “record figure and far exceeded the peak of the [second wave] when 68,000 positive cases were reported in one day“.407 Far higher positive test numbers were expected, with the true number of infections potentially being 300,000 – the Omicron variant was estimated to account for the majority of cases in England. There was a significant impact on the working-age population.408 Professor Whitty advised that the booster vaccination programme was “key“, but it had started at the top end of the age cohorts and was just starting to focus on those of working age.409 Mr Javid stated:
“[M]illions of infections from the Omicron variant were expected, and the current doubling rate would mean that the ‘pingdemic’ seen earlier in the year would seem like a walk in the park.“410 |
| 8.143. | Mr Johnson concluded that the “booster programme and the implementation of Plan B measures were the right way forward to contain” the Omicron variant.411 From 17 December 2021, there were to be daily Covid-O meetings to consider contingency plans.412 |
| 8.144. | At a meeting of the Scottish Gold Command on 19 December 2021, it was agreed that a paper would be prepared for the Scottish Cabinet to set out the full costs and requirements for a four-week circuit breaker lockdown.413 |
| 8.145. | On 19 December 2021, at COBR, it was recorded that Scotland was monitoring the situation, considering it to be behind the wave in London. Wales was still experiencing high, but stable, community transmission of Delta variant cases, and Omicron variant cases were rising, but from a low baseline.414 Mr Johnson was not in attendance.415 |
| 8.146. | At this time, tensions in England over the way forward were becoming more acute. Mr Johnson was facing calls from Mr Javid to go further and to introduce a package of measures akin to the previous Step 2 of the COVID-19 Response – Spring 2021 roadmap (such as no indoor household mixing and the rule of six outdoors).416 Mr Sunak and Mr Johnson had a number of discussions between 16 and 19 December 2021. Mr Johnson recalled that Mr Sunak was “very concerned about restrictions and the impact that they would have on the economy“.417 He did not recall receiving any analysis, modelling or forecasting concerning the economic impact.418 Mr Johnson was described as being “genuinely undecided” after a meeting with Mr Sunak on 18 December.419 Mr Sunak made it clear in a meeting on 19 December that he “remained sceptical of the case for further restrictions“.420 In his evening notes, Professor Vallance recorded that Mr Sunak said he would “err on the side of waiting” as the evidence wasn’t “compelling enough” and that in his view the model showed “herd immunity” being the way through.421 |
| 8.147. | SAGE met on 20 December 2021. Infections and hospitalisations in South Africa appeared to be declining. The reasons for this were unclear and it could not be assumed that it would be sustained or that the wave in the UK would follow a similar pattern – given differing populations and epidemiological situations. SAGE noted the uncertainties, but “[p]olicy decisions (either to do nothing or something) need to be made sooner than these uncertainties can be resolved“.422 The warnings were stark. SAGE reiterated its previous advice about early intervention and further advised that measures targeted at more at-risk groups only (eg shielding) were not an effective substitute for population-wide measures.423 |
| 8.148. | Mr Johnson chaired the UK Cabinet that day.424 The number of infections had hit the highest levels during the pandemic, with 93,000 on 16 December compared with a peak of 68,000 the previous winter. Footfall in city centres in England was 57% of pre-Covid-19 levels since Plan B. London Underground data indicated that, on 17 December, journeys were at 45% of pre-Covid-19 demand.425 A number of European countries had implemented stricter restrictions. Denmark had locked down.426 At Cabinet, Mr Johnson’s view was to continue with Plan B. Mr Javid said:
“[T]he decision to not go further than Plan B was a significant one. It would mean that hospitalisations would increase with an uncertain peak.“427 |
| 8.149. | The discussion in the UK Cabinet focused on:
|
| 8.150. | Professor Whitty provided unambiguous advice, explaining that he wanted to provide:
“his clear professional view on the discussion. It should not be assumed that everything would follow the optimistic path. The balance of debate in Cabinet on the data was a long way from international consensus. There was going to be a wave of hospitalisations based on current infection rates. The question was going to be how big the wave was.“428 He advised that it was difficult to make comparisons with South Africa, where it was summer, compared with the UK’s winter, and where the demographic was different. The relative effectiveness of vaccination and the booster would be known within a week or two. Shielding of clinically vulnerable people would not make a significant impact on hospitalisation but there was evidence of negative mental health impacts.429 Professor Vallance also reiterated the SAGE advice – the longer it took to make decisions to introduce further measures, the higher the number of hospitalisations given current doubling rates. Modelling had included positive assumptions about severity, vaccine effectiveness and the booster uptake. He said that the “trajectory of Omicron infections and hospitalisations was clear“.430 |
| 8.151. | Mr Johnson, noting that the UK Cabinet discussion was the “furthest it had been during the pandemic from the current scientific position“, summed up with the decision not to introduce any further restrictions before the Christmas break:
“[W]hile the data was uncertain, it was premature to reimpose restrictions. Given the uncertainty of the data and the downsides of more stringent measures, it was right to proceed on the basis of: actively implementing Plan B, increasing capacity in the NHS (e.g. discharge); procuring antivirals; encouraging the public to exercise caution; making the proposed changes to self-isolation; and focussing on accelerating the booster campaign. There was an optimistic world where the Government may not need to act further.“431 |
| 8.152. | On 20 and 21 December 2021, to combat an expected increase in Omicron variant cases and consequent NHS pressures, the Welsh Cabinet agreed to move to Level 2 restrictions from 26 December, including reinstating two-metre social distancing, the rule of six and face coverings in hospitality settings. All indoor and outdoor events would be closed to spectators.432 |
| 8.153. | The Scottish Cabinet met on 21 December 2021 to consider whether new restrictions would be required. Ministers were told they should take account of:
“the potential impact of a high number of cases on the wider provision of essential services – even if, in health impact terms, Omicron was much less severe“.433 The Cabinet agreed to introduce additional measures from 27 December 2021, including the reintroduction of one-metre physical distancing in all hospitality and indoor leisure settings and pausing large-scale events.434 The option of a circuit breaker lockdown was confirmed as the best means to tackle the viral spread, but ministers were told they could not take it due to the lack of commitment for financial support from the UK government.435 It was described as “extremely disappointing” that neither the Prime Minister nor the Chancellor of the Exchequer had attended COBR on 19 December.436 |
| 8.154. | That same day, Mr Johnson released a short video confirming that there would be no new restrictions imposed immediately in England for the Christmas period but that they could not be ruled out after Christmas – the situation was “finely balanced“.437 |
| 8.155. | By 22 December 2021, the Omicron variant accounted for over 50% of new cases in Northern Ireland. Hospitals were operating at 103% bed capacity.438 Professors McBride and Young advised that this wave of infection would likely be “significantly larger” if current doubling rates continued, peaking in mid-January 2022 with a lag for any hospital pressures. They warned the Executive Committee that, without significant additional interventions, “it would be unwise to plan on the assumption that the wave would peak before we saw very large numbers” and observed that “earlier and stronger intervention” would be more effective in protecting hospital capacity.439 |
| 8.156. | The same day, the Northern Ireland Executive Committee agreed to impose a number of restrictions, including limits on mixing of households and in workplaces and a capacity cap for events, most of which took effect from 27 December.440 Increased statutory requirements for wearing face coverings were introduced on 27 December, with a grace period to 7 January 2022. The Executive Office explained:
“There was little information available on the impact the Omicron variant would have. The scientific advice was, therefore, to implement precautionary measures to reduce its spread until more was known.“441 |
| 8.157. | On 23 December 2021, SAGE reported that the number of Omicron variant infections was still growing quickly, albeit rates were beginning to slow.442 Multiple analyses suggested (with medium confidence) that the Omicron variant was less severe than the Delta variant, although it remained unclear to what extent.443 The anticipated peak in hospital admissions was “highly uncertain“, but even with:
“a reduction in severity may be comparable to, or higher than previous peaks in the absence of significant behaviour change or further interventions“.444 SAGE advised that delaying interventions until after the anticipated wave of infections in older people was under way would be “too late to make a significant difference to the numbers of infections, hospitalisations or deaths“.445 |
| 8.158. | By 30 December 2021, further data were available. Infection rates were “by far the highest levels seen yet in the pandemic” and admission data showed “rapidly growing pressure on the NHS” in England.446 The Omicron variant was considered to be around 50% to 70% less severe than the Delta variant in a population with high immunity and vaccine efficacy against severe disease, and hospitalisation was estimated at 90% after a booster.447 Professors Vallance and Whitty considered the updated data but advised that the issues and conclusions at the previous SAGE meeting remained appropriate.448 There was “rapidly growing pressure on the NHS” – the threat was no longer a theoretical modelled outcome but was based on admissions data.449 The encouraging severity and vaccine efficacy data were set against the increased proportion of the population infected. They advised 10 Downing Street, the Cabinet Office, the Department of Health and Social Care and the Covid-19 Taskforce that it would be unsafe to assume for planning purposes that the Omicron variant would peak early.450 They emphasised that any action would be useful in reducing the pressure on the NHS and probably in reducing deaths, and that, because the aim was no longer to reduce R to below 1 but instead to buy time for the booster vaccination programme, there would be no need for full lockdown measures akin to earlier in the pandemic.451 |
| 8.159. | A smaller ‘home team’ meeting followed on 31 December 2021, foreshadowing the forthcoming review of Plan B. It was attended by the Prime Minister and representatives from the Cabinet Office and the Treasury.452 An email sent by Professor Vallance that day recorded that there was “huge resistance to any further measures” from Mr Johnson and Mr Sunak, with them not wanting to “move on anything more“.453 Mr Javid, who had previously argued for further restrictions, was not invited.454 The briefing paper from Mr Ridley suggested that Mr Johnson consider further measures for a short period to reduce the peak. Mr Johnson told the Inquiry that he handwrote his scepticism of them: “bollocks“.455 |
The situation at the end of December 2021
| 8.160. | Professor Vallance described the advice of SAGE in December 2021 as a “deeply worrying development“.456 He said:
“It is easy with retrospect to dismiss these concerns as being overblown, primarily because we now know that the disease caused by Omicron in those with Covid-19 immunity proved to be, for most, relatively mild in a well vaccinated population.“457 That was not known at the time, nor “was there good reason to assume that this would be the case“.458 |
| 8.161. | As Professor McBride observed in any event with regard to severity:
“Even if the number of people experiencing severe disease was less, as the CSA [Chief Scientific Adviser] and I said at the time in advice to the Executive on the number that may require hospital care ‘a small percentage of a very large number is still a large number’.“459 |
| 8.162. | Mr Johnson said that he:
“now had the confidence to resist. By this stage of the pandemic, despite not being a scientist, I had looked at so much data that I felt I was getting better at understanding where it would go. I had a fascination with the South African data and felt that, given the date of vaccination and booster rollout, the rate of Omicron would spike soon and fall away.“460 Similarly, Mr Sunak and others were “sceptical of the case for further restrictions“.461 |
| 8.163. | In contrast, Sir Frank Atherton told the Inquiry that, in December 2021, he did not “know an awful lot” about the Omicron variant – he understood it was highly transmissible but that “the severity of the illness that it would cause” was unknown. He said:
“I was pessimistic but my pessimism was unjustified, and so we were lucky. But sometimes it’s better to be wise than lucky.“462 |
| 8.164. | The scientific advisers were best placed to judge the threat posed by the Omicron variant, although that does not mean that decision-makers were bound to follow their advice. There were compelling competing interests. Professor Whitty noted, however, that a “strong narrative developed among some that this was just a trivial infection and nothing to worry about“.463 Both he and Professor Vallance are correct in emphasising that this was not borne out in the data. The Omicron variant was not much less dangerous than the earlier variants. It was also not a trivial infection for many, particularly the elderly and those who developed Long Covid.464 |
| 8.165. | The UK government’s approach in this period was, once again, overly optimistic. The greatest strategic risk was a variant that evaded natural and vaccine-induced immunity. The Omicron variant was potentially exactly that. Had it been so, Plan B would have been insufficient to meet the risk. The sheer number of infections demonstrates that, if vaccines were less effective or the Omicron variant had been as severe as previous variants in terms of morbidity and mortality, the numbers of deaths would have likely exceeded the earlier waves in the absence of another lockdown. |
| 8.166. | The measures taken by the Scottish Government on a precautionary basis in December 2021 were a reasonable step, in light of the emerging threat.465 Mass self-testing was delivered by making free lateral flow tests available to the whole population of Scotland from late 2021, which allowed people to manage their own risk effectively by changing their behaviour when testing positive.466 |
| 8.167. | The Welsh Government also reintroduced restrictions, culminating in a move to Alert Level 2 from 26 December 2021. When case rates and, consequently, death rates began to rise throughout the autumn, it communicated its plans to the public, setting reasonable expectations that restrictions might need quickly to be reimposed if a highly transmissible new variant was identified or vaccine immunity began to wane. The Welsh Government had learned lessons from the failed responses of 2020. The booster vaccine was proving effective at protecting against severe disease for the most vulnerable. However, in light of gaps in data concerning the more general efficacy of vaccines and increasing pressures on the NHS, the introduction of some restrictions was sensible given the possible risks posed by this new variant and the Welsh Government’s stated objective of not overwhelming the NHS. While the response during this period was assisted by the uptake of the vaccine and by the Omicron variant being less severe than may otherwise have been the case, the Welsh Government had clearly articulated objectives in 2021 – that restrictions must be linked to keeping cases at a manageable level without overwhelming the NHS – and it took the public with it during this period through regularly communicating its plans and potential responses. Its decisions remained linked to its objectives. |
| 8.168. | The decision of the Northern Ireland Executive to introduce precautionary measures at the end of December 2021 was a reasonable and appropriate course in the circumstances. Throughout November and December 2021, the rate of new Covid-19 cases in Northern Ireland had increased and health service pressures were ongoing. The clear advice of the Chief Medical Officer and Chief Scientific Adviser at that time was that additional measures were required immediately after Christmas in order to avoid the health service coming under severe pressure. The Executive Committee acted decisively and proactively upon receipt of the medical and scientific advice in December 2021. The decisions taken by the Executive Committee at this juncture demonstrate that the Northern Ireland Executive had, to some extent, learned important and necessary lessons from its management of the earlier waves. |
| 8.169. | The Inquiry is not persuaded by the suggestion that the Welsh and Scottish governments’ ability to make decisions had to be viewed in the context of the UK government refusing to make additional funding available. The minutes of the COBR meeting on 15 December 2021 record that there would be a review of “DA [devolved administration] funding” before Christmas.467 The Treasury would necessarily require time to do this. Additional funding was confirmed just days later on 20 December. In any event, both the Welsh and Scottish governments had access to their own funds if further measures were deemed appropriate. |
January to May 2022
Figure 36: Estimated percentage of the population testing positive for Covid-19 from 1 December 2021 to 1 June 2022 across the UK
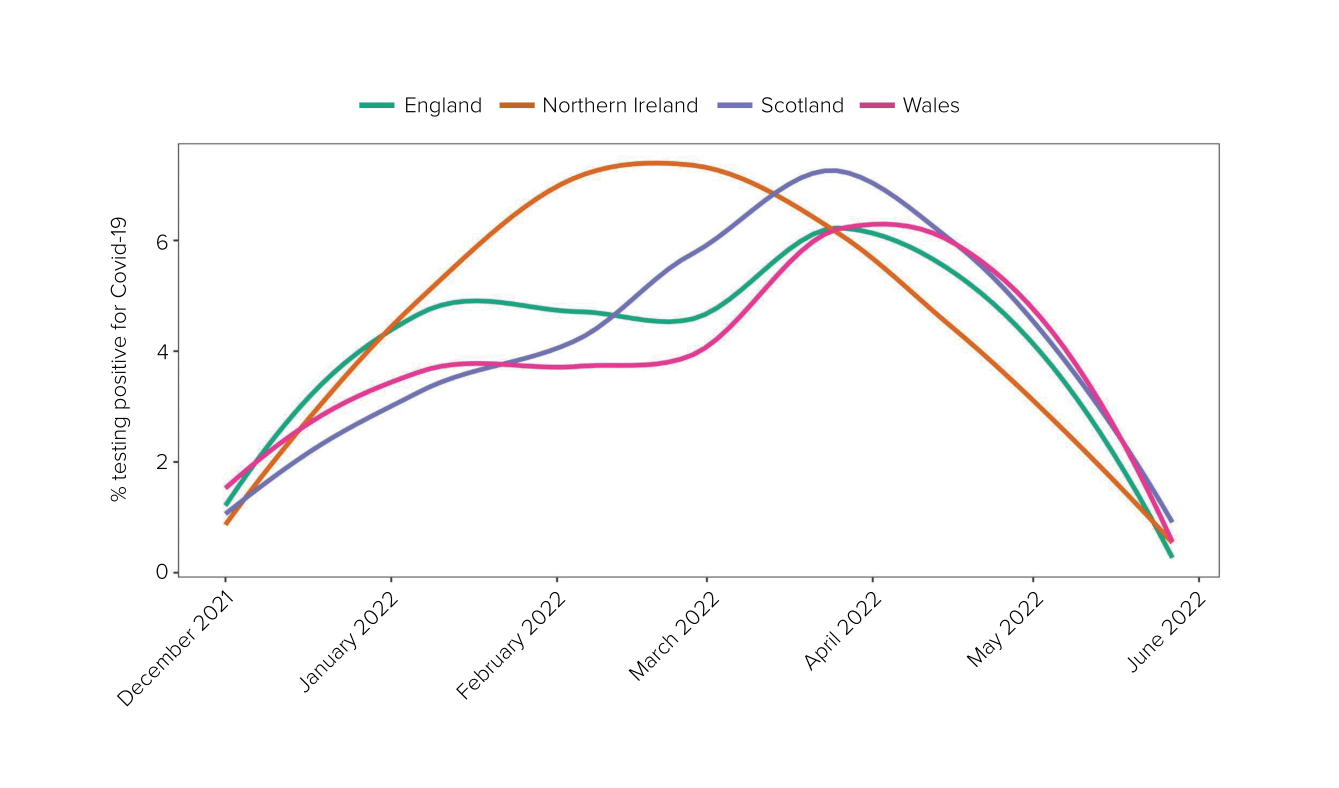
Source: Coronavirus Infection Survey from 1 December 2021 to 1 June 2022 (Modelled estimates, 95% confidence intervals not shown). For raw data, see the Coronavirus (COVID-19) Infection Survey: England, dataset, Office for National Statistics, 10 March 2023 (https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/datasets/coronaviruscovid19infectionsurveydata/2023)
Figure 37: Daily deaths per 100,000 population by date of death from 1 December 2021 to 1 June 2022 across the UK
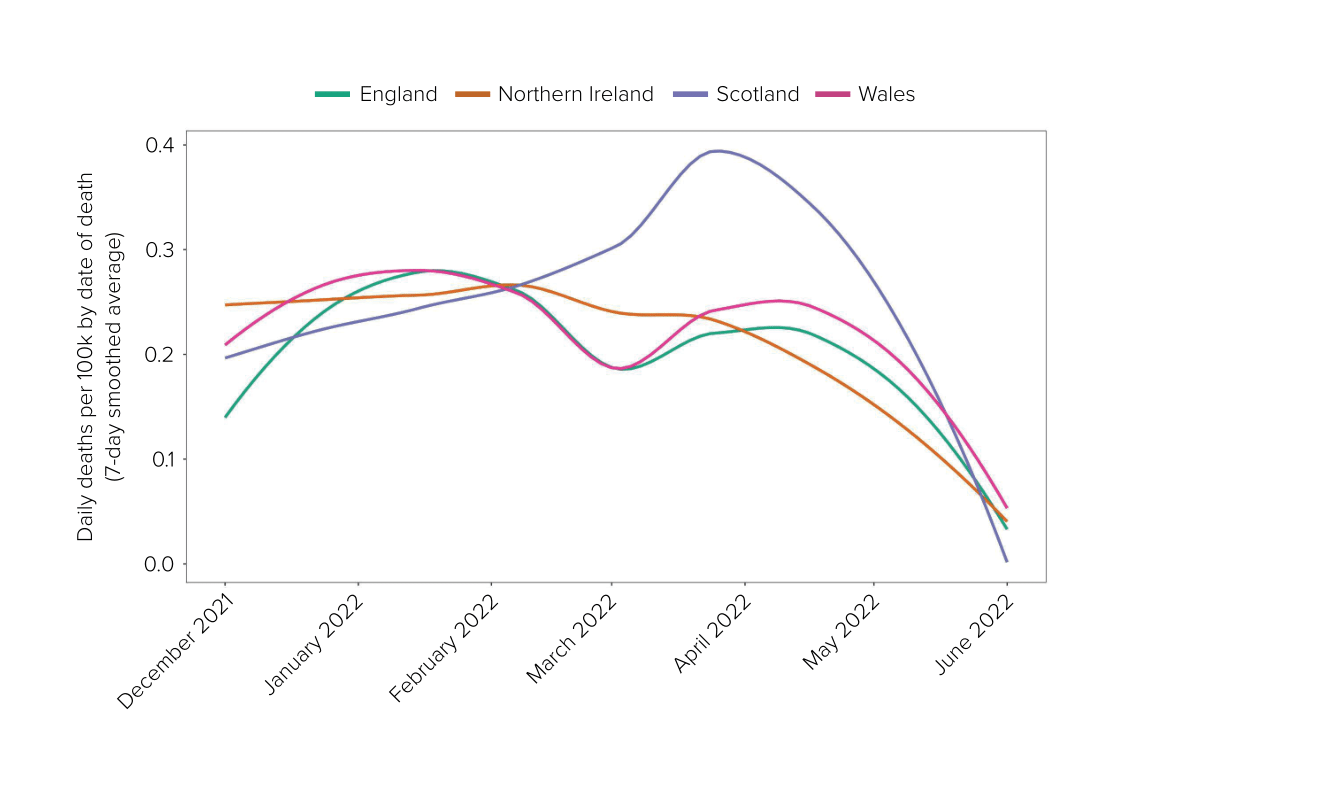
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 8.170. | On 5 January 2022, Mr Yousaf said that the Scottish Government’s task was to “somehow ensure our NHS doesn’t completely collapse“, but he was not sure that could be delivered because “we’ve lost the dressing room on this one“.468 As noted by Professor Linda Bauld (Chief Social Policy Adviser to the Scottish Government from September 2021 to April 2022), societal and economic harms were “very much coming to the fore“.469 |
| 8.171. | Also on 5 January 2022, Covid-O agreed to remove testing requirements for fully vaccinated travellers.470 At a UK Cabinet meeting, Mr Johnson explained that the Omicron variant was less severe and that:
“[T]he single best option for the country was to get through this period without going back to restrictions that had a large negative impact on the way of life of millions.“471 England would continue with Plan B for another three weeks.472 |
| 8.172. | By 7 January 2022, the number of infections had continued to increase but had levelled in London. SAGE considered the most pessimistic scenarios were unlikely.473 It advised that non-pharmaceutical interventions implemented at this stage would have little effect on the peak but could affect hospitalisation levels, although this would be at a far lower level than if implemented earlier.474 |
| 8.173. | On 10 January 2022, Sir Frank Atherton advised the Welsh Cabinet that there was still “significant community transmission” and that “it was too early to tell whether the trajectory of cases had reversed“.475 Dr Orford advised that “hospital admissions were tracking close to the scenario planning but symptoms were less severe for those who had been vaccinated“.476 By 13 January, Welsh case numbers and hospital admissions due to Covid-19 were falling.477 The Cabinet was advised that the peak of Omicron variant cases either had or would soon be reached. It agreed that there would be a return to Alert Level 0 measures from 28 January.478 |
| 8.174. | On 17 January 2022, restrictions in Scotland were relaxed to allow large outdoor events.479 Restrictions would be further relaxed from 24 January, with large indoor events resuming and social distancing rules being removed.480 |
| 8.175. | In Northern Ireland, the Executive Committee met on 20 January 2022. Professor Young advised that hospital pressures were following the optimistic modelling scenario.481 In light of this, the Executive Committee agreed to relax a number of restrictions to take effect on 21 and 26 January.482 |
| 8.176. | On 27 January 2022, the UK government reverted to Plan A of COVID-19 Response: Autumn and Winter Plan 2021.483 The number of hospitalisations was declining.484 On the advice of Professors Whitty and Vallance, messaging was to remain cautious.485 The following day, restrictions on physical distancing and face masks were further reduced in Scotland.486 |
| 8.177. | Most significantly, for reasons unrelated to the pandemic, Paul Givan MLA, First Minister of Northern Ireland from June 2021, resigned on 3 February 2022. As a result, Ms O’Neill also ceased to hold office and power-sharing collapsed. Jayne Brady, Head of the Northern Ireland Civil Service from September 2021, explained:
“In the absence of a First Minister and deputy First Minister as joint Chairs there was no functioning Executive during the period during which the other Ministers remained in office. Ministers could therefore only perform limited roles, within the specific responsibilities of their departments. No cross-cutting, significant or controversial decisions, which must be referred to the Executive under the terms of paragraph 2.4 of the Ministerial Code, could be taken in the absence of the Executive. In The Executive Office, without a First Minister and deputy First Minister in place, any departmental decision-making requiring Ministers was not possible.“487 There was, therefore, no functioning Executive Committee in Northern Ireland from this point onwards. Power-sharing was not restored until 3 February 2024. |
| 8.178. | On 14 February 2022, Mr Swann wrote to his remaining Executive Committee colleagues regarding the management of health protection regulations in the absence of an Executive Committee.488 In an urgent written statement to the Northern Ireland Assembly the same day, Mr Swann confirmed that all remaining Covid-19 restrictions set out in regulations would be replaced by guidance on 15 February.489 |
| 8.179. | In Wales, on 7 February 2022, “there was cautious optimism that the situation was improving and a gradual easement of protections was recommended“.490 Ministers agreed to retain self-isolation requirements, but the requirement to wear a face covering would be retained for retail, transport and public health settings only.491 |
| 8.180. | On 21 February 2022, the UK government announced COVID-19 Response: Living with COVID-19 for the continued management of the response.492 Its stated objective was “to enable the country to manage COVID-19 like other respiratory illnesses“.493 The strategy focused on the use of vaccines and support of the NHS and social care sector. There was a lack of specific plans in the event of a future variant of concern. |
| 8.181. | This followed conflict within the UK government over the strategy to be adopted moving forward and, in particular, with regard to the dismantling of infrastructure and apparatus.494 In January 2022, Professor Vallance recorded in his evening notes that the Treasury was “totally against continued spend” on vaccines.495 These issues came to a head on the morning of the announcement of the strategy. Mr Javid raised concerns with Mr Johnson about the dismantling of infrastructure around testing and lack of continued funding for scientific research.496 Concerns had also been expressed by Professors Whitty and Vallance in respect of the emphasis on the actions to date to the detriment of future plans and an approach that was “too far on the ‘it’s all over’ side of things“.497 It was considered to be “very light on what to do if there is a more severe variant“.498 |
| 8.182. | All remaining restrictions were lifted in England from 24 February 2022. This was accompanied by the withdrawal of free universal testing, as well as the ending of contact tracing, legal requirements to self-isolate and various forms of government funding. In his announcement to the public, Mr Johnson said:
“We have emerged from the teeth of the pandemic before many others … now we have the chance to complete that transition back towards normality, while maintaining the contingencies to respond to a resurgence or a new variant.“499 |
| 8.183. | On 22 February 2022, Ms Sturgeon announced that all legal requirements relating to Covid-19 would be removed in Scotland from 21 March.500 The Scottish Government’s updated strategic framework was published on 22 February.501 Its strategic intent was to:
“manage Covid-19 effectively, primarily through adaptations and health measures that strengthen our resilience and recovery, as we rebuild for a better future“.502 |
| 8.184. | On 4 March 2022, the Welsh Government published Together for a Safer Future: Wales’ Long-Term COVID-19 Transition from Pandemic to Endemic.503 It outlined how Wales would “begin to move beyond the initial emergency phase … to plan a future in which we live with coronavirus, just as we live with many other infectious diseases“.504 It said Covid Stable (additional waves that would not “put unsustainable pressure on the Health and Social Care System“) was “the most likely scenario“.505 |
| 8.185. | On 1 March 2022, R was estimated to be between 1.0 and 1.3 in Scotland.506 On 8 March, the Scottish Cabinet noted that there was a “deteriorating situation“, which was putting additional pressure on the NHS.507 On 9 March, Covid-19 hospitalisation figures in Scotland were at their highest for 13 months, with 1,636 people recorded.508 By 16 March, Covid-19 hospital occupancy had increased by 32% compared with the previous week and was reaching levels close to the previous peak in January 2021.509 A sub-variant of Omicron, BA.2, was believed to be behind a surge in Covid-19 cases.510 Against this backdrop, on 15 March the Scottish Government announced that the legal requirement to wear face coverings on public transport and in most indoor public settings would continue until at least early April, but all other requirements for businesses and service providers were to change from mandatory to advisory from 21 March.511 The requirement to wear face coverings was subsequently extended until 18 April.512 |
| 8.186. | Due to rising case numbers in Wales, on 24 March 2022, the Welsh Cabinet agreed that some restrictions on businesses would remain in place and that face coverings would continue to be required in health and social care settings.513 By 12 April, Covid-19 hospital admissions in Wales had plateaued and “[t]hose in intensive care with the virus had remained lower than in previous waves“.514 Restrictions on businesses would be removed but the legal requirement for face coverings in health and social care settings would remain.515 |
| 8.187. | Hospital pressures due to Covid-19 in Scotland remained considerable in April 2022 and had been higher than the UK average since February 2022.516 On 28 April, the Scottish Government announced that public health advice would change to a ‘stay at home’ message (replacing self-isolation) from 1 May. Testing for the general population and contact tracing would end on 30 April and NHS Scotland would be taken out of its emergency footing at the end of the day on 30 April.517 |
| 8.188. | By 23 May 2022, infection rates in Wales continued to wane and the vaccine was limiting the number of people experiencing serious direct harm. The Welsh Cabinet followed Sir Frank Atherton’s advice and agreed to allow the requirement to wear a face covering in health and social care settings to expire on 30 May. All restrictions in the UK came to an end on 30 May 2022.518 |
The situation at the end of May 2022
Figure 38: Cumulative daily deaths per 100,000 by date of death from May 2021 to May 2022 across the UK
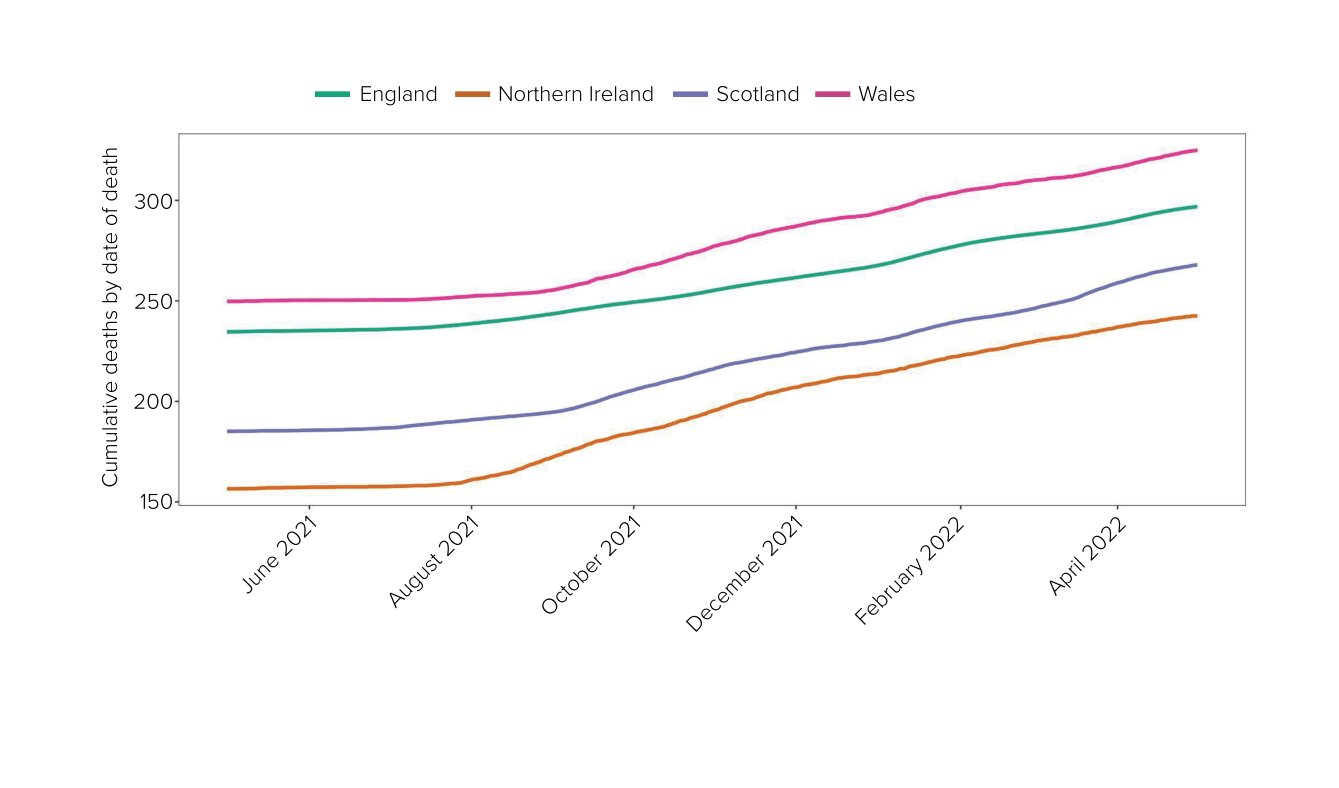
Source: UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download)
| 8.189. | The UK government’s COVID-19 Response: Living with COVID-19 document suffered from many of the flaws identified in strategies developed at earlier stages of the pandemic. The strategy, which was reliant on vaccines, was unlikely to be sufficient in the event of a variant emerging with increased transmissibility or severity or in an evolved state, such that the population did not enjoy either natural or vaccine-induced immunity. Clear plans should have been in place for implementing measures in such scenarios. |
| 8.190. | Scotland experienced a comparably higher level of hospitalisation of Covid-19 patients between May 2021 and May 2022 than the UK as a whole.519 One reason for the higher number of hospitalisations might have been Scotland’s “older and sicker” population, with higher levels of underlying health conditions, which placed people at greater risk.520 This was especially evident in areas that were economically disadvantaged.521 Although hospitalisations in Scotland were comparatively higher than the rest of the UK during this period, the number of deaths in Scotland remained lower than earlier in the pandemic. All governments were faced with difficult choices between balancing the direct harms from the virus and other harms. These choices became more difficult later in the pandemic because there had been prolonged social and economic harm caused by the restrictions. The easing of restrictions by the Scottish Government in this period was a recognition that the balance of harms had shifted from earlier in the pandemic. |
| 8.191. | The Welsh Government was sensible in maintaining some restrictions throughout the first few months of 2022 while it awaited further advice about the severity of the Omicron variant and the impact of the vaccines on direct harm.522 This mirrored the Welsh Government’s approach throughout the period from May 2021 to May 2022 – decisions were informed by scientific advice as the Welsh Government sought to balance the competing harms of the virus. |
| 8.192. | The position in Northern Ireland merits separate consideration. The narrative of the Covid-19 pandemic in Northern Ireland is book-ended by the absence of an Executive. The Northern Ireland Executive re-formed on 11 January 2020 before, once again, collapsing on 3 February 2022. The power-sharing arrangements in Northern Ireland broadly require any decisions that are significant, controversial or cross-cutting to be referred to the Executive. Consequently, the absence of an Executive meant that such decisions simply could not be taken. It is plain from examining the Northern Ireland Executive’s decision-making throughout this period that many, if not most or all, of the decisions relating to the pandemic response in Northern Ireland were of the sort that required referral to the Executive Committee. It was, therefore, fortunate that the power-sharing institutions in Northern Ireland had been restored just prior to the pandemic. Following Mr Givan’s resignation, in the absence of a functioning Executive Committee, Mr Swann had no alternative but to replace all existing Covid-19 restrictions set out in regulations with guidance. In the context of an ongoing pandemic, this is clearly unacceptable. If a further wave of Covid-19 infection had occurred in Northern Ireland after 3 February 2022, it is difficult to envisage how it could have been managed within Northern Ireland in the absence of a functioning Executive. The Northern Ireland Executive should urgently consider how decisions that would usually be subject to ministerial approval would be taken should an emergency occur during the suspension of power-sharing arrangements. |
A new normal
| 8.193. | Much of the period between May 2021 and May 2022 was characterised by the race to ensure the widest vaccine coverage possible and the need to protect the population against the emergence of potentially more transmissible and more deadly variants. As vaccine coverage increased, there was an increasing preparedness within the governments to tolerate a higher level of infection and death, so as to avoid adding further to the significant economic and societal harms that had occurred through the imposition of stringent restrictions. However, there was no active decision or agreement as to what that level was or ought to be. |
| 8.194. | The approach of the UK government and devolved administrations in the autumn of 2021 carried some risk. An immune escape variant had been repeatedly identified as the biggest strategic risk. It was fortunate that the Omicron variant, which emerged in mid-December 2021, came after the vaccine rollout was well progressed. The sheer number of infections demonstrates that, in the event that vaccines had been less effective or the Omicron variant had been as severe as previous variants in terms of morbidity and mortality, the consequences would have been disastrous. |
| 8.195. | The UK government, the Scottish Government and the Northern Ireland Executive had no detailed contingency plan for a variant with greater vaccine-escape properties, save for, where considered, a return to previous restrictions. The Welsh Government’s Coronavirus Control Plan: Autumn and Winter 2021 Update did provide for an “alert levels framework” – one of which, Level 4, amounted to a lockdown.523 However, this plan would have been of greater utility had it provided clearer defined thresholds for possible further action. |
| 8.196. | The UK government’s Plan B, the more pessimistic of the two contingency plans, provided for only modest interventions, which were unlikely to be able to deal adequately with the advent of a more transmissible or lethal variant, evading natural or vaccine-induced immunity. As it was, the UK government delayed the implementation of Plan B until 8 December 2021. Even when it was clear in mid-December that the Omicron variant posed a really serious threat, the UK government declined to implement more stringent measures beyond those in its Plan B, or to return to the measures provided for by Step 2 of the COVID-19 Response – Spring 2021 roadmap. Ultimately, the UK government was spared worse by the fact that the Omicron variant turned out to be around 50% to 70% less severe than the Delta variant in a population with high immunity. |
| 8.197. | The measures taken by the Scottish Government with effect from 27 December 2021, in particular the pausing of large-scale events and the reintroduction of one-metre physical distancing and table service in indoor hospitality (alongside, as with the other governments, the continued acceleration of the vaccine booster programme and the making available of free lateral flow tests), were better calibrated. The Welsh Government and the Northern Ireland Executive Committee also acted decisively and proactively to introduce Level 2 restrictions and limits on the mixing of households and workplaces and a capacity cap for events from 26 and 27 December respectively. |
| 8.198. | Remaining restrictions were lifted in England, Scotland and Wales at different times during the course of the first half of 2022, depending on the case numbers then prevailing and the number of deaths. In Northern Ireland, the collapse of the power-sharing agreement on 3 February 2022 meant that all the existing Covid-19 regulations were withdrawn and replaced by guidance. All restrictions in the UK came to an end on 30 May 2022. |
- In Scotland, the population infection rate remained at over 2% in May 2022, the rates in the other three nations having been about 1.75% at that time (INQ000274150_0010).
- COVID-19 Response – Spring 2021, HM Government, February 2021 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087)
- ‘Moving to Level 3’, Scottish Government, 20 April 2021 (https://www.gov.scot/news/moving-to-level-3; INQ000369717)
- ‘Further coronavirus restriction relaxations brought forward’, Welsh Government, 22 April 2021 (https://www.gov.wales/further-coronavirus-restriction-relaxations-brought-forward; INQ000055026)
- INQ000212958; INQ000207213; INQ000212959; INQ000048525; INQ000212962
- INQ000369765_0061-0062 para 362
- INQ000251645_0150 para 8.82
- SARS-CoV-2 Variants of Concern and Variants Under Investigation in England: Technical Briefing 10, Public Health England, 7 May 2021, p24 (https://assets.publishing.service.gov.uk/media/60953a8dd3bf7f288b4235ec/Variants_of_Concern_VOC_Technical_Briefing_10_England.pdf; INQ000222014)
- Technical Report on the Covid-19 Pandemic in the UK, Department of Health and Social Care, 1 December 2022, p33 (https://www.gov.uk/government/publications/technical-report-on-the-covid-19-pandemic-in-the-uk; INQ000101642)
- INQ000283367_0005
- INQ000283367_0006
- INQ000119964_0001 para 1
- INQ000119964_0001 para 1
- INQ000119964_0001 para 3
- INQ000119964_0001 para 4
- INQ000119964_0001 para 5
- INQ000119963
- INQ000088894_0005
- INQ000088894_0004
- ‘COVID-19 alert level: Update from the UK Chief Medical Officers’, Department of Health and Social Care, 10 May 2021 (https://www.gov.uk/government/news/covid-19-alert-level-update-from-the-uk-chief-medical-officers-10-may-2021; INQ000086792)
- INQ000351841
- INQ000351841
- INQ000120618_0001 para 9
- INQ000120618_0002 para 14
- INQ000057741_0006 para 3.4
- Under the ‘rule of six’, a maximum of six people could meet indoors; (see INQ000057741_0004 para 2.15).
- INQ000120618_0001 para 1
- INQ000354508_0003 para 13
- INQ000354508_0005 para 24
- ‘Most vulnerable offered second dose of COVID-19 vaccine earlier to help protect against variants’, Department of Health and Social Care, 14 May 2021 (https://www.gov.uk/government/news/most-vulnerable-offered-second-dose-of-covid-19-vaccine-earlier-to-help-protect-against-variants; INQ000548026)
- INQ000212967
- INQ000207216_0004 para 13
- INQ000207216_0004-0005 paras 15-16; see also INQ000207216_0013
- INQ000233185_0002. The Scottish Government established the Four Harms Group in late October 2020, involving members from outside the Scottish Government as well as the Chief Medical Officer and other civil servants (INQ000375323_0013 para 38).
- ‘Next steps out of lockdown’, Scottish Government, 11 May 2021 (https://www.gov.scot/news/next-steps-out-of-lockdown; INQ000548029); ‘Coronavirus (COVID-19) update: First Minister’s statement – 11 May 2021’, Scottish Government, 11 May 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-11-2021; INQ000354327)
- INQ000089033_0010. This confirmed that the Delta variant was prevalent in areas such as Bolton and Blackburn.
- INQ000089033_0011
- INQ000089033_0011
- INQ000065750_0002
- INQ000375416
- INQ000048525_0005; INQ000207217_0004
- INQ000212972_0002 para 7
- INQ000212972_0001-0002 para 5
- INQ000212972_0002 para 6
- INQ000214466_0005 para 26
- INQ000233258. This was reflected in ‘Beyond Level 0’, a paper commissioned by Ms Sturgeon on 10 May 2021; see also ‘Beyond Level 0 guidance’, Scottish Hockey (https://scottish-hockey.org.uk/covid-19/coronavirus-covid-19-protection-levels/beyond-level-0-guidance; INQ000651559).
- INQ000233258_0005
- INQ000334792_0006
- INQ000120619_0001 para 1
- INQ000120619 paras 7, 9
- The Office for National Statistics’ Coronavirus (Covid-19) Infection Survey estimated that 48,500 people had Covid-19 in the community for the week 16 to 22 May 2021, as compared to 90,000 people for the week from 10 to 16 April (see INQ000119963_0002 para 9; INQ000120619_0001 para 2).
- SPI-M-O Medium-Term Projections, SPI-M-O, 26 May 2021 (https://assets.publishing.service.gov.uk/media/60c0aa1be90e0743a7a709db/S1252_SPI-M-O_MediumTermProjections.pdf; INQ000548033)
- Coronavirus Control Plan: Revised Alert Levels in Wales (March 2021), Welsh Government, March 2021 (https://www.gov.wales/sites/default/files/publications/2021-05/coronavirus-control-plan-revised-alert-levels-in-wales-march-2021.pdf; INQ000066069); INQ000022537_0003 paras 1.9-1.10
- INQ000382157
- INQ000207218_0003
- The Common Travel Area is an arrangement between the UK, the Crown Dependencies and Ireland under which British and Irish citizens can move freely and reside in either jurisdiction and enjoy associated rights and privileges.
- INQ000207218_0009
- INQ000207218_0009
- INQ000214573_0004 para 16
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 4 June 2021’, Scottish Government, 4 June 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-4-june-2021; INQ000353712_0004-0005)
- INQ000120623_0001 para 1; INQ000120618_0001 para 1
- INQ000120623_0001 para 7
- INQ000251645_0206 para 12.1
- Lee Cain 31 October 2023 81/19-82/22
- Rachael Evans 13 October 2023 116/4-9
- INQ000120513; see also INQ000061556_0003 para 17
- INQ000280197_0002 paras 4-5; INQ000280196_0002 para 3
- INQ000251645_0208-0209 paras 12.8-12.14
- ‘NHS to launch ground breaking online COVID-19 rehab service’, NHS England, 5 July 2020 (https://www.england.nhs.uk/2020/07/nhs-to-launch-ground-breaking-online-covid-19-rehab-service; INQ000205651); INQ000292628; INQ000274099
- INQ000272238
- INQ000280198_0008-0009 para 1.9
- See, for example, Christopher Brightling 13 October 2023 124/2
- INQ000251910_0009
- INQ000255836_0191-0192 para 657; see also Boris Johnson 7 December 2023 162/16-24; INQ000251910_0009; INQ000214216_0052
- Imran Shafi 30 October 2023
- INQ000251916
- INQ000251916_0003
- INQ000251916_0003
- INQ000280198_0031 para 7.4; see also INQ000251645_0207; INQ000269203_0135; INQ000273807_0169; INQ000238826_0203
- INQ000251645_0207
- See also INQ000251645_0207; INQ000269203_0135; INQ000273807_0169; INQ000238826_0203; INQ000280198_0031 para 7.4
- INQ000022537_0005 paras 2.1, 2.4
- INQ000022537_0005-0006 paras 2.6, 2.11
- R was estimated to be between 1.2 and 1.4 in England and Scotland, 1.0 and 1.4 in Wales, and 0.8 and 1.3 in Northern Ireland (see INQ000120627_0001 para 1)
- INQ000120627_0001 para 1
- INQ000120627_0002 para 9
- INQ000120627_0002 paras 11-14
- COVID-19 Response – Spring 2021, HM Government, February 2021, Executive summary (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087_0007)
- INQ000088958 See also INQ000198202 for meeting with the Covid-19 Taskforce earlier that day.
- ‘Vaccination programme accelerated as Step 4 is paused’, Prime Minister’s Office and Boris Johnson, 14 June 2021 (https://www.gov.uk/government/news/vaccination-programme-accelerated-as-step-4-is-paused; INQ000234938)
- INQ000146775_0008
- INQ000146775_0008; ‘Vaccination programme accelerated as Step 4 is paused’, Prime Minister’s Office and Boris Johnson, 14 June 2021 (https://www.gov.uk/government/news/vaccination-programme-accelerated-as-step-4-is-paused; INQ000234938)
- INQ000252914_0070 para 302; INQ000091961; INQ000146810; INQ000146775_0008-0009; INQ000217092_0006-0009
- See, for example, INQ000092509_0006
- ‘Vaccination programme accelerated as Step 4 is paused’, Prime Minister’s Office and Boris Johnson, 14 June 2021 (https://www.gov.uk/government/news/vaccination-programme-accelerated-as-step-4-is-paused; INQ000234938)
- INQ000088958_0008
- INQ000088958_0008
- INQ000212981; INQ000022540_0002 para 1.6; INQ000218171; INQ000218169
- INQ000022540_0002-0003 paras 1.4-1.5, 1.8; INQ000048533; INQ000357301; INQ000212981_0002 para 8
- INQ000357301_0005
- INQ000048534_0002
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 18 June 2021’, Scottish Government, 18 June 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-18-june-2021; INQ000353706)
- Andy Burnham 27 November 2023 127/4-128/9
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 22 June 2021’, Scottish Government, 22 June 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-22-june-2021; INQ000369676)
- INQ000243908
- INQ000174323
- INQ000088958_0008-0009
- INQ000120629. R was estimated to be between 1.2 and 1.5 in England, in Scotland and in Wales, and between 1.3 and 1.6 in Northern Ireland. It had not changed significantly in the preceding weeks.
- INQ000212984_0002 para 5
- INQ000212984_0002 para 5
- INQ000212984_0002 para 5
- INQ000048536; INQ000357302_0001
- Building Forward: Consolidated Covid-19 Recovery Plan, Northern Ireland Executive, July 2021 (https://www.executiveoffice-ni.gov.uk/topics/building-forward-consolidated-covid-19-recovery-plan; INQ000101002). It set out an action plan to promote recovery in areas including economic development, inequalities and health.
- INQ000247795_0024-0025
- INQ000247795_0021
- INQ000247795_0004
- COVID-19 Response: Summer 2021, HM Government, July 2021 (https://www.gov.uk/government/publications/covid-19-response-summer-2021-roadmap; INQ000180301)
- COVID-19 Response: Summer 2021, HM Government, July 2021 (https://www.gov.uk/government/publications/covid-19-response-summer-2021-roadmap; INQ000180301)
- The Technical Advisory Group’s advice on 9 July 2021 formally introduced a fifth harm from Covid-19: “harms arising from the way COVID-19 has exacerbated existing, or introduced new, inequalities in our society” (see Chapter 10: Vulnerabilities and inequalities, in Volume II).
- INQ000120629_0001 para 2
- The four major risks were: an increase in hospitalisations and deaths; more Long Covid; workforce absences (including in the NHS); and the increased risk of new variants emerging. (see INQ000120629_0001-0002 para 9).
- INQ000120629_0002
- INQ000120629_0002 para 12
- INQ000120629_0002 para 14
- INQ000120629_0002
- INQ000048537_0002
- INQ000048537_0005
- INQ000092214_0005
- Sajid Javid 29 November 2023 128/1-25, 131/7-22; INQ000273901_0614
- INQ000092214_0005, 0009. The four tests had been outlined in the spring 2021 roadmap: “a. The vaccine deployment programme continues successfully. b. Evidence shows vaccines are sufficiently effective in reducing hospitalisations and deaths in those vaccinated. c. Infection rates do not risk a surge in hospitalisations which would put unsustainable pressure on the NHS. c. [sic] Our assessment of the risks is not fundamentally changed by new Variants of Concern” (COVID-19 Response – Spring 2021, HM Government, February 2021, p4 (https://assets.publishing.service.gov.uk/media/6033cfdae90e076607c1bf18/COVID-19_Response_-_Spring_2021.pdf; INQ000185087_0008)).
- INQ000092214_0005, 0010
- ‘PM statement at coronavirus press conference: 12 July 2021’, Prime Minister’s Office and Boris Johnson, 12 July 2021 (https://www.gov.uk/government/speeches/pm-statement-at-coronavirus-press-conference-12-july-2021; INQ000086709)
- INQ000129973_0003 para 4.3
- INQ000129973_0003 para 4.4
- INQ000129973_0003 para 4.5
- Coronavirus Contral Plan: Alert Level Zero, Welsh Government, July 2021 (https://www.gov.wales/sites/default/files/publications/2021-09/coronavirus-control-plan-alert-level-zero-0.pdf; INQ000066070)
- INQ000129973_0003-0004 paras 4.8-4.11, 4.15
- INQ000214642_0003 para 12
- INQ000214642_0003 para 13
- Such as restricting gatherings outdoors to 15 people, 1 metre distancing indoors and a delay to live events of up to 200 people ( INQ000214642_0007-0008 para 24). See also ‘Level 0 from 19 July’, Scottish Government, 13 July 2021 (https://www.gov.scot/news/level-0-from-19-july; INQ000369713); ‘Covid restrictions ease as Scotland moves to level zero’, BBC News, 19 July 2021 (https://www.bbc.com/news/uk-scotland-57878745; INQ000357720); ‘Rangers granted permission for 17,000 fans at league opener with Livingston’, BBC News, 20 July 2021 (https://www.bbc.co.uk/sport/football/57901573; INQ000357832); INQ000214642_0003 para 14
- ‘Moving to Step 4 of the roadmap’, Cabinet Office, 27 August 2021 (https://www.gov.uk/government/publications/covid-19-response-summer-2021-roadmap/moving-to-step-4-of-the-roadmap; INQ000136725)
- INQ000273800_0044-0045 paras 130, 132; ‘Does 19 July really represent “Freedom Day” for people with MS?’, Multiple Sclerosis Trust, 8 July 2021 (https://mstrust.org.uk/news/stories/19-july-represent-freedom-day-people-ms; INQ000280373)
- For further information regarding the NHS COVID-19 app, see ‘Epidemiological impacts of the NHS COVID-19 app in England and Wales throughout its first year’, M. Kendell, D. Tsallis, C. Wymant, A. Di Franca, Y. Balogun, X. Didelot, et al., Nature Communications (2021), 14(858) (https://doi.org/10.1038/s41467-023-36495-z; INQ000575411); ‘NHS COVID-19 app launches across England and Wales’, Department of Health and Social Care, 24 September 2020 (https://www.gov.uk/government/news/nhs-covid-19-app-launches-across-england-and-wales; INQ000237570).
- INQ000092196_0006
- INQ000092856
- INQ000273901_0489. The report was considered in later Department of Health and Social Care and Covid-19 Taskforce contingency planning documents, for example, INQ000257037.
- COVID-19: Preparing for the Future. Looking Ahead to Winter 2021/22 and Beyond, The Academy of Medical Sciences, 15 July 2021 (https://acmedsci.ac.uk/file-download/4747802; INQ000387464)
- ‘COVID-19: Preparing for the future. Public summary’, The Academy of Medical Sciences, 15 July 2021 (https://acmedsci.ac.uk/file-download/38576298; INQ000591889)
- INQ000092555
- INQ000092058_0002 para 1(d)
- INQ000092226_0004; INQ000092555
- INQ000065680_0002 para 5
- INQ000065680_0002 para 6
- INQ000065680_0002 para 6
- INQ000065680_0002 para 5
- INQ000065680_0002-0003 para 9
- INQ000065680_0005
- INQ000236737; INQ000065584_0002 para 4
- INQ000065584_0002 para 4
- INQ000022545
- Coronavirus (COVID-19) Infection Survey (Positivity Estimates): 25 to 31 July 2021, Welsh Government, 6 August 2021 (https://www.gov.wales/coronavirus-covid-19-infection-survey-positivity-estimates-25-31-july-2021-html; INQ000548011)
- INQ000330424; INQ000065597_0011-0012 para 35
- INQ000066234
- INQ000238826_0144-0145 para 438
- INQ000207216_0004 para 13
- INQ000065680_0002 para 5
- INQ000207218_0009; INQ000357301_0005; INQ000048534_0002; INQ000212984_0002 para 5; INQ000048536; INQ000357302_0001; INQ000065680_0002, 0005; INQ000236737; INQ000065584_0002 para 4
- INQ000591920
- ‘Covid: Scotland tops Europe hotspot chart’, BBC News, 5 July 2021 (https://www.bbc.co.uk/news/uk-scotland-57712737; INQ000357759)
- INQ000624817
- ‘Covid: Scotland tops Europe hotspot chart’, BBC News, 5 July 2021 (https://www.bbc.co.uk/news/uk-scotland-57712737; INQ000357759_0003)
- INQ000214642_0003 para 11
- INQ000214642_0003 para 14
- INQ000233258_0005; INQ000334792_0006
- Building Resilience Together: NI Civil Contingencies Framework, The Executive Office, 10 August 2021 (https://www.executiveoffice-ni.gov.uk/publications/northern-ireland-civil-contingencies-framework; INQ000086922); INQ000438174_0176-0177 para 671
- INQ000205712_0001
- INQ000205712_0001
- INQ000286302_0001
- INQ000065675_0001
- INQ000065675; INQ000048540
- INQ000421321_0041-0042, 0053 paras 82, 110
- INQ000375741
- INQ000065672
- INQ000207223_0004 para 10
- INQ000249453_0011
- ‘Covid in Scotland: Cases doubling weekly after restrictions eased’, BBC News, 30 August 2021 (https://www.bbc.co.uk/news/uk-scotland-58383606; INQ000360053)
- This phase follows the ‘Route Map’ approach in place during mid-2020; and the ‘Levels’ approach implemented from November 2020 to August 2021 (INQ000273978_0096 para 385; INQ000078476).
- INQ000339033_0140 para 400; ‘Coronavirus (COVID-19) update: First Minister’s statement – 3 August 2021’, Scottish Government, 3 August 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-3-
august-2021-1; INQ000353731) - ‘Coronavirus (COVID-19) update: First Minister’s statement – 27 August 2021’, Scottish Government, 27 August 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-27-august-2021; INQ000353708)
- INQ000214565_0045; INQ000078614
- INQ000214641_0008; see also INQ000214563_0003 para 13(a)
- INQ000214735_0003-0004 paras 12, 17, 18
- Official Report: Meeting of the Parliament (Hybrid), The Scottish Parliament, 16 September 2021, Session 6, (https://www.parliament.scot/api/sitecore/CustomMedia/OfficialReport?meetingId=13300; INQ000548024)
- Coronavirus (COVID-19) Infection Survey, UK: 17 September 2021, Office for National Statistics, 17 September 2021 (https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/bulletins/coronaviruscovid19infectionsurveypilot/17september2021; INQ000548012); ‘Coronavirus (COVID-19): State of the epidemic’, Scottish Government, 24 September 2021 (https://www.gov.scot/publications/coronavirus-covid-19-state-epidemic-24-september-2021; INQ000626477)
- INQ000092120_0004
- INQ000092120_0006
- INQ000056330_0002
- INQ000056330_0004
- INQ000022547_0003 para 2.7
- INQ000090707_0001. Mr Drakeford announced the compulsory Covid-19 pass for a number of venues and reinforced the importance of working from home and face coverings (see INQ000090708).
- INQ000061603_0002 para 4
- INQ000061603_0003 para 12; INQ000253920_0002 para 10
- INQ000061603_0003 para 12
- INQ000253920_0001 para 2; INQ000061603_0003 paras 12-18
- INQ000061603_0002 para 2
- INQ000253920_0001 para 6
- INQ000252914_0070 paras 304-305
- INQ000198208_0001 para 4
- INQ000198208_0001 para 4
- INQ000092113; COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270); INQ000198217
- COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270)
- COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021, p6, para 7 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270)
- COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021, pp25-28, paras 85-88 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270)
- COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270)
- COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021, p23, para 73 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270)
- ‘JCVI statement regarding a COVID-19 booster vaccine programme for winter 2021 to 2022’, Joint Committee on Vaccination and Immunisation, 14 September 2021 (https://www.gov.uk/government/publications/jcvi-statement-september-2021-covid-19-booster-vaccine-programme-for-winter-2021-to-2022/jcvi-statement-regarding-a-covid-19-booster-vaccine-programme-for-winter-2021-to-2022; INQ000257044)
- Coronavirus Control Plan: Autumn and Winter 2021 Update, Welsh Government, October 2021 (https://www.gov.wales/sites/default/files/publications/2021-10/coronavirus-control-plan-autumn-and-winter-2021-update.pdf; INQ000082368)
- Coronavirus Control Plan: Autumn and Winter 2021 Update, Welsh Government, October 2021, p6 (https://www.gov.wales/sites/default/files/publications/2021-10/coronavirus-control-plan-autumn-and-winter-2021-update.pdf; INQ000082368)
- INQ000390618_0061-0062 para 185; INQ000350502_0002
- Coronavirus Control Plan: Autumn and Winter 2021 Update, Welsh Government, October 2021, p6 (https://www.gov.wales/sites/default/files/publications/2021-10/coronavirus-control-plan-autumn-and-winter-2021-update.pdf; INQ000082368)
- Coronavirus Control Plan: Autumn and Winter 2021 Update, Welsh Government, October 2021, pp34-35 (https://www.gov.wales/sites/default/files/publications/2021-10/coronavirus-control-plan-autumn-and-winter-2021-update.pdf; INQ000082368)
- INQ000065667
- NI Executive Autumn/Winter COVID-19 Contingency Plan, Northern Ireland Executive, October 2021 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/autumn-winter-covid-19-contingency-plan-2021.PDF; INQ000104468_0003)
- INQ000438174_0164 para 605
- COVID-19: Scotland’s Strategic Framework Update, Scottish Government, June 2021 (https://www.gov.scot/publications/coronavirus-covid-19-scotlands-strategic-framework-update-june-2021; INQ000235137)
- The Scottish Government published specific plans for winter preparedness for the health and social care sector in October 2021: Health and Social Care Winter Overview 2021-2022, Scottish Government, 22 October 2021 (https://www.gov.scot/publications/scottish-government-health-social-care-winter-overview-2021-22/documents; INQ000492663); Adult Social Care Winter Preparedness Plan 2021-22, Scottish Government, 22 October 2021 (https://www.gov.scot/publications/adult-social-care-winter-preparedness-plan-2021-22; INQ000280634).
- Covid Recovery Strategy: For a Fairer Future, Scottish Government, 5 October 2021, p3 (https://www.gov.scot/publications/covid-recovery-strategy-fairer-future; INQ000131075)
- Covid Recovery Strategy: For a Fairer Future, Scottish Government, 5 October 2021, p4 (https://www.gov.scot/publications/covid-recovery-strategy-fairer-future; INQ000131075)
- Covid Recovery Strategy: For a Fairer Future, Scottish Government, 5 October 2021, p4 (https://www.gov.scot/publications/covid-recovery-strategy-fairer-future; INQ000131075)
- John Swinney 30 January 2024 99/8-13
- INQ000061604
- INQ000061604_0002
- INQ000061604_0002 para 4
- INQ000061604_0005 para 31
- INQ000128600_0001 para 1
- INQ000238826_0147 para 446
- INQ000064175
- INQ000064175
- INQ000236362_0001
- INQ000022553; see also INQ000350062
- ‘Written Statement: Review of the Health Protection (Coronavirus Restriction) (No. 5) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 29 October 2021 (https://www.gov.wales/written-statement-review-health-protection-coronavirus-restriction-no5-wales-regulations-2020-15; INQ000023302_0002)
- ‘UK: Daily new confirmed COVID-19 cases per 100,000, Oct 31, 2021’, Our World in Data, 31 October 2021 (https://ourworldindata.org/grapher/uk-daily-covid-cases-7day-average?tab=discrete-bar&time=2021-10-31&country=Scotland~England~Wales~Northern+Ireland; INQ000548394)
- INQ000396876_0008 Figure 1; INQ000022553_0002; INQ000249453_0011; INQ000048537_0002; ‘UK: Daily new confirmed COVID-19 deaths’, Our World in Data, 31 October 2021 (https://ourworldindata.org/grapher/uk-daily-covid-deaths?time=earliest..2021-10-31&country=Northern+Irelan~Wales~England~Scotland~Northern+Ireland; INQ000548396); ‘UK: Daily new confirmed COVID-19 cases per 100,000’, Our World in Data, 1 August to 31 October 2021 (https://ourworldindata.org/grapher/uk-daily-covid-cases-7day-average?time=2021-08-01..2021-10-31; INQ000548393)
- INQ000065228_0048 Figure 15; INQ000065602_0007 para 21
- INQ000370347_0057 para 117; ‘Covid-19 booster vaccinations underway’, Scottish Government, 20 September 2021 (https://www.gov.scot/news/covid-19-booster-vaccinations-underway; INQ000548017); ‘Covid-19 vaccines for over-12s and boosters for over 50s’, BBC News, 14 September 2021 (https://www.bbc.co.uk/news/uk-northern-ireland-58555665; INQ000548019); ‘Covid Wales: Go-ahead for boosters and jabs for 12-15 year olds’, BBC News, 14 September 2021 (https://www.bbc.co.uk/news/uk-wales-politics-58557120; INQ000548016); ‘Covid booster vaccine rollout to begin across UK next week’, BBC News, 14 September 2021 (https://www.bbc.co.uk/news/health-58550833; INQ000548014)
- INQ000092120_0004, 0006; INQ000421704_0228 para 493; Official Report: Meeting of the Parliament (Hybrid), The Scottish Parliament, 16 September 2021, Session 6 (https://www.parliament.scot/api/sitecore/CustomMedia/OfficialReport?meetingId=13300; INQ000548024); INQ000090707_0001
- INQ000198208_0001 para 4
- ‘Written Statement: Review of the Health Protection (Coronavirus Restriction) (No. 5) (Wales) Regulations 2020’, Welsh Government, 29 October 2021 (https://www.gov.wales/written-statement-review-health-protection-coronavirus-restriction-no5-wales-regulations-2020-15; INQ000023302)
- NI Executive Autumn/Winter COVID-19 Contingency Plan, Northern Ireland Executive, October 2021 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/autumn-winter-covid-19-contingency-plan-2021.PDF; INQ000104468)
- NI Executive Autumn/Winter COVID-19 Contingency Plan, Northern Ireland Executive, October 2021 (https://www.executiveoffice-ni.gov.uk/sites/default/files/publications/execoffice/autumn-winter-covid-19-contingency-plan-2021.PDF; INQ000104468)
- INQ000092856_0005 para 42
- INQ000233716
- INQ000120655_0001 para 4; INQ000120658_0001 para 1
- ‘First UK cases of Omicron variant identified’, Department of Health and Social Care, 27 November 2021 (https://www.gov.uk/government/news/first-uk-cases-of-omicron-variant-identified; INQ000237598)
- ‘Covid-19: Boosters advised for all adults and masks back in shops’, BBC News, 29 November 2021 (https://www.bbc.co.uk/news/uk-59465127; INQ000357726_0003)
- INQ000421714_0002 para 10; INQ000371645_0042 para 158
- INQ000283367_0006
- INQ000283367_0003
- See UK Health Security Agency Covid-19 data dashboard archive (https://ukhsa-dashboard.data.gov.uk/covid-19-archive-data-download).
- INQ000119424; INQ000074374
- INQ000273901_0529
- INQ000119424
- INQ000119424_0006 para 18
- INQ000119424; INQ000074374. Other actions included early detection, containment measures, acceleration of the booster vaccination campaign, antivirals, more work on understanding the characteristics and preparation of countermeasures (vaccines and antibodies).
- INQ000092222_0005
- INQ000092222_0006
- INQ000092222_0010
- Sajid Javid 29 November 2023 146/19-23
- INQ000273901_0529
- INQ000092196_0001-0003; INQ000185095
- ‘PM opening statement at COVID-19 press conference: 27 November 2021’, Prime Minister’s Office and Boris Johnson, 27 November 2021 (https://www.gov.uk/government/speeches/pm-opening-statement-at-covid-19-press-conference-27-november-2021; INQ000055627)
- INQ000092196_0004-0005
- INQ000092196_0007; ‘PM opening statement at COVID-19 press conference: 27 November 2021’, Prime Minister’s Office and Boris Johnson, 27 November 2021 (https://www.gov.uk/government/speeches/pm-opening-statement-at-covid-19-press-conference-27-november-2021; INQ000055627_0003)
- INQ000185095
- ‘PM opening statement at COVID-19 press conference: 27 November 2021’, Prime Minister’s Office and Boris Johnson, 27 November 2021 (https://www.gov.uk/government/speeches/pm-opening-statement-at-covid-19-press-conference-27-november-2021; INQ000055627)
- INQ000334923_0027
- INQ000334923_0027
- INQ000334923_0027
- INQ000249371
- INQ000064245; INQ000230814; INQ000230792; INQ000230793
- INQ000061605_0003 para 12
- INQ000061605_0003 para 14
- INQ000061605_0003 para 15
- INQ000130006
- ‘PM opening statement at COVID-19 press conference: 30 November 2021’, Prime Minister’s Office and Boris Johnson, 30 November 2021 (https://www.gov.uk/government/speeches/pm-opening-statement-at-covid-19-press-conference-30-november-2021; INQ000086803)
- INQ000089099_0001
- INQ000089099_0008
- INQ000089099_0008
- INQ000089099_0008
- ‘Exclusive: Boris Johnson “broke Covid lockdown rules” with Downing Street parties at Xmas’, The Mirror, 30 November 2021 (https://www.mirror.co.uk/news/politics/boris-johnson-broke-covid-lockdown-25585238; INQ000548386)
- INQ000214473_0004 para 13
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 30 November 2021’, Scottish Government, 30 November 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-30-november-2021; INQ000353733_0004-0005); ‘Omicron variant’, Scottish Government, 29 November 2021 (https://www.gov.scot/news/omicron-variant; INQ000584994)
- INQ000218226_0002
- INQ000236761_0004
- INQ000092227_0001-0004
- INQ000092192_0002
- INQ000088914_0002
- INQ000120655
- INQ000120655_0002 para 3
- INQ000120655_0001 para 9
- INQ000120655_0002 para 1
- INQ000214474_0008-0009 para 29
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 7 December 2021’, Scottish Government, 7 December 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-statement-7-december-2021; INQ000353736)
- INQ000217015
- INQ000217015_0003
- INQ000217015_0018-0019, 0023
- INQ000217015_0025-0026
- INQ000217015_0004
- Sajid Javid 29 November 2023 150/20-151/20
- INQ000217015_0008
- INQ000217015_0009
- INQ000217015_0011
- INQ000217015_0011
- INQ000185093_0003
- INQ000185093_0006
- INQ000185093_0006
- INQ000185093_0006
- INQ000185093_0006
- INQ000185093_0006
- INQ000185093_0006
- INQ000092202_0005
- INQ000092202_0006
- INQ000092202_0012
- INQ000092202_0012-0013
- INQ000092194
- INQ000088915
- INQ000088915
- INQ000088915
- INQ000092202_0006-0007
- INQ000273901_0540
- INQ000273901_0540
- ‘Prime Minister confirms move to Plan B in England’, Prime Minister’s Office and Boris Johnson, 8 December 2021 (https://www.gov.uk/government/news/prime-minister-confirms-move-to-plan-b-in-england; INQ000049258)
- ‘Prime Minister confirms move to Plan B in England’, Prime Minister’s Office and Boris Johnson, 8 December 2021 (https://www.gov.uk/government/news/prime-minister-confirms-move-to-plan-b-in-england; INQ000049258_0002)
- INQ000271796_0006 para 1.1
- Eluned Morgan 12 March 2024 42/23-24
- INQ000271796_0002 para 1.5
- INQ000271796_0002 para 1.6. Test, Trace, Protect was the Welsh Government’s service to track and prevent Covid-19, primarily through testing and contact tracing.
- INQ000271796_0004 para 3.11
- INQ000271796_0004 para 3.10; INQ000057958_0004 para 11
- INQ000269147_0001; INQ000421704_0229 para 495
- INQ000207229_0002
- ‘Public Health Scotland urges public to defer Christmas parties’, Public Health Scotland, 9 December 2021 (https://publichealthscotland.scot/news/2021/december/public-health-scotland-urges-public-to-defer-christmas-parties; INQ000274186)
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 10 December 2021’, Scottish Government, 10 December 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-10-december-2021; INQ000353715)
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 10 December 2021’, Scottish Government, 10 December 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-10-december-2021; INQ000353715)
- ‘Coronavirus (COVID-19) update: First Minister’s statement – 10 December 2021’, Scottish Government, 10 December 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-10-december-2021; INQ000353715)
- INQ000256922; INQ000256925; Sajid Javid 29 November 2023 103/24-104/18
- INQ000083854_0003 paras 2-3, 5
- INQ000083854_0003 para 5
- INQ000083854_0003-0004 paras 5-7
- INQ000090717
- INQ000327548_0079
- ‘UK coronavirus (COVID-19) alert level increased from Level 3 to Level 4’, Department of Health and Social Care, 12 December 2021 (https://www.gov.uk/government/news/uk-coronavirus-covid-19-alert-level-increased-from-level-3-to-level-4; INQ000237425)
- INQ000088916
- INQ000088916_0001
- INQ000088916_0001
- INQ000354766; INQ000089006_0004-0005; ‘Urgent Omicron appeal: Get boosted now’, Prime Minister’s Office and Boris Johnson, 12 December 2021 (https://www.gov.uk/government/news/urgent-omicron-appeal-get-boosted-now; INQ000086635)
- INQ000088916_0001
- INQ000088916_0001
- INQ000088916_0001
- INQ000088916_0002
- INQ000089006_0004-0005
- INQ000089008_0008-0014
- INQ000089008_0010
- INQ000089008_0010
- INQ000089008_0010
- INQ000089008_0010
- INQ000089008_0011
- INQ000089008_0012
- INQ000089008_0008-0014
- INQ000089008_0013
- INQ000089008_0013
- INQ000255836_0184-0185 para 633; ‘As it happened: Covid passes become law in England despite Tory rebellion’, BBC News, 14 December 2021 (https://www.bbc.co.uk/news/live/uk-politics-59651187; INQ000548009)
- ‘Covid: New Plan B rules on working from home and masks announced for England’, BBC News, 8 December 2021 (https://www.bbc.co.uk/news/uk-59585307; INQ000548020); ‘COVID-19 press conference (8 December 2021)’, YouTube, 8 December 2021 (https://www.youtube.com/watch?v=87aIf4opgts; INQ000548291)
- ‘UK Government confirms £430 million funding for devolved administrations to tackle Covid’, HM Treasury, 14 December 2021 (https://www.gov.uk/government/news/uk-government-to-confirm-extra-funding-for-devolved-administrations-to-tackle-covid; INQ000548036). For Scotland, this doubled to £440 million on 19 December (INQ000215484_0015-0016 para 53). For Wales, this doubled to £270 million on 20 December (INQ000321085_0001-0002 para 5). For Northern Ireland, this doubled to £150 million (INQ000304512_0002).
- INQ000083855_0004-0005 para 4
- INQ000228013_0002
- INQ000083855_0005
- INQ000083855_0004-0005
- INQ000231045
- INQ000231045
- INQ000231045
- INQ000231045
- INQ000104595_0004; INQ000120660_0001 para 6
- INQ000228013_0002
- INQ000057972
- INQ000057972
- INQ000548018
- INQ000057972_0008
- INQ000057972_0012
- INQ000048551_0003 para 9
- INQ000355166
- ‘Limiting the spread of Omicron’, Scottish Government, 16 December 2021 (https://www.gov.scot/news/limiting-the-spread-of-omicron; INQ000548023)
- ‘Coronavirus (COVID-19) update: First Minister’s speech – 17 December 2021’, Scottish Government, 17 December 2021 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-17-december-2021; INQ000353701_0003)
- INQ000057970_0002para 1.6. Health boards were reporting a “relatively stable situation“; however, there were “850 more beds occupied at this stage than the same time the previous year” (INQ000057970_0003 para 1.10).
- INQ000057970_0004 para 1.16
- INQ000057970_0004 paras 1.20-1.21
- INQ000057970_0003 para 1.12
- INQ000057970_0003 para 1.13
- ‘Written Statement: Review of the Health Protection (Coronavirus Restriction) (No. 5) (Wales) Regulations 2020’, Mark Drakeford, First Minister, Welsh Government, 17 December 2021 (https://www.gov.wales/written-statement-review-health-protection-coronavirus-restrictions-no5-wales-regulations-2020; INQ000023305)
- INQ000321085_0002 para 5
- INQ000120658
- INQ000120658_0001 para 1
- INQ000120658_0001 para 6
- INQ000120658_0002 para 8
- INQ000251921
- INQ000104595_0001
- INQ000104595_0004
- INQ000104595_0004
- INQ000104595_0005
- INQ000104595_0006
- INQ000104595_0009
- INQ000104595_0005
- INQ000249362_0001
- INQ000083852_0005
- INQ000083852_0001-0002
- INQ000251920; INQ000251921; INQ000255836_0185 para 636
- INQ000255836_0186 para 638
- INQ000255836_0186 para 638
- INQ000184558_0001; INQ000263374_0141-0142 paras 526-528
- INQ000263374_0142 para 529
- INQ000273901_0556
- INQ000120660_0001 para 6
- INQ000120660_0002 para 11
- INQ000217347_0001
- INQ000088918_0015
- INQ000088918_0021
- INQ000217347_0005
- INQ000217347_0007
- INQ000217347_0007
- INQ000217347_0007
- INQ000217347_0008
- INQ000057982; INQ000023306
- INQ000214475_0004-0005 paras 23-24
- INQ000214475_0008 para 34(d)
- INQ000214475_0005 para 26
- INQ000214475_0005 para 30
- INQ000257218
- INQ000207230_0002 para 2; INQ000421704_0231 para 500
- INQ000065662_0006-0007 paras 14, 19
- INQ000207230_0006-0007; INQ000065662_0002 para 7
- INQ000438174_0180 para 684
- INQ000120661_0001 para 1
- INQ000120661_0001 para 5
- INQ000120661_0002 para 13
- INQ000120661_0002 para 15
- INQ000074640_0001
- INQ000074640_0001
- INQ000340401_0001
- INQ000340401_0001
- INQ000340401_0001
- INQ000074640_0002
- INQ000238826_0155 para 462
- INQ000064366
- Sajid Javid 29 November 2023 148/17-150/24; INQ000273901_0569, 0618; see, for example, INQ000251921. Mr Javid was also not invited to a meeting on 18 December 2021 (INQ000273901_0555).
- Boris Johnson 7 December 2023 69/13-25; INQ000251924_0007; INQ000255836_0187 para 641
- INQ000238826_0150-0151 para 454
- INQ000238826_0150-0151 para 454
- INQ000238826_0150-0151 para 454
- INQ000421704_0229-0230 para 496
- INQ000255836_0182-0183 para 627
- INQ000263374_0142 para 529
- Frank Atherton 4 March 2024 57/2-19
- INQ000251645_0161 para 8.115
- INQ000236456; INQ000236457
- INQ000369765_0063 para 371
- ‘Coronavirus (COVID-19): Modelling the epidemic in Scotland (issue no. 88)’, Scottish Government, 3 February 2022 (https://www.gov.scot/publications/coronavirus-covid-19-modelling-epidemic-issue-no-88/documents; INQ000369763); INQ000369765_0064 para 376
- INQ000083855_0004 para 4
- INQ000334792_0049
- INQ000346395_0034 para 106
- INQ000091584_0001
- INQ000088948_0006
- ‘PM statement to the House of Commons on COVID-19: 5 January 2022’, Prime Minister’s Office and Boris Johnson, 5 January 2022 (https://www.gov.uk/government/speeches/pm-statement-to-the-house-of-commons-on-covid-19-5-january-2022; INQ000086671_0003)
- INQ000120662
- INQ000120662_0002 para 4
- INQ000057923_0002 paras 3.2-3.3
- INQ000057923_0002 para 3.5
- INQ000057924
- INQ000057924_0003 para 1.10
- These events required at least 50% of the crowd to be checked for vaccine certificates. See ‘Large outdoor events resume from 17 January’, Scottish Government, 11 January 2022 (https://www.gov.scot/news/large-outdoor-events-resume-from-17-january; INQ000369712).
- ‘Omicron measures to be lifted’, Scottish Government, 18 January 2022 (https://www.gov.scot/news/omicron-measures-to-be-lifted; INQ000584993)
- INQ000048555_0002
- INQ000048555_0007
- COVID-19 Response: Autumn and Winter Plan 2021, HM Government, September 2021 (https://www.gov.uk/government/publications/covid-19-response-autumn-and-winter-plan-2021/covid-19-response-autumn-and-winter-plan-2021; INQ000137270); ‘England returns to Plan A as regulations on face coverings and COVID passes change today’, Department of Health and Social Care and Sajid Javid, 27 January 2022 (https://www.gov.uk/government/news/england-returns-to-plan-a-as-regulations-on-face-coverings-and-covid-passes-change-today; INQ000257262)
- INQ000120665
- INQ000089038_0004-0007
- ‘Covid in Scotland: Rules on distancing and face masks relaxed further’, BBC News, 28 January 2022 (https://www.bbc.co.uk/news/uk-scotland-60159431; INQ000357658)
- INQ000421714_0012 para 42; Ministerial Code, Northern Ireland Executive, 6 April 2006 (https://www.northernireland.gov.uk/publications/northern-ireland-executive-ministerial-code; INQ000262764)
- INQ000271068
- INQ000438259; The Health Protection (Coronavirus, Restrictions, Wearing of Face Coverings) (Revocation) Regulations (Northern Ireland) 2022 (https://www.legislation.gov.uk/nisr/2022/47/contents/made); The Health Protection (Coronavirus, Restrictions) Regulations (Northern Ireland) 2021 (revoked) (https://www.legislation.gov.uk/nisr/2021/93/content); The Health Protection (Coronavirus, Wearing of Face Coverings) Regulations (Northern Ireland) 2020 in their entirety (https://www.legislation.gov.uk/nisr/2020/164/contents/made)
- INQ000022568_0002 para 3.5
- INQ000022568_0003 para 3.8
- ‘PM statement on living with COVID: 21 February 2022’, Prime Minister’s Office and Boris Johnson, 21 February 2022 (https://www.gov.uk/government/speeches/pm-statement-on-living-with-covid-21-february-2022; INQ000237518); COVID-19 Response: Living with COVID-19, HM Government, February 2022 (https://www.gov.uk/government/publications/covid-19-response-living-with-covid-19; INQ000086652)
- COVID-19 Response: Living with COVID-19, HM Government, February 2022, para 20 (https://www.gov.uk/government/publications/covid-19-response-living-with-covid-19; INQ000086652_0012)
- INQ000302485_0040-0041 paras 124-126
- INQ000273901_0571
- INQ000302485_0040-0041 paras 124-126
- INQ000198233; INQ000198234
- INQ000198238
- ‘PM statement at Covid press conference: 21 February 2022’, Prime Minister’s Office and Boris Johnson, 21 February 2022 (https://www.gov.uk/government/speeches/pm-statement-at-covid-press-conference-21-february-2022; INQ000281415)
- ‘Coronavirus (COVID-19) update: First Minister’s speech – 22 February 2022’, Scottish Government, 22 February 2022 (https://www.gov.scot/publications/coronavirus-covid-19-update-first-ministers-speech-tuesday-22-february-2022; INQ000353698)
- COVID-19: Scotland’s Strategic Framework Update, Scottish Government, February 2022 (https://www.gov.scot/publications/coronavirus-covid-19-scotlands-strategic-framework-update-february-2022/documents; INQ000147446)
- Coronavirus (COVID-19) Strategic Framework Update February 2022: Equalities and Fairer Scotland Impact Assessment (EQFSIA), Scottish Government, February 2022 (https://www.gov.scot/publications/coronavirus-covid-19-strategic-framework-update-february-2022-equalities-fairer-scotland-impact-assessment-eqfsia/pages/4; INQ000147453); INQ000273978_0149 para 596
- Together for a Safer Future: Wales’ Long-Term COVID-19 Transition from Pandemic to Endemic, Welsh Government, March 2022 (https://www.gov.wales/wales-long-term-covid-19-transition-pandemic-endemic; INQ000066072)
- Together for a Safer Future: Wales’ Long-Term COVID-19 Transition from Pandemic to Endemic, Welsh Government, March 2022 (https://www.gov.wales/wales-long-term-covid-19-transition-pandemic-endemic; INQ000066072_0003)
- Together for a Safer Future: Wales’ Long-Term COVID-19 Transition from Pandemic to Endemic, Welsh Government, March 2022 (https://www.gov.wales/wales-long-term-covid-19-transition-pandemic-endemic; INQ000066072_0007)
- ‘Coronavirus (COVID-19): State of the epidemic – 18 March 2022’, Scottish Government, 18 March 2022 (https://www.gov.scot/publications/coronavirus-covid-19-state-epidemic-18-march-2022/documents; INQ000350991_0004)
- INQ000214481_0002-0003 paras 7, 9, 11
- ‘Covid in Scotland: Hospital patient numbers highest in 13 months’, BBC News, 10 March 2022 (https://www.bbc.co.uk/news/uk-scotland-60698453; INQ000548015)
- ‘Coronavirus (COVID-19): State of the epidemic – 18 March 2022’, Scottish Government, 18 March 2022 (https://www.gov.scot/publications/coronavirus-covid-19-state-epidemic-18-march-2022/documents; INQ000350991_0002)
- INQ000214482_0003 para 9
- ‘Update on COVID regulations’, Scottish Government, 15 March 2022 (https://www.gov.scot/news/update-on-covid-regulations; INQ000131013)
- ‘Update on COVID-19 regulations’, Scottish Government, 30 March 2022 (https://www.gov.scot/news/update-on-covid-19-regulations; INQ000326404)
- INQ000058010_0002 para 1.4
- INQ000130049_0003 para 2.4
- INQ000130049_0004 paras 2.7, 2.9, 2.10
- INQ000591920
- ‘New “stay at home” guidance published’, Scottish Government, 28 April 2022 (https://www.gov.scot/news/new-stay-at-home-guidance-published; INQ000370957)
- INQ000022580
- INQ000274150_0015
- INQ000215495_0042 para 164; Roger Halliday 17 January 2024 157/18
- INQ000215495_0042 para 164; INQ000215470_0012-0013 para 46
- INQ000391115_0051-0055 paras 206-214
- Coronavirus Control Plan: Autumn and Winter 2021 Update, Welsh Government, October 2021, pp6, 28 (https://www.gov.wales/sites/default/files/publications/2021-10/coronavirus-control-plan-autumn-and-winter-2021-update.pdf; INQ000082368)